Neck CT with Intravenous Contrast: gold standard for imaging deep neck spaces
Neck MRI: may alternatively be used
Ultrasound: may help distinguish between phlegmon and abscess, give information about the condition of surrounding vessels, and guide fine needle aspiration
Carotid Angiogram/Venogram: may be helpful when carotid, jugular, or innominate vessels are involved
Clinical Features by Anatomic Space
Parapharyngeal Space
Anatomy: comprised of the lateral pharyngeal space, the pharyngomaxillary space, the pterygomaxillary space, and the pterygopharyngeal space
Posterior Compartment: carotid sheath (carotid artery, internal jugular vein, vagus nerve), glossopharyngeal and hypoglossal nerves, sympathetic chain, and lymphatics, accessory nerve (this nerve is relatively protected, as it is located behind the sternocleidomastoid muscle)
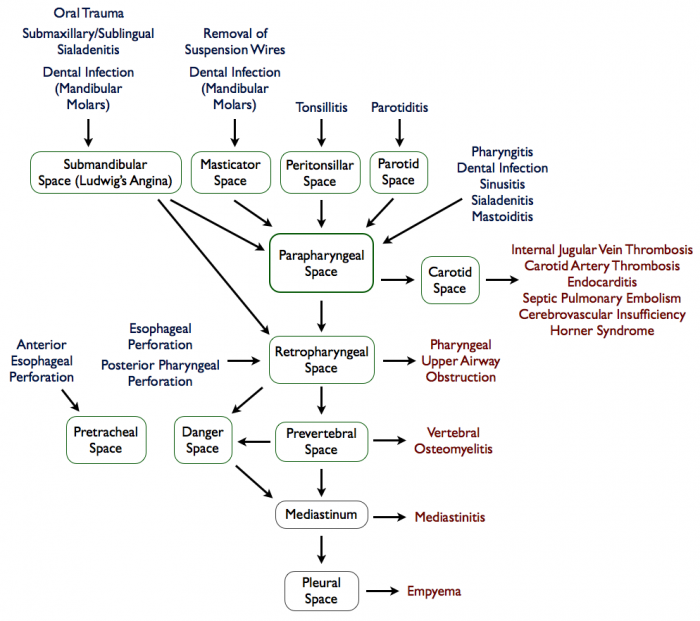
Anatomic Communication: parapharyngeal space is a centally located space, with connections to the other deep neck spaces
Infections that spread from the peritonsillar space (this was the most commonly affected space in the pre-antibiotic era): tonsillitis, pharyngitis, dental infection, sialadenitis, nasal infections, or mastoid/Bezold abscess
Posteromedially, parapharyngeal space communicates with the retropharyngeal space
Inferiorly, parapharyngeal space communicates with the submandibular space
Laterally, parapharyngeal space communicates with the masticator space
Clinical Features with Abscess in This Space
Trismus
Medial Displacement of the Lateral Pharyngeal Wall and Tonsil
The retropharyngeal space is sometimes considered a third medial compartment within the parapharyngeal space because these two spaces communicate laterally
This space lies between the visceral division of the middle layer of the deep cervical fascia around the pharyngeal constrictors and the alar division of the deep layer of deep cervical fascia posteriorly
It extends from the skull base to the tracheal bifurcation around T2 where the visceral and alar divisions fuse
Contents: retropharyngeal lymphatics
Anatomic Communication
Entry
Traumatic/Foreign Body Perforation of Posterior Pharyngeal Wall: common in adult cases
Traumatic/Foreign Body Perforation of Esophagus: common in adult cases
Extension from Parapharyngeal Space Abscess (resulting from infections in nose, adenoids, nasopharynx, and sinuses): respiratory tract infections account for >60% of retropharyngeal abscesses in children
Retropharyngeal lymph nodes tend to regress by about age 5 years, making infection in this space much more common in children than adults
Anterior Displacement of One or Both Sides of Posterior Pharyngeal Wall: due to involvement of lymph nodes, which are distributed lateral to the midline fascial raphe
Anatomy: spread within the danger space tends to occur rapidly because of loose areolar tissue in this region
Located posterior to the retropharyngeal space and anterior to the prevertebral space
It is a midline space without a midline raphe, so infections can occur bilaterally
Located between the alar and prevertebral divisions of the deep layer of the deep cervical fascia
Extends from the skull base to the posterior mediastinum and diaphragm
Laterally, it is limited by the fusion of the alar and prevertebral division with the transverse processes of the vertebrae
Some authors consider the danger space a component of the prevertebral space
Anatomic Communication
Entry
Extension from retropharyngeal, parapharyngeal, or prevertebral space abscesses
Exit
Extension into mediastinum -> resulting in empyema/sepsis
Masticator Space
Anatomy
Located laterally to the medial pterygoid fascia and medially to the masseter muscle
Bounded by the sphenoid bone, the posterior aspect of the mandible, and the zygomatic arch
Inferior to the temporal space
Anterolateral to the parapharyngeal space
Anatomic Communication
Entry
Dental Infections (particularly of the third mandibular molars)
Removal of Suspension Wires following Reduction and Fixation of Facial Fractures
Exit
Extension to parapharyngeal, parotid, or temporal spaces
Contents: masseter, pterygoids, ramus and body of the mandible, temporalis tendon, and the inferior alveolar vessels and nerve
Clinical Features with Abscess in This Space
Trismus: commonly seen as part of the initial presentation, but may also persist chronically
Submandibular Space
Anatomy: bounded inferiorly by the superficial layer of the deep cervical fascia extending from the hyoid to the mandible, laterally by the body of the mandible, and superiorly by the mucosa of the floor of mouth
Anatomic Communication
Entry
Oral Trauma
Submaxillary or Sublingual Sialadenitis
Dental Abscess of Mandibular Teeth
Exit
Extension to parapharyngeal and retropharyngeal spaces
Physiology
Inflammation and cellulitis of the submandibular space, usually originating in the submaxillary space and spreading to the sublingual space via the fascial planes (not via the lymphatics)
Induration of floor of mouth (which does not necessarily require a focal abscess) -> tongue is forced upward and backward, resulting in airway obstruction
Clinical Features with Abscess in This Space: Ludwig’s Angina (see Ludwig’s Angina)
Retropharyngeal abscess in children: the rising incidence of methicillin-resistant Staphylococcus aureus. Pediatr Infect Dis J. 2012 Jul;31(7):696-9 [MEDLINE]