

Treatment-General
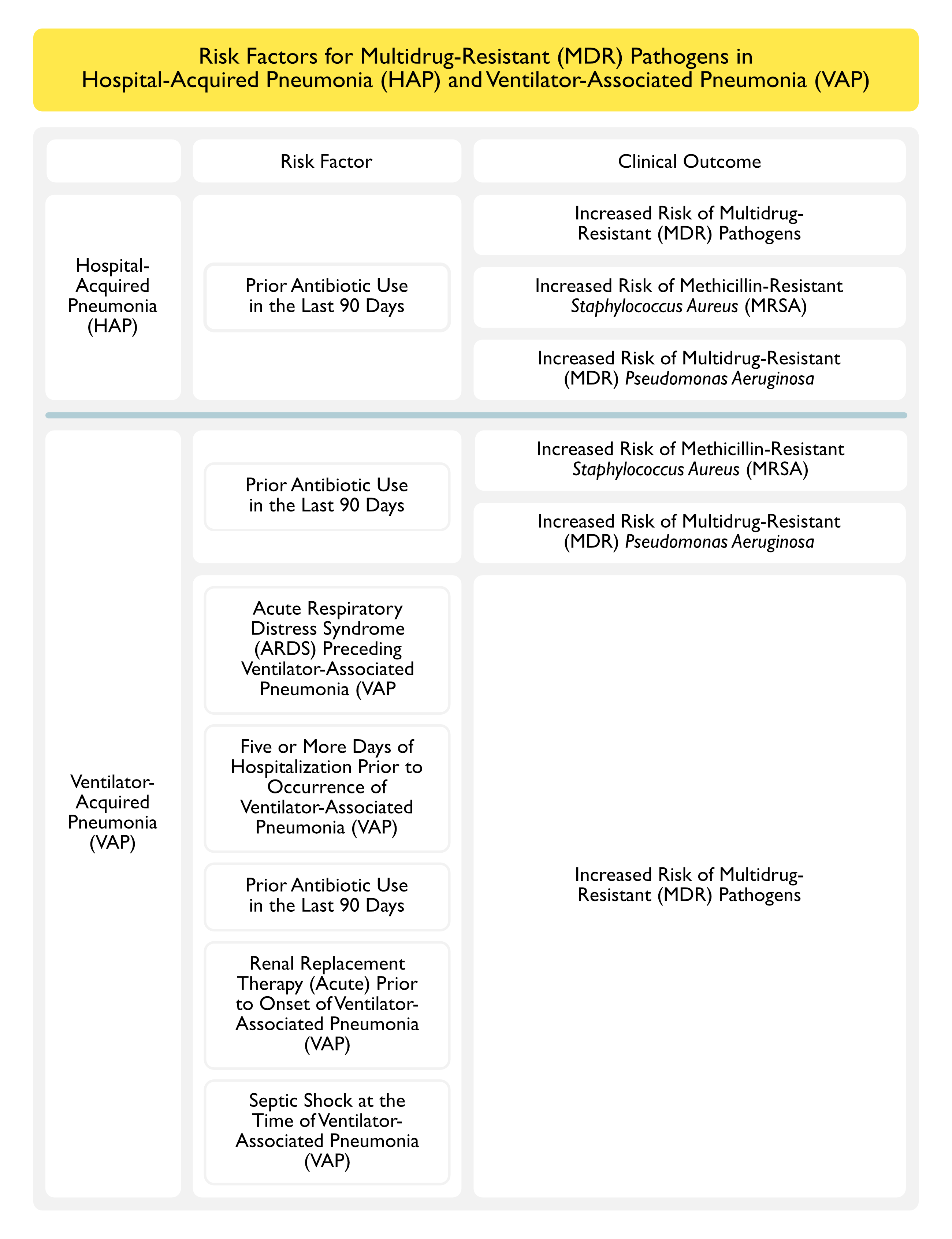
Risk Factors for Multidrug-Resistant Pathogens in Hospital-Acquired Pneumonia (HAP) and Ventilator-Associated Pneumonia (VAP) (Clin Infect Dis, 2016) [MEDLINE]

Treatment of Hospital Acquired Pneumonia (HAP)
General Comments
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
- All Hospitals Should Regularly Generate and Distribute an Antibiogram (Particularly One Which is Specific for Hospital Population)
Antibiotic Treatment Based on Empiric Coverage vs Based on Microbiologic Studies
Recommendations *Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
- Patients with HAP Should Be Treated Based on Results of Non-Invasively Obtained Microbiologic Studies, Rather than Being Treated Empirically (Weak Recommendation, Very Low Quality Evidence)
- Non-Invasive Sampling Methods
- Sputum Expectoration
- Sputum Induction
- Nasotracheal Suctioning
- Non-Invasive Sampling Methods
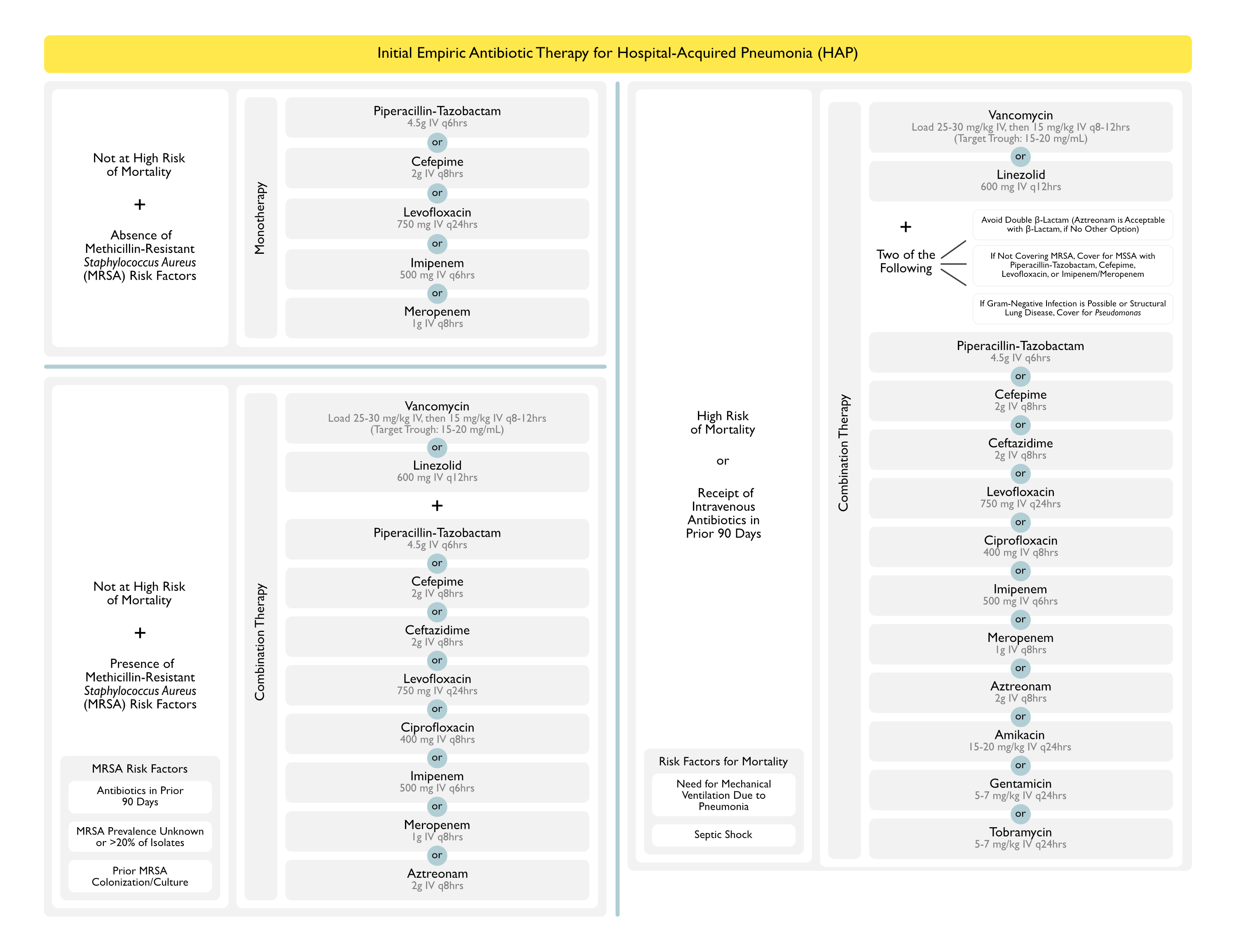
Empiric Antibiotics for Hospital-Acquired Pneumonia (HAP) (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
General Comments
- Choose One Agent with Activity Against Either Methicillin-Sensitive Staphylococcus Aureus (MSSA) or Methicillin-Resistant Staphylococcus Aureus (MRSA) + One/Two Agent with Activity Against Pseudomonas Aeruginosa (and Other Gram-Negatives) (Strong Recommendation, Very Low-Quality Evidence)
- If MRSA Coverage is Not Required, One the Following Agents is Suggested for Empiric MSSA Coverage (Weak Recommendation, Very Low-Quality Evidence): although nafcillin/oxacillin/cefazolin are recommended for proven MSSA, they are not required for empiric HAP coverage if one of the following agents are used (Weak Recommendation, Very Low-Quality Evidence)
- Cefepime (Maxipime) (see Cefepime)
- Imipenem (Primaxin) (see Imipenem)
- Meropenem (Merrem) (see Meropenem)
- Levofloxacin (Levaquin) (see Levofloxacin)
- Piperacillin-Tazobactam (Zosyn) (see Piperacillin-Tazobactam)
- Indications for MRSA Coverage in Empiric HAP Therapy (Weak Recommendation, Very Low-Quality Evidence)
- High Risk for Mortality
- Need for Ventilatory Support (Due to the HAP)
- Septic Shock
- Presence of Local Staphylococcus Aureus Methicillin-Resistance Rate >20% (or Where Resistance Rate is Unknown)
- Prior Intravenous Antibiotic Use in the Last 90 Days
- High Risk for Mortality
- Empiric HAP Coverage Should Include Coverage of Pseudomonas Aeruginosa and Other Gram-Negatives (Strong Recommendation, Very Low-Quality Evidence)
- Indications for Double-Coverage of Pseudomonas Aeruginosa in Empiric HAP Therapy (Weak Recommendation, Very Low-Quality Evidence)
- High Risk for Mortality
- Need for Ventilatory Support (Due to the HAP)
- Septic Shock
- Intravenous Antibiotics in the Last 90 Days
- High Risk for Mortality
- In Empiric Treatment of HAP, Avoid Using Aminoglycosides as the Sole Anti-Pseudomonal Agent (Strong Recommendation, Very Low-Quality Evidence): due to their poor lung penetration, risk of nephrotoxicity, risk of ototoxicity, and poorer clinical response rates (but no difference in mortality rate) as compared to other agents in the treatment of VAP (recommendations are based on extrapolation from the VAP data)
- Dosing of Antibiotics in HAP/VAP Should Be Determined Using Pharmacokinetic/Pharmacodynamic Data (Using Blood Antibiotic Concentrations, Extended and Continuous Infusions, Weight-Based Dosing for Certain Antibiotics, etc) Rather than the Manufacturer’s Prescribing Recommendations (Weak Recommendation, Very Low-Quality Evidence)
- If MRSA Coverage is Not Required, One the Following Agents is Suggested for Empiric MSSA Coverage (Weak Recommendation, Very Low-Quality Evidence): although nafcillin/oxacillin/cefazolin are recommended for proven MSSA, they are not required for empiric HAP coverage if one of the following agents are used (Weak Recommendation, Very Low-Quality Evidence)
Absence of Factors Imparting High Risk for Mortality (Need for Ventilatory Support, Septic Shock) and Absence of Factors Increasing the Likelihood of Methicillin-Resistant Staphylococcus Aureus (MRSA) (Local MRSA Rate >20% or Rate Unknown, Intravenous Antibiotics in Last 90 Days)
- General Comments
- Factors Imparting High-Risk for Mortality: absence of need for ventilatory support due to pneumonia and septic shock
- Factors Increasing the Likelihood of Methicillin-Resistant Staphylococcus Aureus (MRSA)
- Presence of Local Staphylococcus Aureus Methicillin-Resistance Rate >20% (or Where Resistance Rate is Unknown)
- Prior Intravenous Antibiotic Use in the Last 90 Days
- One of the Following
- Anti-Pseudomonal Penicillins (see Penicillins)
- Piperacillin-Tazobactam (Zosyn) (see Piperacillin-Tazobactam): 4.5 g IV q6hrs
- Anti-Pseudomonal Cephalosporins (see Cephalosporins)
- Cefepime (Maxipime) (see Cefepime): 2 g IV q8hrs
- Ceftazidime (Fortaz) (see Ceftazidime): 2 g IV q8hrs
- Carbapenems (see Carbapenems)
- Fluoroquinolones (see Fluoroquinolones)
- Levofloxacin (Levaquin) (see Levofloxacin): 750 mg IV q24hrs
- Anti-Pseudomonal Penicillins (see Penicillins)
Absence of Factors Imparting High Risk for Mortality (Need for Ventilatory Support, Septic Shock), But Presence of Factors Increasing the Likelihood of Methicillin-Resistant Staphylococcus Aureus (MRSA) (Local MRSA Rate >20% or Rate Unknown, Intravenous Antibiotics in Last 90 Days)
- One of the Following (Strong Recommendation, Moderate-Quality Evidence)
- Oxazolidinones
- Linezolid (Zyvox) (see Linezolid): 600 mg IV q12hrs
- Glycopeptides
- Vancomycin (see Vancomycin): consider load of 25-30 mg/kg IV for severe illness, then 15 mg/kg IV q8-12 hrs with target trough 15-20 mg/mL
- Oxazolidinones
- One of the Following
- Anti-Pseudomonal Penicillins (see Penicillins)
- Piperacillin-Tazobactam (Zosyn) (see Piperacillin-Tazobactam): 4.5 g IV q6hrs
- Anti-Pseudomonal Cephalosporins (see Cephalosporins)
- Cefepime (Maxipime) (see Cefepime): 2 g IV q8hrs
- Ceftazidime (Fortaz) (see Ceftazidime): 2 g IV q8hrs
- Carbapenems (see Carbapenems)
- Fluoroquinolones (see Fluoroquinolones)
- Ciprofloxacin (Cipro) (see Ciprofloxacin): 400 mg IV q8hrs
- Levofloxacin (Levaquin) (see Levofloxacin): 750 mg IV q24hrs
- Monobactams
- Aztreonam (Azactam) (see Aztreonam): 2 g IV q8hrs
- Anti-Pseudomonal Penicillins (see Penicillins)
Factors Imparting High Risk for Mortality (Need for Ventilatory Support, Septic Shock) or Receipt of Intravenous Antibiotics Within the Prior 90 Days
- One of the Following (Strong Recommendation, Moderate-Quality Evidence)
- Oxazolidinones
- Linezolid (Zyvox) (see Linezolid): 600 mg IV q12hrs
- Glycopeptides
- Vancomycin (see Vancomycin): consider load of 25-30 mg/kg IV for severe illness, then 15 mg/kg IV q8-12 hrs with target trough 15-20 mg/mL
- Oxazolidinones
- Two of the Following: avoid two β-lactams
- Anti-Pseudomonal Penicillins (see Penicillins)
- Piperacillin-Tazobactam (Zosyn) (see Piperacillin-Tazobactam): 4.5 g IV q6hrs
- Anti-Pseudomonal Cephalosporins (see Cephalosporins)
- Cefepime (Maxipime) (see Cefepime): 2 g IV q8hrs
- Ceftazidime (Fortaz) (see Ceftazidime): 2 g IV q8hrs
- Carbapenems (see Carbapenems)
- Fluoroquinolones (see Fluoroquinolones)
- Ciprofloxacin (Cipro) (see Ciprofloxacin): 400 mg IV q8hrs
- Levofloxacin (Levaquin) (see Levofloxacin): 750 mg IV q24hrs
- Monobactams
- Aztreonam (Azactam) (see Aztreonam): 2 g IV q8hrs
- Aminoglycosides (see Aminoglycosides)
- Amikacin (see Amikacin): 15-20 mg/kg IV q24hrs
- Gentamicin (see Gentamicin): 5-7 mg/kg IV q24hrs
- Tobramycin (see Tobramycin): 5-7 mg/kg IV q24hrs
- Anti-Pseudomonal Penicillins (see Penicillins)
Pathogen-Specific Antibiotics for Hospital-Acquired Pneumonia (HAP) (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
HAP/VAP Due to Methicillin-Resistant Staphylococcus Aureus (MRSA) (see Staphylococcus Aureus)
- Recommended Agents for the Treatment of HAP/VAP Due to MRSA (Strong Recommendation, Moderate-Quality Evidence): meta-analyses indicate no difference in mortality between these agents (Clin Infect Dis, 2016) [MEDLINE]
- Oxazolidinones
- Linezolid (Zyvox) (see Linezolid): 600 mg IV q12hrs
- Glycopeptides
- Vancomycin (see Vancomycin): consider load of 25-30 mg/kg IV, then 15 mg/kg IV q8-12 hrs with target trough 15-20 mg/mL
- Oxazolidinones
HAP/VAP Due to Pseudomonas Aeruginosa (see Pseudomonas Aeruginosa)
- Antibiotics for HAP/VAP Due to Pseudomonas Aeruginosa Should Be Guided by Antimicrobial Susceptibility Testing (Strong Recommendation, Low-Quality Evidence)
- Aminoglycoside Monotherapy for HAP/VAP Due to Pseudomonas Aeruginosa is Not Recommended (Strong Recommendation, Very Low-Quality Evidence)
- Indications for Double-Coverage of Pseudomonas Aeruginosa HAP/VAP (Strong Recommendation, Low-Quality Evidence)
- High Risk for Mortality: defined as mortality risk >25% (low risk for mortality is defined as <15% risk)
- Need for Ventilatory Support
- Septic Shock
- Lack of Availability of Antibiotic Susceptibility Testing
- High Risk for Mortality: defined as mortality risk >25% (low risk for mortality is defined as <15% risk)
HAP/VAP Due to Extended-Spectrum β-Lactamase (ESBL)-Producing Gram-Negative Bacilli
- Antibiotics for HAP/VAP Due to ESBL-Producing Gram-Negative Bacilli Should Be Guided by Antimicrobial Susceptibility Testing (Strong Recommendation, Very Low-Quality Evidence)
HAP/VAP Due to Acinetobacter (see Acinetobacter)
- HAP/VAP Due to Acinetobacter Should Be Treated with Ampicillin-Sulbactam (Unasyn) or a Carbapenem, if Susceptible (Weak Recommendation, Low-Quality Evidence)
- For HAP/VAP Due to Acinetobacter, Tigecycline is Not Recommended (Strong Recommendation, Low-Quality Evidence)
- For HAP/VAP Due to Acinetobacter Which is Susceptible Only to Polymyxins, Intravenous Polymyxin Should Be Used (Strong Recommendation, Low-Quality Evidence) with Inhaled Colistin (Weak Recommendation, Low-Quality Evidence)
- For HAP/VAP Due to Acinetobacter Which is Susceptible Only to Colistin, Adjunctive Rifampicin is Not Recommended (Weak Recommendation, Moderate-Quality Evidence)
HAP/VAP Due to Carbapenem-Resistant Pathogens
- For HAP/VAP Due to Carbapenem-Resistant Pathogens Which is Only Sensitive to Polymyxins, Intravenous Polymyxin Should Be Used (Strong Recommendation, Moderate-Duality Evidence) with Inhaled Colistin (Weak)
Duration of Therapy for Hospital-Acquired Pneumonia (HAP)
Clinical Efficacy
- Cochrane Database Systematic Review and Meta-Analysis of Using Serum Procalcitonin to Start or Stop Antibiotics in Acute Respiratory Tract Infection (Cochrane Database Syst Rev, 2017) [MEDLINE]
- Use of Serum Procalcitonin to Guide Initiation and Duration of Antibiotics Results in Lower Risks of Mortality, Lower Antibiotic Consumption, and Lower Risk of Antibiotic-Associated Adverse Effects
- Results were Similar for Different Clinical Settings and Types of Acute Respiratory Tract Infections
- Future Research is Required to Confirm the Results in Immunocompromised Patients and Patients with Non-Respiratory Infections
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
- For HAP/VAP, Antibiotic Therapy Should Be De-Escalated (Weak Recommendation, Very Low-Quality Evidence)
- For Patients with HAP, a 7 Day Course of Therapy is Recommended Over Longer Duration of Therapy (Strong Recommendation, Very Low-Quality Evidence): some clinical situations may merit a shorter/longer duration of therapy, depending on the rate of improvement in clinical/radiologic/laboratory parameters
- For HAP/VAP, Combined Clinical Criteria and Serum Procalcitonin Should Be Used to Guide Antibiotic Discontinuation Over Clinical Criteria Alone (Weak Recommendation, Low-Quality Evidence)
- However, is it Unclear if there are Benefits of Using Serum Procalcitonin to Determine Whether or Not to Discontinue Antibiotic Therapy in Settings Where Standard Antimicrobial Therapy for VAP is Already ≤7 Days
- For HAP/VAP, Clinical Pulmonary Infection Score (CPIS) Should Not Be Used to Guide Antibiotic Discontinuation (Weak Recommendation, Low-Quality Evidence)
Treatment of Ventilator-Associated Tracheobronchitis
Clinical Efficacy
- Antibiotic Therapy May Shorten the Duration of Mechanical Ventilation, But it is Unclear as to Whether it Improves Other Clinical Outcomes (Due to Inconsistent Data)
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
- Patients with Ventilator-Associated Tracheobronchitis Should Not Be Treated with Antibiotic Therapy (Weak Recommendation, Low-Quality Evidence)
Treatment of Ventilator-Associated Pneumonia (VAP)
General Comments
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
- All Hospitals Should Regularly Generate and Distribute an Antibiogram (Particularly One Which is Specific for the Intensive Care Unit Population)
- Microbial Flora and Resistance Patterns Vary Significantly Between Countries, Regions, and Hospitals
- Antibiogram Should Inform Empiric Treatment Decisions
- Meta-Analyses Indicate that Inadequate and/or Delayed Antibiotic Treatment of VAP Results in a (2.34x) Increased Mortality Rate (J Crit Care, 2008) [MEDLINE]
Initial Antibiotic Choice Based on Gram Stain (see Sputum Culture)
Clinical Efficacy-Use of Gram Stain to Guide Initial Antibiotic Therapy in Ventilator-Associated Pneumonia
- Japanese GRACE-VAP Multicenter, Open-Label, Noninferiority Randomized Trial of the Use of Gram Stain to Guide the Initial Antibiotic Treatment of Ventilator-Associated Pneumonia (JAMA Netw Open, 2022) [MEDLINE]: n = 206 (Patients Age ≥15 from 12 ICU’s)
- Clinical Response Occurred in 76.7% of Patients in the Gram Stain-Guided Group and 71.8% of Patients in the Guideline-Based Group (Risk Difference, 0.05; 95% CI: -0.07 to 0.17; P < 0.001 for Noninferiority)
- Reduced Use of Antipseudomonal Agents (30.1%; 95% CI: 21.5%-39.9%; P < .001) and Anti-MRSA Agents (38.8%; 95% CI: 29.4%-48.9%; P < 0.001) was Observed in the Gram Stain-Guided Group vs Guideline-Based Group
- The 28-Day Cumulative Incidence of Mortality was 13.6% (n = 14) in the Gram Stain-Guided Group vs 17.5% (n = 18) in the Guideline-Based Group (P = 0.39)
- Escalation of Antibiotics According to Culture Results was Performed in 6.8% of Patients in the Gram Stain-Guided Group and 1.0% of Patients in the Guideline-Based Group (P = 0.03)
- There were No Significant Differences Between the Groups in ICU-Free Days, Ventilator-Free Days, and Adverse Events
- Authors Concluded that Gram Stain-Guided Antibiotic Treatment was Non inferior to Guideline-Based Antibiotic Treatment and Significantly Decreased the Use of Broad-Spectrum Antibiotics in Ventilator-Associated Pneumonia
Antibiotic Use Based on Quantitative Cultures in Ventilator-Associated Pneumonia (VAP)
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
- Non-Invasive Sampling with Semiquantitative Cultures is Recommended Over Non-Invasive Sampling with Quantitative Cultures or Invasive Sampling with Quantitative Cultures (Weak Recommendation, Low Quality Evidence): there is no evidence that invasive microbiologic sampling improves clinical outcomes compared with non-invasive sampling with either quantitative or semiquantitative cultures
- Non-Invasive Sampling Methods: endotracheal suction sampling
- Quantitative Threshold for Endotracheal Tube Aspirate: <10 to the 5th CFU/mL
- Invasive Sampling Methods: bronchoscopy with bronchoalveolar lavage or protected brush specimen, blind bronchial sampling (“mini-BAL”)
- Non-Invasive Sampling Methods: endotracheal suction sampling
- Effect of Invasive Sampling with Quantitative Cultures on Antibiotic Exposure is Unclear
- If Invasive Sampling with Quantitative Cultures are Performed, Diagnostic Thresholds for VAP (Protected Brush Specimen with <10 to the 3rd CFU/mL, Bronchoalveolar With <10 to the 4th CFU/mL) Should Be Utilized to Decide Whether to Stop Antibiotics (Weak Recommendation, Very Low Quality Evidence)
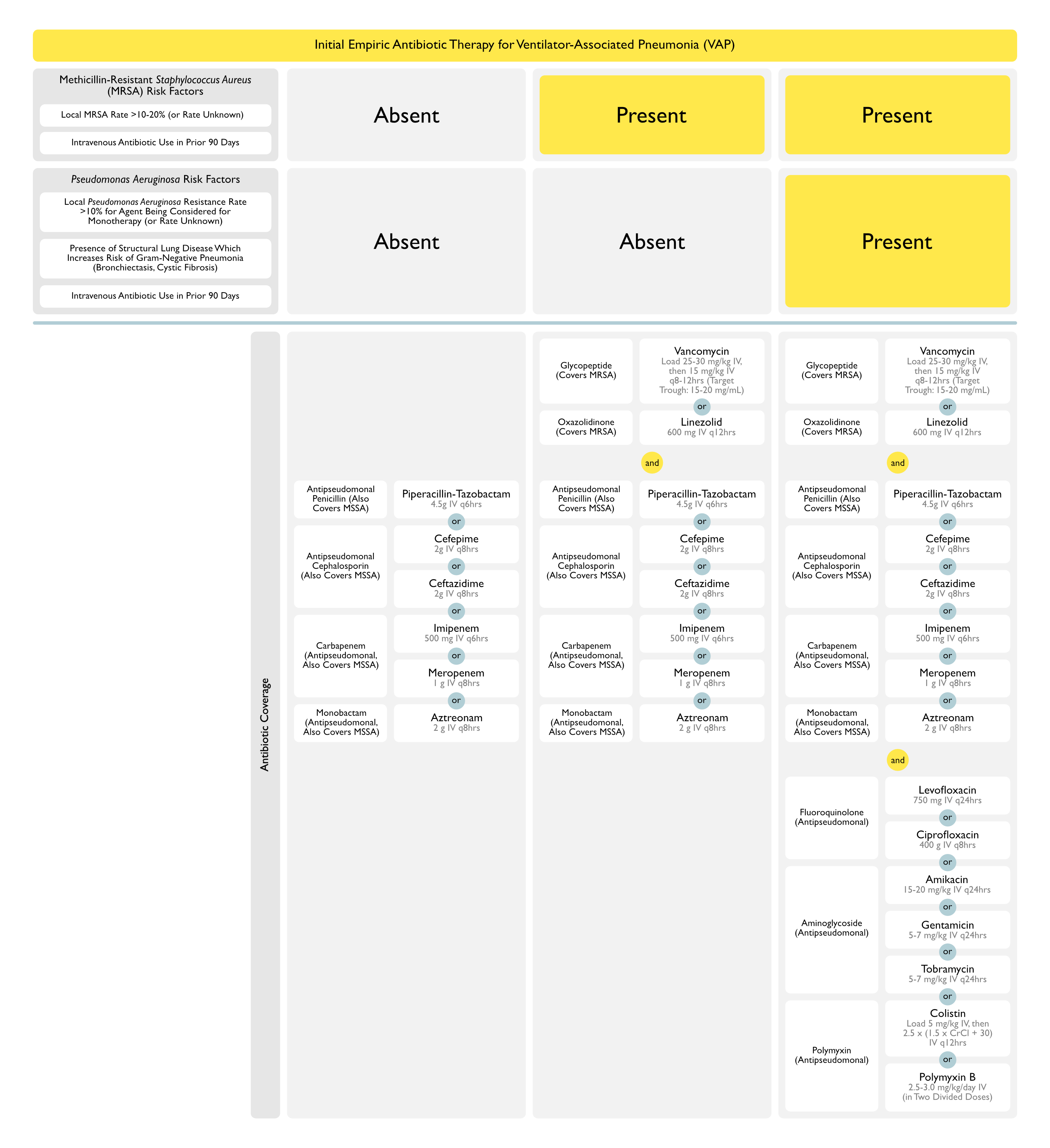
Empiric Antibiotics for Ventilator-Associated Pneumonia (VAP)
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
General Comments
- Choose One Agent with Activity Against Either Methicillin-Sensitive Staphylococcus Aureus (MSSA) or Methicillin-Resistant Staphylococcus Aureus (MRSA) + One β-Lactam Agent with Activity Against Pseudomonas Aeruginosa (and Gram-Negatives) + One Non-β-Lactam Agent with Activity Against Pseudomonas Aeruginosa (and Other Gram-Negatives) (Strong Recommendation, Low-Quality Evidence)
- Use an Agent Active Against Methicillin-Resistant Staphylococcus Aureus (MRSA) for the Following Indications (Weak Recommendation, Very Low-Quality Evidence)
- Presence of Local Staphylococcus Aureus Methicillin-Resistance Rate >10-20% (or Where Resistance Rate is Unknown)
- Prior Intravenous Antibiotic Use in the Last 90 Days
- Use Agents from Two Different Anti-Pseudomonal Classes for the Following Indications (Weak Recommendation, Low-Quality Evidence): the rationale for double-covering Pseudomonas is to increase the probability that the organism will be sensitive to at least one of the agents
- Presence of Local Gram-Negative Resistance Rate >10% for the Agent Being Considered for Monotherapy (or Where Resistance Rate is Unknown)
- Presence of Structural Lung Diseases Which Increase the Risk of Gram-Negative Pneumonia (Bronchiectasis, Cystic Fibrosis)
- Prior Intravenous Antibiotic Use in the Last 90 Days
- In Patients with Suspected VAP, Avoid Aminoglycosides if Alternative Agents with Gram-Negative Coverage are Available (Weak Recommendation, Low-Quality Evidence): due to their poor lung penetration, risk of nephrotoxicity, risk of ototoxicity, and poorer clinical response rates (but no difference in mortality rate) than that of other drug classes
- In Patients with Suspected VAP, Avoid Colistin if Alternative Agents with Gram-Negative Coverage are Available (Weak Recommendation, Very Low-Quality Evidence)
- Dosing of Antibiotics in HAP/VAP Should Be Determined Using Pharmacokinetic/Pharmacodynamic Data (Using Blood Antibiotic Concentrations, Extended and Continuous Infusions, Weight-Based Dosing for Certain Antibiotics, etc) Rather than the Manufacturer’s Prescribing Recommendations (Weak Recommendation, Very Low-Quality Evidence)
- Use an Agent Active Against Methicillin-Resistant Staphylococcus Aureus (MRSA) for the Following Indications (Weak Recommendation, Very Low-Quality Evidence)
Agents with Activity Against Methicillin-Sensitive Staphylococcus Aureus (MSSA) (see Staphylococcus Aureus)
- Preferred Agents for Proven MSSA: due to decreased likelihood of inducing resistance
- Other Agents with MSSA Coverage (Weak Recommendation, Very Low-Quality Evidence)
- Cefepime (Maxipime) (see Cefepime)
- Imipenem (Primaxin) (see Imipenem)
- Meropenem (Merrem) (see Meropenem)
- Levofloxacin (Levaquin) (see Levofloxacin)
- Piperacillin-Tazobactam (Zosyn) (see Piperacillin-Tazobactam)
Agents with Activity Against Methicillin-Resistant Staphylococcus Aureus (MRSA) (see Staphylococcus Aureus) (Strong Recommendation, Moderate-Quality Evidence)
- Recommended Agents (Strong Recommendation, Moderate-Quality Evidence)
- Oxazolidinones
- Linezolid (Zyvox) (see Linezolid): 600 mg IV q12hrs
- Glycopeptides
- Vancomycin (see Vancomycin): consider load of 25-30 mg/kg IV, then 15 mg/kg IV q8-12 hrs with target trough 15-20 mg/mL
- Oxazolidinones
- Other Agents: these agents have not been as well-studied in the treatment of VAP
- Ceftaroline (Teflaro) (see Ceftaroline)
- Quinupristin-Dalfopristin (Synercid) (see Quinupristin-Dalfopristin)
- Tedizolid (Sivextro) (see Tedizolid)
- Teicoplanin (Targocid) (see Teicoplanin)
- Telavancin (Vibativ) (see Telavancin)
- Agents Which are Not Recommended for Use in VAP: due to demonstrated lower clinical cure rates in VAP
- Ceftobiprole (see Ceftobiprole)
- Tigecycline (Tygacil) (see Tigecycline)
β-Lactam Agents with Activity Against Pseudomonas Aeruginosa (see Pseudomonas Aeruginosa)
- Anti-Pseudomonal Penicillins (see Penicillins)
- Piperacillin-Tazobactam (Zosyn) (see Piperacillin-Tazobactam): 4.5 g IV q6hrs
- Anti-Pseudomonal Cephalosporins
- Cefepime (Maxipime) (see Cefepime): 2 g IV q8hrs
- Ceftazidime (Fortaz) (see Ceftazidime): 2 g IV q8hrs
- Carbapenems (see Carbapenems)
- Monobactams
- Aztreonam (Azactam) (see Aztreonam): 2 g IV q8hrs
- In the absence of other options, aztreonam may be used with other β-lactams, since it has a different target within the bacterial cell wall
- Aztreonam (Azactam) (see Aztreonam): 2 g IV q8hrs
- Agents Which Have Not Been Studied in VAP
- Ceftazidime-Avibactam (Avycaz) (see Ceftazidime-Avibactam)
- Ceftolozane-Tazobactam (Zerbaxa) (see Ceftolozane-Tazobactam)
- Agents Which are Not Recommended for Use in VAP: due to demonstrated lower clinical cure rates in VAP
- Doripenem (Finibax, Doribax) (see Doripenem)
Non-β-Lactam Agents with Activity Against Pseudomonas Aeruginosa (see Pseudomonas Aeruginosa)
- Fluoroquinolones (see Fluoroquinolones)
- Ciprofloxacin (Cipro) (see Ciprofloxacin): 400 mg IV q8hrs
- Levofloxacin (Levaquin) (see Levofloxacin): 750 Hg IV q24hrs
- Aminoglycosides (see Aminoglycosides): in meta-analyses, aminoglycoside regimens are associated with lower clinical response rates, but no difference in mortality rate
- General Comments: aminoglycosides should be avoided if alternative agents with adequate Gram-negative coverage are available (Weak Recommendation, Low-Quality Evidence)
- Amikacin (see Amikacin): 15-20 mg/kg IV q24hrs
- Gentamicin (see Gentamicin): 5-7 mg/kg IV q24hrs
- Tobramycin (see Tobramycin): 5-7 mg/kg IV q24hrs
- Polymyxins (see Polymyxins)
- Colistin (see Colistin): load 5 mg/kg IV, then 2.5 mg x (1.5 x CrCl + 30) IV q12hrs
- In Cases with Resistant Pseudomonas Aeruginosa, Combination Intravenous + Aerosolized Colistin was Superior to Intravenous Colistin Alone, in Terms of Cure Rate and Days of Mechanical Ventilation After VAP Onset (Chest, 2013) [MEDLINE]
- Polymyxin B (see Polymyxin B): 2.5–3.0 mg/kg/day IV divided in 2 daily doses
- Colistin (see Colistin): load 5 mg/kg IV, then 2.5 mg x (1.5 x CrCl + 30) IV q12hrs
Pathogen-Specific Antibiotics for Ventilator-Associated Pneumonia (VAP) (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
Role of Inhaled Antibiotic Therapy in the Management of Multidrug-Resistant Gram-Negative Bacilli
- Gram-Negative Bacilli Susceptible Only to Aminoglycosides/Polymyxins Should Be Treated with Both Inhaled (Gentamicin, Tobramycin, Colistin) and Systemic Antibiotics, as Opposed to Systemic Antibiotics Alone (Weak Recommendation, Very Low-Quality Evidence): meta-analyses suggest that the addition of inhaled antibiotics to systemic antibiotics increased the clinical cure rate, but had no effect on the mortality rate or nephrotoxicity (Clin Infect Dis, 2016) [MEDLINE]
- Rationale: antibiotic efficacy against bacteria which reside within purulent secretions may require antibiotic concentrations which are >10–25x the minimum inhibitory concentration (MIC) (these MIC’s cannot be achieved with intravenous therapy alone and the addition of inhaled antibiotic therapy may be beneficial in achieving the relevant MIC)
- Notably, subtherapeutic antibiotic concentrations within the lung and airway may further select antibiotic-resistant organisms
- Typical Multidrug-Resistant Organisms: multidrug-resistant Klebsiella Pneumoniae, Pseudomonas Aeruginosa, and Acinteobacter Baumannii
- It is Also Reasonable to Consider the Addition of Inhaled Antibiotics as Adjunctive Therapy in Patients Who are Not Responding to Intravenous Antibiotics Alone (Regardless of Whether the Infecting Organism is Multidrug-Resistant or Not)
- Rationale: antibiotic efficacy against bacteria which reside within purulent secretions may require antibiotic concentrations which are >10–25x the minimum inhibitory concentration (MIC) (these MIC’s cannot be achieved with intravenous therapy alone and the addition of inhaled antibiotic therapy may be beneficial in achieving the relevant MIC)
HAP/VAP Due to Methicillin-Resistant Staphylococcus Aureus (MRSA) (see Staphylococcus Aureus)
- Recommended Agents for the Treatment of HAP/VAP Due to MRSA (Strong Recommendation, Moderate-Quality Evidence): meta-analyses indicate no difference in mortality between these agents (Clin Infect Dis, 2016) [MEDLINE]
- Oxazolidinones
- Linezolid (Zyvox) (see Linezolid): 600 mg IV q12hrs
- Glycopeptides
- Vancomycin (see Vancomycin): consider load of 25-30 mg/kg IV, then 15 mg/kg IV q8-12 hrs with target trough 15-20 mg/mL
- Oxazolidinones
HAP/VAP Due to Pseudomonas Aeruginosa (see Pseudomonas Aeruginosa)
- Antibiotics for HAP/VAP Due to Pseudomonas Aeruginosa Should Be Guided by Antimicrobial Susceptibility Testing (Strong Recommendation, Low-Quality Evidence)
- Aminoglycoside Monotherapy for HAP/VAP Due to Pseudomonas Aeruginosa is Not Recommended (Strong Recommendation, Very Low-Quality Evidence)
- Indications for Double-Coverage of Pseudomonas Aeruginosa HAP/VAP (Strong Recommendation, Low-Quality Evidence)
- High Risk for Mortality: defined as mortality risk >25% (low risk for mortality is defined as <15% risk)
- Need for Ventilatory Support (see Invasive Mechanical Ventilation)
- Septic Shock (see Sepsis)
- Lack of Availability of Antibiotic Susceptibility Testing
- High Risk for Mortality: defined as mortality risk >25% (low risk for mortality is defined as <15% risk)
HAP/VAP Due to Extended-Spectrum β-Lactamase (ESBL)-Producing Gram-Negative Bacilli
- Antibiotics for HAP/VAP Due to ESBL-Producing Gram-Negative Bacilli Should Be Guided by Antimicrobial Susceptibility Testing (Strong Recommendation, Very Low-Quality Evidence)
HAP/VAP Due to Acinetobacter (see Acinetobacter)
- HAP/VAP Due to Acinetobacter Should Be Treated with Ampicillin-Sulbactam (Unasyn) or a Carbapenem, if Susceptible (Weak Recommendation, Low-Quality Evidence)
- For HAP/VAP Due to Acinetobacter, Tigecycline is Not Recommended (Strong Recommendation, Low-Quality Evidence)
- For HAP/VAP Due to Acinetobacter Which is Susceptible Only to Polymyxins, Intravenous Polymyxin Should Be Used (Strong Recommendation, Low-Quality Evidence) with Inhaled Colistin (Weak Recommendation, Low-Quality Evidence)
- For HAP/VAP Due to Acinetobacter Which is Susceptible Only to Colistin, Adjunctive Rifampicin is Not Recommended (Weak Recommendation, Moderate-Quality Evidence)
HAP/VAP Due to Carbapenem-Resistant Pathogens
- For HAP/VAP Due to Carbapenem-Resistant Pathogens Which is Only Sensitive to Polymyxins, Intravenous Polymyxin Should Be Used (Strong Recommendation, Moderate-Duality Evidence) with Inhaled Colistin (Weak)
Antibiotic Choice and Stewardship in Ventilator-Associated Pneumonia (VAP)
Goals of Antibiotic Stewardship
- Optimization of Clinical VAP Outcomes
- Minimization of Antibiotic Resistance, Antibiotic Toxicity, Adverse Events, and Selection of Pathogenic Organisms
- Decrease in Health Care Costs
Techniques of Antibiotic Stewardship
- Formulary Restriction/Preauthorization for Antibiotics
- Audit of Antibiotic Use with Feedback to the Prescriber
- De-Escalation of Antibiotics
- Start with Broad-Spectrum Antibiotic Strategy
- At First Opportunity (with the Aid of Culture Data), Provider Should Decrease the Number of Antimicrobial Agents, Shorten the Duration of Antimicrobial Agent Exposure, and/or Discontinue Antimicrobial Therapy (as Dictated by the Patient’s Clinical Response and Culture Results)
Clinical Efficacy
- Study of Microbial Isolates and Susceptibility Across Hospital Sites in Different Spanish Cities (Am J Respir Crit Care Med, 1999) [MEDLINE]
- Etiologies of VAP Varied Across the Treatment Sites
- Therefore, Authors Conclude that Antimicrobial Prescribing Practices Should Be Based on Information About Patterns of Multi-Drug Resistant Isolates from Each Institution, Instead of Following General Recommendations
- PneumA Trial of Shortened Antibiotic Duration in VAP Treatment (JAMA, 2003) [MEDLINE]
- Among Patients Who Had Received Initial Empiric Antibiotic Therapy (with the Possible Exception of Those with Non-Fermenting GNR Infections), 8-day Regimen was Comparable to 15-Day Regimen in Terms of Clinical Outcome: 8-day group had less antibiotic use
- Trial Using Antibiotic De-Escalation in VAP (Crit Care Med, 2004) [MEDLINE]
- De-Escalation was Possible in 31.4% of Cases
- Bronchoscopic and/or tracheal aspirate cultures were instrumental in allowing de-escalation
- Authors did not perform de-escalation without a known pathogen
- De-Escalation was Performed in Only 2.7% of Cases with Non-Fermenting GNR’s and Other Potentially Multi-Drug Resistant Organisms (Such as Pseudomonas Aeruginosa)
- De-Escalation was Possible in 31.4% of Cases
- Multicenter Observational Study of VAP (Chest, 2006) [MEDLINE]
- De-Escalation was Performed in 22.1% of Cases (and Escalation in 15.3% of Cases)
- De-Escalation was Performed in Only 6.5% of Cases without a Known Pathogen
- Mortality was Significantly Decreased in Cases with De-Escalation (17%), vs 23.7% in Those with No Change in Therapy and 42.6% in Those with Escalation in Therapy
- Study of the Impact of Regular Communication Between Infectious Disease and Critical Care Providers on Antimicrobial Use and Patient Outcome (Crit Care Med, 2013) [MEDLINE]
- Active Communication Between Critical Care Providers and Infectious Disease Providers Significantly Decreases Medical ICU Antibiotic Overuse (by Earlier Modification or Cessation of Antibiotics) without an Increase in Mortality: this may decrease health care costs
- Systematic Review of Antibiotic De-Escalation in the ICU (Clin Infect Dis, 2016) [MEDLINE]
- There is No Uniform Definition of “De-Escalation”
- There is Little Evidence Related to the Effect of De-Escalation on Duration of Antimicrobial Therapy, Emergence of Resistance, or Costs
- There was an Association Between De-Escalation and Improved Outcome: however, from the evidence, it is not clear that this is causal (since patients with clinical improvement may have been the ones with higher rates of de-escalation)
Recommendations
- Knowledge of Local Antibiograms is Essential in Determining Appropriate Initial Antibiotic Regimens
- Antibiotic De-Escalation (to a Narrower Regimen) is Recommended, Whenever Possible (Weak Recommendation, Very Low-Quality Evidence) (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
- Collaborative Approach Between Critical Care and Infectious Disease Providers is Recommended to Decrease Antibiotic Overuse
Duration of Antibiotic Therapy in Ventilator-Associated Pneumonia (VAP)
Clinical Efficacy
- Cochrane Database Systematic Review and Meta-Analysis of Using Serum Procalcitonin to Start or Stop Antibiotics in Acute Respiratory Tract Infection (Cochrane Database Syst Rev, 2017) [MEDLINE]
- Use of Serum Procalcitonin to Guide Initiation and Duration of Antibiotics Results in Lower Risks of Mortality, Lower Antibiotic Consumption, and Lower Risk of Antibiotic-Associated Adverse Effects
- Results were Similar for Different Clinical Settings and Types of Acute Respiratory Tract Infections
- Future Research is Required to Confirm the Results in Immunocompromised Patients and Patients with Non-Respiratory Infections
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2016 Clinical Practice Guidelines for the Management of HAP/VAP (Clin Infect Dis, 2016) [MEDLINE]
- For HAP/VAP, Antibiotic Therapy Should Be De-Escalated (Weak Recommendation, Very Low-Quality Evidence)
- For VAP, a 7 Day Course of Therapy is Recommended Over Longer Duration of Therapy (Strong Recommendation, Moderate-Quality Evidence): some clinical situations may merit a shorter/longer duration of therapy, depending on the rate of improvement in clinical/radiologic/laboratory parameters
- Evidence Indicates that Shorter Courses of Antibiotics Decrease Antibiotic Exposure and the Risk of Recurrent Pneumonia Due to Multidrug-Resistant Organisms
- Duration of Antibiotic Therapy Do Not Appear to Impact the Mortality Rate
- For HAP/VAP, Combined Clinical Criteria and Serum Procalcitonin Should Be Used to Guide Antibiotic Discontinuation Over Clinical Criteria Alone (Weak Recommendation, Low-Quality Evidence)
- However, is it Unclear if there are Benefits of Using Serum Procalcitonin to Determine Whether or Not to Discontinue Antibiotic Therapy in Settings Where Standard Antimicrobial Therapy for VAP is Already ≤7 Days
- For HAP/VAP, Clinical Pulmonary Infection Score (CPIS) Should Not Be Used to Guide Antibiotic Discontinuation (Weak Recommendation, Low-Quality Evidence)
Respiratory Support
Supplemental Oxygen Therapy (see Oxygen)
- Recommendations (British Thoracic Society Emergency Oxygen Guidelines, 2017) (Thorax, 2017) [MEDLINE]
- SpO2 Target
- Oxygen Should Be Prescribed to Achieve a Target Saturation of 94–98% for Most Acutely Ill Patients or 88–92% or Patient-Specific Target Range for Those at Risk of Hypercapnic Respiratory Failure
- Best Practice is to Prescribe a Target Range for All Hospitalized Patients at the Time of Hospital Admission So that Appropriate Oxygen Therapy Can Be Started in the Event of Unexpected Clinical Deterioration with Hypoxemia and Also to Ensure that the Oximetry Section of the Early Warning Score Can Be Scored Appropriately
- SpO2 Target
- Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- Supplemental Oxygen Therapy Should Be Titrated to SpO2 ≤96% (Strong Recommendation)
- SpO2 >96% likely is Associated with a Small, But Important, Increased Risk of Death without Plausible Clinical Benefit
- Supplemental Oxygen Therapy Should Be Titrated to SpO2 ≤96% (Strong Recommendation)
Prognostic Factors
Hospital-Acquired Pneumonia (HAP)
Effect of Hospital-Acquired Pneumonia (HAP) on Mortality Rate
Ventilator-Associated Pneumonia (VAP)
Effect of Ventilator-Associated Pneumonia (VAP) on Mortality Rate
- Mortality Rate Attributable to VAP is 13% (Lancet Infect Dis, 2013) [MEDLINE]: however, the all-cause mortality rate associated with VAP has been estimated to be 20-50%
Effect of Ventilator-Associated Pneumonia (VAP) on Other Outcomes
- VAP Increased the Duration of Mechanical Ventilation (Clin Infect Dis, 2010) [MEDLINE]; (Infect Control Hosp Epidemiol, 2012) [MEDLINE]: by 7.6-11.5 days
- VAP Increased Hospital Length of Stay (Clin Infect Dis, 2010) [MEDLINE]; (Infect Control Hosp Epidemiol, 2012) [MEDLINE]: by 11.5-13.1 days
- Excess Cost Associated with VAP is Estimated to $40k Per Patient (Infect Control Hosp Epidemiol, 2012) [MEDLINE]
Ventilator-Associated Pneumonia (VAP) in the Elderly (Crit Care Med, 2014) [MEDLINE]
- Advanced Age
- Advanced Age Did Not Increase the Prevalence of VAP, But it Increased the VAP-Associated Mortality Rate (Age 65-74 y/o and Age >75 y/o Had 51% Mortality Rate, as Compared to 35% Mortality Rate for Younger Age Groups)
- Older Age Groups Had Higher Incidence of Chronic Congestive Heart Failure, Diabetes Mellitus, and Non-Metastatic Cancer
- Age Did Not Impact the Duration of Mechanical Ventilation or Length of ICU Stay
- Diabetes Mellitus (see Diabetes Mellitus)
- Diabetes Mellitus Increased the VAP Mortality Rate
- Septic Shock (see Sepsis)
- Presence of Septic Shock Increased the VAP Mortality Rate
- Poor Prognostic Factor: Pseudomonas aeruginosa and/or Acinetobacter calcoaceticus isolation
- Poor Prognostic Factor: Patients who have initially been treated with inappropriate antibiotics
- No difference in morbidity or mortality has been found between the patients who had VAP diagnosed with quantitative sputum c/s vs protected brush specimens
- Quantitative BAL cultures has not been shown to improve VAP outcome
- Unknown if there is a difference in morbidity or mortality if one diagnoses VAP with a nonquantitative sputum c/s vs quantitative culture technique
Hospital Readmission for Pneumonia
- Clinical Efficacy
- Study of Factors Related to Hospital Readmission for Pneumonia (Clin Infect Dis, 2013) [MEDLINE]
- Hospital Readmission Rate for Pneumonia: 20%
- Patients with HCAP were 7.5x More Likely to Be Readmitted than Patients with CAP
- Criteria in HCAP that Associated with the Risk of Hospital Readmission
- Admission from Long-term Care (adjusted odds ratio [AOR], 2.2 [95% CI, 1.4-3.4])
- Immunosuppression (AOR, 1.9 [95% CI, 1.3-2.9])
- Prior Antibiotics (AOR, 1.7 [95% CI, 1.2-2.6])
- Prior Hospitalization (AOR, 1.7 [95% CI, 1.1-2.5])
- Study of Factors Related to Hospital Readmission for Pneumonia (Clin Infect Dis, 2013) [MEDLINE]
References
Treatment
General
- Variations in etiology of ventilator-associated pneumonia across four treatment sites: implications for antimicrobial prescribing practices. Am J Respir Crit Care Med. 1999;160(2):608-613 [MEDLINE]
- PneumA Trial. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290(19):2588-2598 [MEDLINE]
- Antimicrobial activity of tigecycline tested against organisms causing community-acquired respiratory tract infection and nosocomial pneumonia. Diagn Microbiol Infect Dis. 2005;52:187-193
- Parenteral and inhaled colistin for treatment of ventilator-associated pneumonia. Clin Infect Dis. 2006;43(suppl 2):S89-S94
- De-escalation in lower respiratory tract infections. Curr Opin Pulm Med. 2006;12(5):364-368 [MEDLINE]
- De-escalation therapy in ventilator-associated pneumonia. Curr Opin Crit Care. 2006;12(5):452-457 [MEDLINE]
- Clinical characteristics and treatment patterns among patients with ventilator-associated pneumonia. Chest 2006; 129:1210–1218 [MEDLINE]
- Impact of inappropriate antibiotic therapy on mortality in patients with ventilator-associated pneumonia and blood stream infection: a meta-analysis. J Crit Care 2008; 23:91–100 [MEDLINE]
- Antibiotic stewardship: overcoming implementation barriers. Curr Opin Infect Dis. 2011;24(4): 357-362 [MEDLINE]
- Antimicrobial stewardship programs: mandatory for all ICUs. Crit Care. 2012;16:179. doi:10.1186/cc11853 [MEDLINE]
- Impact of regular collaboration between infectious diseases and critical care practitioners on antimicrobial utilization and patient outcome. Crit Care Med. 2013;41:2099–2107. doi: 10.1097/CCM.0b013e31828e9863 [MEDLINE]
- Effect of aerosolized colistin as adjunctive treatment on the outcomes of microbiologically documented ventilator-associated pneumonia caused by colistin-only susceptible gram-negative bacteria. Chest. 2013 Dec;144(6):1768-75. doi: 10.1378/chest.13-1018 [MEDLINE]
- Antibiotic stewardship in hospital-acquired pneumonia. Chest. 2013;143:1195–1196. doi:10.1378/chest.12-2729 [MEDLINE]
- What can be expected from antimicrobial de-escalation in the critically ill? Intensive Care Med 2014; 40:92–5 [MEDLINE]
- A Systematic Review of the Definitions, Determinants, and Clinical Outcomes of Antimicrobial De-escalation in the Intensive Care Unit. Clin Infect Dis. 2016 Apr 15;62(8):1009-17. doi: 10.1093/cid/civ1199. Epub 2015 Dec 23 [MEDLINE]
- Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016 Sep 1;63(5):e61-e111. doi: 10.1093/cid/ciw353. Epub 2016 Jul 14 [MEDLINE]
- Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2017 Oct 12;10:CD007498. doi: 10.1002/14651858.CD007498.pub3 [MEDLINE]
- Effect of Gram Stain-Guided Initial Antibiotic Therapy on Clinical Response in Patients With Ventilator-Associated Pneumonia: The GRACE-VAP Randomized Clinical Trial. JAMA Netw Open. 2022 Apr 1;5(4):e226136. doi: 10.1001/jamanetworkopen.2022.6136 [MEDLINE]
Respiratory Support
- British Thoracic Society Emergency Oxygen Guideline Group BTS Emergency Oxygen Guideline Development Group. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax 2017;72(Suppl 1):ii1-90. 10.1136/ thoraxjnl-2016-209729 pmid:28507176 [MEDLINE]
- Oxygen therapy for acutely ill medical patients: a clinical practice guideline. BMJ. 2018 Oct 24;363:k4169. doi: 10.1136/bmj.k4169 [MEDLINE]
Tracheostomy (see Tracheostomy)
- The timing of tracheotomy in critically ill patients undergoing mechanical ventilation: a systematic review and meta-analysis of randomized controlled trials. Chest 2011;140(6):1456–1465 [MEDLINE]
- Early percutaneous tracheotomy versus prolonged intubation of mechanically ventilated patients after cardiac surgery: a randomized trial. Ann Intern Med 2011;154:373–383 [MEDLINE]
- Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA. 2013;309:2121–2129 [MEDLINE]