Standing Orders Have Been Demonstrated to Be the Most Effective Means of Improving Vaccination Rates in Medical Offices/Hospitals/Long-Term Care Settings (JAMA, 2003) [MEDLINE]
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of CAP) (Clin Infect Dis, 2007) [MEDLINE]
Smoking Cessation is Recommended for Smokers Hospitalized with Community-Acquired Pneumonia (Moderate Recommendation, Level III Evidence)
Smokers Who Will Not Quit Should Be Vaccinated for Both Pneumococcus and Influenza (Weak Recommendation, Level III Evidence)
Treatment
Site of Care
Clinical Data-Hospital Admission
The Decision to Admit a Patient for Community-Acquired Pneumonia is the Most Costly Issue in the Management of Community-Acquired Pneumonia
Inpatient Care for Pneumonia is 25x as Expensive as Outpatient Care (Clin Ther, 1998) [MEDLINE]
Inpatient Care for Pneumonia Consumes the Majority of the Estimated $8.4-10 Billion Spent Annually on Pneumonia Treatment
CAP Patients Treated as Outpatients are Able to Resume Normal Activity Sooner than Those Who are Hospitalized
Approximately 74% of CAP Patients Prefer Outpatient Treatment (Arch Intern Med, 1996) [MEDLINE]
Hospitalization Increases the Risk of Venous Thromboembolism and Superinfection with More Virulent or Resistant Organisms (Arch Intern Med, 2004) [MEDLINE]
Clinical Data-Intensive Care Unit Admission
Systematic Review and Meta-Analysis of Criteria to Predict Intensive Care Unit Admission in Community-Acquired Pneumonia
Without the Major Criteria, a Threshold ≥3 Community-Acquired Pneumonia Minor Criteria (Below) Had a Pooled Sensitivity of 56% and Specificity of 91% for Predicting Intensive Care Unit Admission (Intensive Care Med, 2011) [MEDLINE]
Study of Association Between Intensive Care Unit Admission and Mortality in Patients with Pneumonia (JAMA, 2015) [MEDLINE]
Among Medicare Beneficiaries Hospitalized with Pneumonia, Intensive Care Unit Admission of Patients for Whom the Decision Appeared to Be Discretionary was Associated with Improved Survival and No Significant Difference in Costs
Recommendations (American Thoracic Society and Infectious Diseases Society of America 2019 Clinical Practice Guidelines for the Diagnosis and Treatment of Adults with Community-Acquired Pneumonia) (Am J Respir Crit Care Med, 2019) [MEDLINE]
In Addition to Clinical Judgement, it is Recommended to Use a Validated Clinical Prediction Rule to Determine the Need for Hospitalization in Adults Diagnosed with Community-Acquired Pneumonia (Conditional Recommendation, Low Quality of Evidence)
Pneumonia Severity Index (PSI) is Preferred Over the CURB-65 (Tool Based on Confusion, Urea Level, Respiratory Rate, Blood Pressure, and Age >65) (Strong Recommendation, Moderate Quality of Evidence)
In Patient with Hypotension Requiring Vasopressors or Respiratory Failure Requiring Mechanical Ventilation, Intensive Care Unit Admission is Recommended (Strong Recommendation, Low Quality of Evidence)
In a Patient Not Requiring Vasopressors or Mechanical Ventilation, the Community-Acquired Pneumonia Minor Severity Criteria Below Combined with Clinical Judgment are Recommended to Guide the Need for Higher Levels of Treatment Intensity (Conditional Recommendation, Low Quality of Evidence)
Criteria for Severe Community-Acquired Pneumonia (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of CAP) (Clin Infect Dis, 2007) [MEDLINE]
General Comments
Validated Definition of Severe Community-Acquired Pneumonia Includes Either 1 Major Criterion or ≥3 Minor Criteria
VA Retrospective Cohort Study Examining the Impact of Azithromycin on Mortality and Cardiovascular Events in Older Patients Hospitalized with Pneumonia (JAMA, 2014) MEDLINE]: n = 73,690 patients (from 118 hospitals)
Azithromycin Decreased the 90-Day Mortality Rate, as Compared to Other Antibiotics
Azithromycin Also Demonstrated a Smaller Increased Risk of Myocardial Infarction, But No Difference in Arrhythmias or Congestive Heart Failure
CAP-START Trial-Antibiotic Choice in Non-ICU Community-Acquired Pneumonia (NEJM, 2015) [MEDLINE]
Empiric Treatment with β-Lactam Monotherapy was Non-Inferior to β-Lactam/Macrolide Combination or Fluoroquinolones with Respect to the 90-Day Mortality Rate
Large VA Retrospective Multicenter Cohort Study of the Impact of Empiric Anti-MRSA Antibiotic Therapy with Vancomycin (within the First Day of Hospitalization) in Patients Hospitalized for Community-Acquired Pneumonia (CAP) (JAMA Intern Med, 2020) [MEDLINE]: n = 88, 605 hospitalized patients (from 2008-2013)
Study Population: predominantly males (86 ,851 out of 88,605) with median age 70 years (interquartile range: 62-81 y/o)
Importantly, This Study Did Not Address Whether Whether MRSA Should Be Treated When it is Isolated
The Study Only Addressed Whether Empiric Antibiotic Therapy Against MRSA was Beneficial, as Compared to Standard Empiric Antibiotic Treatment Alone
Subgroup Analysis was Performed in Patients with Initial Intensive Care Unit Admission, MRSA Risk Factors, Positive Results of a MRSA Surveillance Test, and/or Positive Results of an MRSA Admission Culture
Empirical Anti-MRSA Therapy Plus Standard Therapy was Significantly Associated with an Increased Adjusted Risk of Death (Adjusted Risk Ratio 1.4; 95% CI: 1.3-1.5), Kidney Injury (Adjusted Risk Ratio 1.4; 95% CI: 1.3-1.5), and Secondary Clostridium Difficile Infections (Adjusted Risk Ratio 1.6; 95% CI: 1.3-1.9), Vancomycin-Resistant Enterococcus Species Infections (Adjusted Risk Ratio 1.6; 95% CI: 1.0-2.3), and Secondary Gram-Negative Rod Infections (Adjusted Risk Ratio 1.5; 95% CI: 1.2-1.8)
Empirical Anti-MRSA Antibiotic Therapy was Not Associated with Decreased 30-Day Mortality for Any Group of Patients Hospitalized for Pneumonia
Critiques/Limitations of the Study
This was a Retrospective Study, Not a Prospective Trial
The Study Evaluated Use of Vancomycin in 98% of Cases (with Minimal Data Related to the Use of Linezolid)
The Patients Treated with Anti-MRSA Antibiotic Regimens were Sicker (Had Higher Pneumonia Severity Indices, Had Higher Rates of Previous Hospitalization in Prior 90 Days, Had Higher Rates of Previous Antibiotics in Prior 60 Days, Had Higher ICU Admission Rates, etc) than Those Treated with Standard Antibiotic Regimens
Also, the Authors Readily Admitted that Treatment Effects (Whether Generated from Randomized Trials or Observational Studies) are Population Means and Individual Members of a Population May Vary Significantly in Terms of Outcomes from Different Treatments
Canadian Study of Adherence to Guideline-Recommended Empiric Antibiotic Therapy in the Hospital Treatment of Community-Acquired Pneumonia in Patients >65 y/o (Chest, 2023) [MEDLINE]: n = 1,909
Selection of Guideline-Concordant Antibiotic Therapy was Associated with a Trend Towards Lower All-Cause Mortality at 1 Year Post-Community-Acquired Pneumonia (Hazard Ratio 0.82; 95% CI: 0.65-1.04; P = 0.099)
Use of Guideline-Concordant Antibiotic Therapy was Associated with a Significant Almost 50% Reduction in Cardiovascular Death Risk 1 Year Post-Community-Acquired Pneumonia (Hazard Ratio 0.53; 95% CI: 0.34-0.80; P = 0.003)
Time to First Antibiotic Dose (TFAD)
Clinical Efficacy
Retrospective Medicare Study of Timing of Antibiotic Administration in Patients Hospitalized with CAP (Arch Intern Med, 2004) [MEDLINE]
Early Antibiotic Therapy Within 4 hrs is Associated with Decreased In-Hospital Mortality Rate, 30-Day Mortality Rate, and Hospital Length of Stay
Prospective Cohort Study of the Time to First Antibiotic Dose (within 4 hrs) in Community-Acquired Pneumonia (Clin Microbiol Infect, 2021) [MEDLINE]: n = 2,264
More than 80% of the Patients Had a Low Risk Pneumonia (with CURB-65 Score 0-2)
In All Models, the Administration of Antibiotics within 4 hrs of Admission Had No Significant Effect on the Outcomes
Adjusted Odds Ratios Derived from the Multivariable Models for 30-Day Mortality, Stability within 72 hrs and 30-Day Readmission were 1.01 (95% CI: 0.76-1.33), 0.88 (95% CI: 0.74-1.05) and 1.05 (95% CI: 0.82-1.34), Respectively
Adjusted Hazard Ratio for Time to Discharge was 1.00 (95% CI: 0.91-1.10)
Authors Recommended That Patients Should Be Triaged and Prioritized According to Age, Comorbidities, Clinical Condition, and Pneumonia Severity
Critiques
Although Study Evaluated a Large Number of Patients, the Cohort was Composed Mainly of Elderly Patients with Comorbidities, Which Could Account for the Relatively High Mortality Rate Observed in the Study
In Addition, the Criteria for CAP Diagnosis of Did Not Include Confirmation of Bacterial Etiology, Thus Non-Bacterial Episodes Could Have Been Included, Influencing the Results
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of CAP) (Clin Infect Dis, 2007) [MEDLINE]
For Patients Admitted Via the Emergency Department, First Antibiotic Dose Should Be Administered in the Emergency Department (Moderate Recommendation, Level III Evidence)
No Specific Length of Time for Antibiotic Administration was Specified in the Guidelines
Recommendations-Choice of Empiric Antibiotic Therapy (American Thoracic Society and Infectious Diseases Society of America 2019 Clinical Practice Guidelines for the Diagnosis and Treatment of Adults with Community-Acquired Pneumonia) (Am J Respir Crit Care Med, 2019) [MEDLINE]
Outpatient Adult without Comorbidities or Risk Factors for Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa
Amoxicillin (see Amoxicillin): 1 g PO TID (Strong Recommendation, Moderate Quality of Evidence)
Doxycycline (see Doxycycline): 100 mg PO BID (Conditional Recommendation, Low Quality of Evidence)
Macrolide (Azithromycin, Clarithromycin) (see Macrolides) (Conditional Recommendation, Moderate Quality of Evidence)
Use Macrolides Only in Regions with Streptococcus Pneumoniae Resistance (MIC ≥16 μg/mL) to Macrolides <25%
Azithromycin (see Azithromycin): 500 mg PO on first day, then 250 mg PO qday
Clarithromycin (see Clarithromycin): 500 mg PO BID (or extended-release 1000 mg PO qday)
Combination Therapy (Strong Recommendation, Moderate Quality of Evidence for Combination Therapy with Macrolides; Conditional Recommendation, Low Quality of Evidence for Combination Therapy with Doxycycline)
Outpatient Adult with Risk Factors for Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa (Prior Respiratory Isolation of Methicillin-Resistant Staphylococcus Aureus, Prior Respiratory Isolation of Pseudomonas Aeruginosa, or Recent Hospitalization with Intravenous Antibiotics in the Last 90 Days
Same as for Outpatient with Co-Morbidities (Chronic Heart/Lung/Liver/Renal Disease, Diabetes Mellitus, Alcoholism, Malignancy, Asplenia) with Added Coverage for Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa
However, Patients with Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa are Uncommonly Managed in the Outpatient Setting
Inpatient Adult with Suspected Aspiration Pneumonia
Routine Addition of Anaerobic Antibiotic Coverage for Suspected Aspiration Pneumonia is Not Recommended, Unless Lung Abscess or Empyema is Suspected (Conditional Recommendation, Very Low Quality of Evidence)
Inpatient Adult with Non-Severe Community-Acquired Pneumonia and Absence of Risk Factors for Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa
Monotherapy (Strong Recommendation, High Quality of Evidence)
Respiratory Fluoroquinolone
Levofloxacin (see Levofloxacin): 750 mg PO/IV qday
Moxifloxacin (see Moxifloxacin): 400 mg PO/IV qday
Combination Therapy (Strong Recommendation, High Quality of Evidence for Combination Therapy with Macrolide; Conditional Recommendation, Low Quality of Evidence for Combination Therapy with Doxycycline)
Inpatient Adult with Non-Severe Community-Acquired Pneumonia and Prior Respiratory Isolation of Methicillin-Resistant Staphylococcus Aureus (MRSA)
Background
The Use of the Prior Term, Healthcare-Associated Pneumonia (HCAP), to Guide Selection of Extended Antibiotic Coverage in Adults with Community-Acquired Pneumonia Should Be Abandoned (Strong Recommendation, Moderate Quality of Evidence)
Prior Identification of Methicillin-Resistant Staphylococcus Aureus (MRSA) in the Respiratory Tract within the Prior Year Predicts a Very High Risk of This Pathogen Being Identified in Patients Presenting with Community-Acquired Pneumonia
Monotherapy with Respiratory Fluoroquinolone or Combination β-Lactam and Macrolide (or Doxycycline): see above
Add Methicillin-Resistant Staphylococcus Aureus Coverage and Obtain Cultures/Nasal PCR to Allow Deescalation or Confirm Need for Continued Methicillin-Resistant Staphylococcus Aureus (MRSA) Therapy
Vancomycin (see Vancomycin): 15 mg/kg IV q12hrs (adjust based on levels)
Inpatient Adult with Non-Severe Community-Acquired Pneumonia and Recent Hospitalization with Intravenous Antibiotics and Locally Validated Risk Factors for Methicillin-Resistant Staphylococcus Aureus (i.e. Whether Methicillin-Resistant Staphylococcus Aureus is Prevalent in Patients with Community-Acquired Pneumonia and What Risk Factors for Infection are at a Local Hospital/Catchment Area Level) (Strong Recommendation, Moderate Quality of Evidence)
Background
The Use of the Prior Term, Healthcare-Associated Pneumonia (HCAP), to Guide Selection of Extended Antibiotic Coverage in Adults with Community-Acquired Pneumonia Should Be Abandoned (Strong Recommendation, Moderate Quality of Evidence)
There are No Validated Scoring Systems to Identify Patients with Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa with Sufficiently High Positive Predictive Value to Determine the Need for Empiric Extended-Spectrum Antibiotic Treatment (Due to Varying Prevalence of These Organisms in Different Populations and Lack of Benefit in Terms of Patient Outcome or Reduction in the Use of Broad-Spectrum Antibiotics)
However, as Noted Above (See Diagnostic), a Nasal Methicillin-Resistant Staphylococcus Aureus Culture Has a High Negative Predictive Value (i.e. Treatment for Methicillin-Resistant Staphylococcus Aureus (MRSA) Can Generally Be Withheld When the Nasal Methicillin-Resistant Staphylococcus Aureus (MRSA) is Negative, Especially in Non-Severe Community-Acquired Pneumonia)
If Clinicians are Currently Covering Empirically for Methicillin-Resistant Staphylococcus Aureus (MRSA) in Adults with Community-Acquired Pneumonia Based on Published Risk Factors, But Do Not Have Local Etiologic Data, Continuing Empiric Coverage While Obtaining Culture Data to Justify Continued Treatment is Recommended (Strong Recommendation, Low Quality of Evidence)
Monotherapy with Respiratory Fluoroquinolone or Combination β-Lactam and Macrolide (or Doxycycline): see above
Obtain Cultures, But Withhold Methicillin-Resistant Staphylococcus Aureus Coverage Unless Culture Results are Positive
If Methicillin-Resistant Staphylococcus Aureus Rapid Nasal PCR Testing is Negative, Withhold Additional Empiric Therapy Against Methicillin-Resistant Staphylococcus Aureus
If Methicillin-Resistant Staphylococcus Aureus Rapid Nasal PCR Testing is Positive, Add Methicillin-Resistant Staphylococcus Aureus Coverage and Obtain Cultures
Inpatient Adult with Non-Severe Community-Acquired Pneumonia and Prior Respiratory Isolation of Pseudomonas Aeruginosa
Background
The Use of the Prior Term, Healthcare-Associated Pneumonia (HCAP), to Guide Selection of Extended Antibiotic Coverage in Adults with Community-Acquired Pneumonia Should Be Abandoned (Strong Recommendation, Moderate Quality of Evidence)
Prior Identification of Pseudomonas Aeruginosa in the Respiratory Tract within the Prior Year Predicts a Very High Risk of This Pathogen Being Identified in Patients Presenting with Community-Acquired Pneumonia
Monotherapy with Respiratory Fluoroquinolone or Combination β-Lactam and Macrolide (or Doxycycline): see above
Add Coverage for Pseudomonas Aeruginosa and Obtain Cultures to Allow Deescalation or Confirmation of Need for Continued Pseudomonas Aeruginosa Therapy: does not include coverage for extended-spectrum β-lactamase–producing Enterobacteriaceae (which should be considered only on the basis of patient or local microbiological data)
Inpatient Adult with Non-Severe Community-Acquired Pneumonia and Recent Hospitalization with Intravenous Antibiotics and Locally Validated Risk Factors for Pseudomonas Aeruginosa (i.e. Whether Pseudomonas Aeruginosa is Prevalent in Patients with Community-Acquired Pneumonia and What Risk Factors for Infection are Present at a Local Hospital/Catchment Area Level) (Strong Recommendation, Moderate Quality of Evidence)
Background
The Use of the Prior Term, Healthcare-Associated Pneumonia (HCAP), to Guide Selection of Extended Antibiotic Coverage in Adults with Community-Acquired Pneumonia Should Be Abandoned (Strong Recommendation, Moderate Quality of Evidence)
There are No Validated Scoring Systems to Identify Patients with Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa with Sufficiently High Positive Predictive Value to Determine the Need for Empiric Extended-Spectrum Antibiotic Treatment (Due to Varying Prevalence of These Organisms in Different Populations and Lack of Benefit in Terms of Patient Outcome or Reduction in the Use of Broad-Spectrum Antibiotics)
If Clinicians are Currently Covering Empirically for Pseudomonas Aeruginosa in Adults with Community-Acquired Pneumonia Based on Published Risk Factors, But Do Not Have Local Etiologic Data, Continuing Empiric Coverage While Obtaining Culture Data to Justify Continued Treatment is Recommended (Strong Recommendation, Low Quality of Evidence)
Monotherapy with Respiratory Fluoroquinolone or Combination β-Lactam and Macrolide (or Doxycycline): see above
Obtain Cultures, But Initiate Pseudomonas Aeruginosa Coverage Only if Culture Results are Positive
Inpatient Adult with Severe Community-Acquired Pneumonia and Absence of Risk Factors for Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa
Combination Therapy (Strong Recommendation, Moderate Quality of Evidence for Combination Therapy with Macrolide; Strong Recommendation, Low Quality of Evidence for Combination Therapy with Respiratory Fluoroquinolone)
Azithromycin (see Azithromycin): 500 mg on first day, then 250 mg PO qday (or 500 mg IV qday x ≥5 days)
Clarithromycin (see Clarithromycin): 500 mg PO BID (or extended-release 1,000 mg PO qday)
Levofloxacin (see Levofloxacin): 750 mg PO/IV qday
Moxifloxacin (see Moxifloxacin): 400 mg PO/IV qday
Inpatient Adult with Severe Community-Acquired Pneumonia and with Prior Respiratory Isolation of Methicillin-Resistant Staphylococcus Aureus (MRSA) or Recent Hospitalization with Intravenous Antibiotics and Locally Validated Risk Factors for Methicillin-Resistant Staphylococcus Aureus (MRSA) Therapy (i.e. Whether Methicillin-Resistant Staphylococcus Aureus is Prevalent in Patients with Community-Acquired Pneumonia and What Risk Factors for Infection are Present at a Local Hospital/Catchment Area Level) (Strong Recommendation, Moderate Quality of Evidence)
Background
The Use of the Prior Term, Healthcare-Associated Pneumonia (HCAP), to Guide Selection of Extended Antibiotic Coverage in Adults with Community-Acquired Pneumonia Should Be Abandoned (Strong Recommendation, Moderate Quality of Evidence)
Prior Identification of Methicillin-Resistant Staphylococcus Aureus (MRSA) in the Respiratory Tract within the Prior Year Predicts a Very High Risk of This Pathogen Being Identified in Patients Presenting with Community-Acquired Pneumonia
There are No Validated Scoring Systems to Identify Patients with Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa with Sufficiently High Positive Predictive Value to Determine the Need for Empiric Extended-Spectrum Antibiotic Treatment (Due to Varying Prevalence of These Organisms in Different Populations and Lack of Benefit in Terms of Patient Outcome or Reduction in the Use of Broad-Spectrum Antibiotics)
However, as Noted Above (See Diagnostic), a Nasal Methicillin-Resistant Staphylococcus Aureus (MRSA) Culture Has a High Negative Predictive Value (i.e. Treatment for Methicillin-Resistant Staphylococcus Aureus Can Generally Be Withheld When the Nasal Methicillin-Resistant Staphylococcus Aureus (MRSA) is Negative, Especially in Non-Severe Community-Acquired Pneumonia)
If Clinicians are Currently Covering Empirically for Methicillin-Resistant Staphylococcus Aureus (MRSA) in Adults with Community-Acquired Pneumonia Based on Published Risk Factors, But Do Not Have Local Etiologic Data, Continuing Empiric Coverage While Obtaining Culture Data to Justify Continued Treatment is Recommended (Strong Recommendation, Low Quality of Evidence)
Combination β-Lactam and Macrolide (or Respiratory Fluoroquinolone): see above
Add Methicillin-Resistant Staphylococcus Aureus (MRSA) Coverage and Obtain Cultures/Nasal PCR to Allow Deescalation or Confirmation of Need for Continued Methicillin-Resistant Staphylococcus Aureus MRSA) Therapy
Vancomycin (see Vancomycin): 15 mg/kg IV q12hrs (adjust based on levels)
Inpatient Adult with Severe Community-Acquired Pneumonia and Prior Respiratory Isolation of Pseudomonas Aeruginosa or Recent Hospitalization with Intravenous Antibiotics and Locally Validated Risk Factors for Pseudomonas Aeruginosa (i.e. Whether Pseudomonas Aeruginosa is Prevalent in Patients with Community-Acquired Pneumonia and What Risk Factors for Infection are Present at a Local Hospital/Catchment Area Level) (Strong Recommendation, Moderate Quality of Evidence)
Background
The Use of the Prior Term, Healthcare-Associated Pneumonia (HCAP), to Guide Selection of Extended Antibiotic Coverage in Adults with Community-Acquired Pneumonia Should Be Abandoned (Strong Recommendation, Moderate Quality of Evidence)
Prior Identification of Pseudomonas Aeruginosa in the Respiratory Tract within the Prior Year Predicts a Very High Risk of This Pathogen Being Identified in Patients Presenting with Community-Acquired Pneumonia
There are No Validated Scoring Systems to Identify Patients with Methicillin-Resistant Staphylococcus Aureus (MRSA) or Pseudomonas Aeruginosa with Sufficiently High Positive Predictive Value to Determine the Need for Empiric Extended-Spectrum Antibiotic Treatment (Due to Varying Prevalence of These Organisms in Different Populations and Lack of Benefit in Terms of Patient Outcome or Reduction in the Use of Broad-Spectrum Antibiotics)
If Clinicians are Currently Covering Empirically for Pseudomonas Aeruginosa in Adults with Community-Acquired Pneumonia Based on Published Risk Factors, But Do Not Have Local Etiologic Data, Continuing Empiric Coverage While Obtaining Culture Data to Justify Continued Treatment is Recommended (Strong Recommendation, Low Quality of Evidence)
Combination β-Lactam and Macrolide (or Respiratory Fluoroquinolone): see above
Add Pseudomonas Aeruginosa Coverage and Obtain Cultures
Recommendations-Choice of Targeted Antibiotic Against a Specific Pathogen (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of CAP) (Clin Infect Dis, 2007) [MEDLINE]
Fluoroquinolone (see Fluoroquinolones): levofloxacin, moxifloxacin, gatifloxacin, ciprofloxacin
Switch from Intravenous to Oral Antibiotic Therapy
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of CAP) (Clin Infect Dis, 2007) [MEDLINE]
Patients Should Be Switched from Intravenous to Oral Antibiotic Therapy When They are Hemodynamically Stable and Improving Clinically, Able to Ingest Medications, and have a Normally Functioning Gastrointestinal Tract (Strong Recommendation, Level II Evidence)
Patients Should Be Discharged as Soon as they are Clinically Stable, Have No Other Active Medical Problems, and Have a Safe Environment for Continued Care (Moderate Recommendation, Level II Evidence): inpatient observation while receiving oral therapy is not necessary
Duration of Antibiotic Therapy
Clinical Efficacy
De-Escalation of Antibiotics (Curr Opin Pulm Med, 2006) [MEDLINE]
De-Escalation is an Effective Strategy to Limit Antibiotic Exposure During the Course of Pneumonia Treatment
Spanish Multicenter Randomized Trial of Shortened Antibiotic Course in Community-Acquired Pneumonia (JAMA Intern Med, 2016) [MEDLINE]: n = 312
Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS) Guideline for Shortened Antibiotic Course Based on Clinical Stability was Safely Implemented in Hospitalized Patients with CAP: patients in shortened course intervention group were treated for a minimum of 5 days and antibiotics were stopped if body temperature was <37.8 degrees C for 48 hrs and they had ≤1 CAP-associated sign of clinical instability (temperature ≥37.8 degrees C, heart rate ≥100 bpm, respiratory rate ≥24 breaths/min, systolic blood pressure ≤90 mm Hg, room air SaO2 ≤90% or pO2 ≤60, inability to maintain oral intake, or altered mental status)
Cochrane Database Systematic Review and Meta-Analysis of Using Serum Procalcitonin to Start or Stop Antibiotics in Acute Respiratory Tract Infection (Cochrane Database Syst Rev, 2017) [MEDLINE]
Use of Serum Procalcitonin to Guide Initiation and Duration of Antibiotics Results in Lower Risks of Mortality, Lower Antibiotic Consumption, and Lower Risk of Antibiotic-Associated Adverse Effects
Results were Similar for Different Clinical Settings and Types of Acute Respiratory Tract Infections
Future Research is Required to Confirm the Results in Immunocompromised Patients and Patients with Non-Respiratory Infections
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of CAP) (Clin Infect Dis, 2007) [MEDLINE]
Treatment for a Minimum of 5 Days is Recommended (Moderate Recommendation, Level I Evidence)
Patient Should Have for Temperature <37.8 degrees C for 48-72 hrs and Have ≤1 CAP-Associated Sign of Clinical Instability (Temperature ≥37.8 degrees C, Heart Rate ≥100 bpm, Respiratory Rate ≥24 breaths/min, Systolic Blood Pressure ≤90 mm Hg, Room Air SaO2 ≤90% or pO2 ≤60, Inability to Maintain Oral Intake, or Altered Mental Status) Prior to Antibiotic Discontinuation (Moderate Recommendation, Level II Evidence)
Longer Duration of Antibiotic Therapy May Be Required if Initial Antibiotic Therapy was Not Active Against the Identified Pathogen or if Pneumonia is Complicated by Extrapulmonary Infection (Meningitis, Endocarditis, etc) (Weak Recommendation, Level III Evidence)
Clinical Guidelines for Short-Course Antibiotics in Common Infections (Annals of Internal Medicine, 2021) [MEDLINE]
Clinicians Should Prescribe Antibiotics for Community-Acquired Pneumonia for a Minimum of 5 Days
Extension of Therapy After 5 Days of Antibiotics Should Be Guided by Validated Measures of Clinical Stability (Including Resolution of Vital Sign Abnormalities, Ability to Eat, and Normal Mentation)
Recommendations-Duration of Antibiotic Therapy (American Thoracic Society and Infectious Diseases Society of America 2019 Clinical Practice Guidelines for the Diagnosis and Treatment of Adults with Community-Acquired Pneumonia) (Am J Respir Crit Care Med, 2019) [MEDLINE]
Duration of Therapy Should Be Guided by Validated Measures of Clinical Stability (Resolution of Heart Rate/Respiratory Rate/Blood Pressure/Oxygen Saturation/Temperature Abnormalities), Ability to Eat, and Normal Mentation (Strong Recommendation, Moderate Quality of Evidence)
Antibiotic Therapy Should Be Continued Until the Patient Achieves Stability and For ≥5 Days (Strong Recommendation, Moderate Quality of Evidence)
Longer Antibiotic Courses are Recommended for the Following
Pneumonia Complicated by Endocarditis/Meningitis/Other Deep-Seated Infection
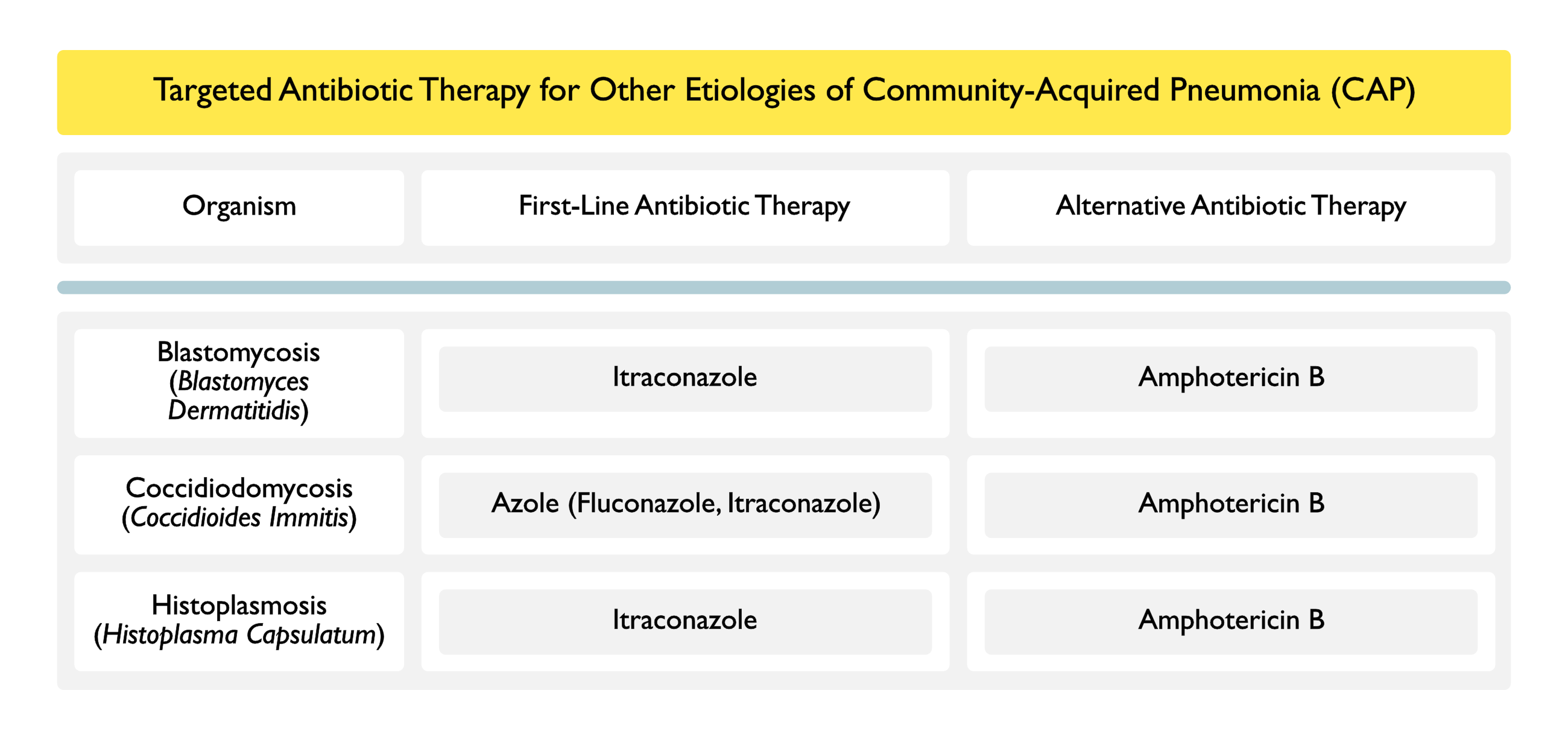
Infection with Less Common Pathogens Not Covered in These Guidelines (i.e. Burkholderia Pseudomallei, Mycobacterium Tuberculosis, Endemic Fungi, etc)
Duration of Therapy for Community-Required Pneumonia Due to Methicillin-Resistant Staphylococcus Aureus (MRSA) of Pseudomonas Aeruginosa Should Be 7 Days (in Agreement with the Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia Guidelines)
Reasons for Failure to Respond to Antibiotic Therapy (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of CAP) (Clin Infect Dis, 2007) [MEDLINE]
General Comments
Approximately 45% of Patients with Community-Acquired Pneumonia Who Ultimately Require Intensive Care Unit Admission are Initially Admitted to a Non-ICU Setting and are Transferred Due to Clinical Deterioration (Thorax, 2004) [MEDLINE]
Treatment of Concomitant Influenza and Community-Acquired Pneumonia (see Influenza Virus)
Recommendations-Choice of Empiric Antibiotic Therapy (American Thoracic Society and Infectious Diseases Society of America 2019 Clinical Practice Guidelines for the Diagnosis and Treatment of Adults with Community-Acquired Pneumonia) (Am J Respir Crit Care Med, 2019) [MEDLINE]
Outpatient Setting
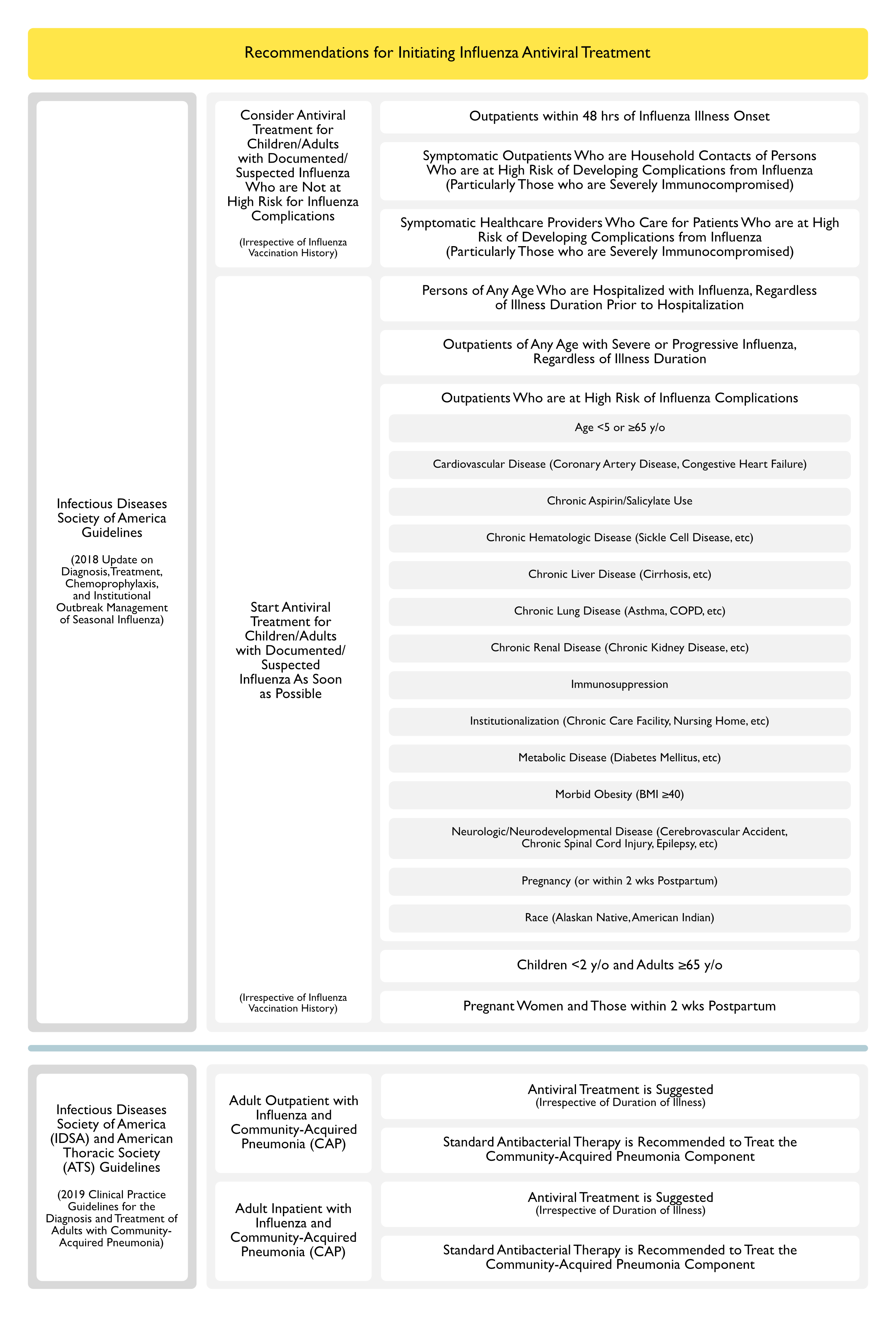
In Adults with Influenza and Community-Acquired Pneumonia, Anti-Influenza Treatment (Such as Oseltamivir) is Suggested, Independent of the Duration of Illness Before Diagnosis (Conditional Recommendation, Low Quality of Evidence)
In Adults with Concomitant Influenza and Clinical and Radiographic Evidence of Community-Acquired Pneumonia, Standard Antibacterial Therapy is Recommended to Treat the Community-Acquired Pneumonia in Both Outpatient/Inpatient Settings (Strong Recommendation, Low Quality of Evidence)
Inpatient Setting
In Adults with Influenza and Community-Acquired Pneumonia, Antiinfluenza Treatment (Such as Oseltamivir) is Recommended, Independent of the Duration of Illness Before Diagnosis (Strong Recommendation, Moderate Quality of Evidence)
In Adults with Concomitant Influenza and Clinical and Radiographic Evidence of Community-Acquired Pneumonia, Standard Antibacterial Therapy is Recommended to Treat the Community-Acquired Pneumonia in Both Outpatient/Inpatient Settings (Strong Recommendation, Low Quality of Evidence)
Routine Use of Corticosteroids is Not Recommended in Adults with Severe Influenza-Related Pneumonia (Conditional Recommendation, Low Quality of Evidence)
Corticosteroids Decrease the Length of Hospital Stay, But Did Not Decrease the Mortality Rate
Corticosteroids Decreased the Persistence of Chest X-Ray Abnormalities and Decreased the Incidence of Delayed Shock
Systematic Review and Meta-Analysis of Corticosteroids for Community-Acquired Pneumonia (CAP) (Chest, 2016) [MEDLINE]: n = 1,667 (from 9 randomized controlled trials) and n= 4,095 (from 6 cohort studies)
Mean Corticosteroid Dose and Treatment Duration were Methylprednisolone 30 mg/Day for 7 Days
Corticosteroids Did Not Have a Statistically Significant Effect on Mortality Rate (Relative Risk 0.72; 95% CI: 0.43-1.21; Evidence Rank, Low) in Patients with Community-Acquired Pneumonia and Patients with Severe Community-Acquired Pneumonia (Randomized Controlled Trials: Relative Risk 0.72; 95% CI: 0.43-1.21; Evidence Rank, Low; Cohort Studies: Relative Risk 1.00; 95% CI: 0.86-1.17)
Corticosteroids Treatment was Associated with a Decreased Risk of Acute Respiratory Distress Syndrome (ARDS) (Relative Risk 0.21; 95% CI: 0.08-0.59) and May Decrease Hospital Length of Stay, Intensive Care Unit Length of Stay, Duration of Intravenous Antibiotic Treatment, and Time to Clinical Stability
Corticosteroids were Not Associated with Increased Rates of Adverse Events
Corticosteroids Decreased Morbidity and Mortality in Adults with Severe Community-Acquired Pneumonia
The Number Needed to Treat for an Additional Beneficial Outcome was 18 Patients (95% CI: 12-49) to Prevent One Death
Non-Severe Community-Acquired Pneumonia
Corticosteroids Decreased Morbidity, But Not Mortality, for Adults and Children with Non-Severe Community-Acquired Pneumonia
Corticosteroids Were Associated with More Adverse Events (Especially Hyperglycaemia), But the Harms Did Not Seem to Outweigh the Benefits
Meta-Analysis Examining Corticosteroids in Community-Acquired Pneumonia (CAOP)/b> (Clin Infect Dis, 2018) [MEDLINE]: n = 1506 (from 6 trials)Corticosteroids Decreased the Time to Clinical Stability and Length of Hospital Stay by Approximately 1 Day Without a Decrease in MortalityCorticosteroids Increased the Risk for Community-Acquired Pneumonia-Related Rehospitalization and Hyperglycemia
Cost-Effectiveness of Corticosteroids in Community-Acquired Pneumonia (CAP) (Chest, 2019) [MEDLINE]
In the Base-Case Analysis, Corticosteroids and Antibiotics Resulted in Savings of $142,795 Per Death Averted
In the Probabilistic Analysis, at a Willingness to Pay of $50,000, Combination Corticosteroids and Antibiotics Had a 86.4% Chance of Being Cost-Effective, as Compared to Combination of Placebo and Antibiotics
In Cost-Effectiveness Acceptability Curves, the Combination of Corticosteroids and Antibiotics Strategy was Cost-Effective in 87.6-94.3% of Simulations, as Compared with the Combination Placebo and Antibiotics Strategy for a Willingness to Pay Ranging from $0-50,000
In Patients with Severe CAP (Pneumonia Severity Index Classes IV and V) the Corticosteroids and Antibiotics Strategy Resulted in Savings of $70,587 and Had a 82.6% Chance of Being Cost-Effective, as Compared to the Combination Placebo and Antibiotics Strategy
Conclusion
Combination Corticosteroids and Antibiotics is a Cost-Effective Strategy and Results in Considerable Healthcare Cost-Savings, Especially in Patients with Severe Community-Acquired Pneumonia (Pneumonia Severity Index Classes IV and V)
Systematic Review, Meta-analysis, and Meta-Regression of Randomized Control Trials of Corticosteroid Treatment in Community-Acquired Pneumonia (CAP) (Chest, 2023) [MEDLINE]: n = 3,842 (16 studies)
All-Cause Mortality (16 Studies [3,842 Patients]; Risk Ratio 0.85 [95% Confidence Interval: 0.67-1.07]; P = 0.17; I2 = 14%; Trial Sequential Analysis-Adjusted Confidence Interval: 0.61-1.09), ICU Admission (6 Studies [2,619 Patients]; Risk Ratio 0.66 [95% CI, 0.45-0.97]; P = 0.04; I2 = 0%; Trial Sequential Analysis-Adjusted Confidence Interval: 0.37-1.12), Treatment Failure (6 Studies [2,093 Patients]; Risk Ratio 0.78 [95% CI, 0.37-1.67]; P = 0.52; I2 = 68%; Trial Sequential Analysis-Adjusted Confidence Interval: 0.02-25.5), and the Incidence of Adverse Events (6 Studies [2,487 Patients]; Risk Ratio 1.10 [95% CI, 0.97-1.25]; P = .14; I2 = 53%; Trial Sequential Analysis-Adjusted Confidence Interval: 0.82-2.41) were Similar Between Patients Receiving Corticosteroids and Patients Assigned to the Control Group
The Need for Mechanical Ventilation (8 Studies [1,457 Patients]; Risk Ratio 0.51 [95% Confidence Interval: 0.33-0.77]; P = 0.001; I2 = 0%; Trial Sequential Analysis-Adjusted Confidence Interval: 0.20-0.85) was Lower Among Patients Receiving Corticosteroids, as Compared with those Receiving Standard Care
However, Corticosteroid Use May Be Associated with Higher Rates of Hospital Readmission (5 Studies [2,853 Patients]; Risk Ratio 1.20 [95% CI: 1.05-1.38]; P = 0.008; I2 = 0%; Trial Sequential Analysis-Adjusted Confidence Interval: 0.89-1.98)
Conclusions
Corticosteroid Therapy is Associated with a Lower Incidence of Progression to Requiring Mechanical Ventilation in Patients Hospitalized with Community-Acquired Pneumonia
Corticosteroid Therapy was Not Associated with Decreased Mortality, Decreased Treatment Failure, or Increased Risk of Adverse Events
French CAPE COD Multicenter, Randomized, Double-Blind, Phase 3 Trial of Hydrocortisone (200 mg IV qDay x Either 4 or 8 Days as Determined by Clinical Improvement, Followed by Tapering for a Total of 8-14 Days) in Severe Community-Acquired Pneumonia (CAP) in Adults Admitted to the Intensive Care Unit (NEJM, 2023) [MEDLINE]; n = 800 (trial stopped after the second planned interim analysis, data from 795 patients was analyzed)
28-Day Mortality Rate was 6.2% (95% CI: 3.9 to 8.6) in the Hydrocortisone Group and 11.9% (95% CI: 8.7-15.1) in the Placebo Group (Absolute Difference -5.6 Percentage Points; 95% CI: -9.6 to -1.7; P = 0.006)
Among the Patients Who were Not Undergoing Mechanical Ventilation at Baseline, Endotracheal Intubation was Performed in 18.0% of Patients in the Hydrocortisone Group and in 29.5% of Patients in the Placebo Group (Hazard Ratio 0.59; 95% CI: 0.40-0.86)
Among the Patients Who were Not Receiving Vasopressors at Baseline, Vasopressor Therapy was Initiated by Day 28 in 15.3% of Patients in Hydrocortisone Group and 25.0% of Patients in the Placebo Group (Hazard Ratio 0.59; 95% CI: 0.43-0.82)
Adverse Events
Frequencies of Hospital-Acquired Infections and Gastrointestinal Bleeding were Similar in the Two Groups
Patients in the Hydrocortisone Group Received Higher Daily Doses of Insulin During the First Week of Treatment
Systematic Review and Meta-Analysis of Randomized Controlled Trials Studying Corticosteroids in Severe Community-Acquired Pneumonia (CAP) (Crit Care, 2023) [MEDLINE]: n = 1,689
Overall, Study Group Had a Lower 30-Day Mortality Rate than the Control Group (Risk Ratio 0.61; 95% CI: 0.44-0.85; p < 0.01) with low heterogeneity (I2 = 0%, p = 0.42)
Compared to the Control Group, Study Group Had a Lower Risk of the Requirement for Mechanical Ventilation (Risk Ratio 0.57; 95% CI: 0.45-0.73; p < 0.001), Shorter Intensive Care Unit Length of Stay (MD – 0.8; 95% CI: – 1.4 to – 0.1; p = 0.02), and Shorter Hospital Length of Stay (MD – 1.1; 95% CI: – 2.0 to – 0.1; p = 0.04)
Finally, No Significant Difference was Observed Between the Study and Control Groups in Terms of Gastrointestinal Tract Bleeding (Risk Ratio 1.03; 95% CI: 0.49-2.18; p = 0.93), Healthcare-Associated Infection (Risk Ratio 0.89; 95% CI: 0.60-1.32; p = 0.56), and Acute Kidney Injury (RR 0.68; 95% CI 0.21-2.26; p = 0.53)
Conclusions
In Patients with Severe Community-Acquired Pneumonia (CAP), Adjunctive Corticosteroids Can Provide Survival Benefits and Improve Clinical Outcomes without Increasing Adverse Events
However, Because the Pooled Evidence Remains Inconclusive, Further Studies are Required
Recommendations (American Thoracic Society and Infectious Diseases Society of America 2019 Clinical Practice Guidelines for the Diagnosis and Treatment of Adults with Community-Acquired Pneumonia) (Am J Respir Crit Care Med, 2019) [MEDLINE]
Routine Use of Corticosteroids is Not Recommended in Adults with Non-Severe Community-Acquired Pneumonia (Strong Recommendation, High Quality of Evidence) or Severe Community-Acquired Pneumonia (Conditional Recommendation, Moderate Quality of Evidence)
Routine Use of Corticosteroids is Not Recommended in Adults with Severe Influenza-Related Pneumonia (Conditional Recommendation, Low Quality of Evidence)
In the Setting of Refractory Septic Shock, Surviving Sepsis Recommendations for the Use of Corticosteroids are Recommended
Of Note, There is No Intent that the Above Recommendations Should Override Clinically Appropriate Use of Corticosteroids for Comorbid Diseases, Such as Chronic Obstructive Pulmonary Disease, Asthma, and Autoimmune Disease, in Which Corticosteroids are Supported as a Component of Treatment
Hemodynamic Support
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of Community-Acquired Pneumonia) (Clin Infect Dis, 2007) [MEDLINE]
Severe Community-Acquired Pneumonia with Hypotension Requiring Intravenous Fluid Resuscitation Should Be Screened for Occult Adrenal Insufficiency (Moderate Recommendation, Level II Evidence)
Recommendations (Infectious Diseases Society of America, IDSA/American Thoracic Society, ATS 2007 Consensus Guidelines for the Management of Community-Acquired Pneumonia) (Clin Infect Dis, 2007) [MEDLINE]
CAP Patients with Hypoxemia/Acute Respiratory Failure Should Receive a Cautious Trial of Noninvasive Positive-Pressure Ventilation (NIPPV) Unless They Require Immediate Intubation Due to Severe Hypoxemia (pO2/FiO2 Ratio <150) and Bilateral Alveolar Infiltrates (Moderate Recommendation, Level I Evidence) (see Noninvasive Positive-Pressure Ventilation)
Low Tidal Volume Ventilation (6 mL/kg PBW) is Recommended for Mechanical Ventilation of CAP Patients with Diffuse Bilateral Pneumonia or ARDS (Strong Recommendation, Level I Evidence)
Oxygen Should Be Prescribed to Achieve a Target Saturation of 94–98% for Most Acutely Ill Patients or 88–92% or Patient-Specific Target Range for Those at Risk of Hypercapnic Respiratory Failure
Best Practice is to Prescribe a Target Range for All Hospitalized Patients at the Time of Hospital Admission So that Appropriate Oxygen Therapy Can Be Started in the Event of Unexpected Clinical Deterioration with Hypoxemia and Also to Ensure that the Oximetry Section of the Early Warning Score Can Be Scored Appropriately
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
Supplemental Oxygen Therapy Should Be Titrated to SpO2 ≤96% (Strong Recommendation)
SpO2 >96% likely is Associated with a Small, But Important, Increased Risk of Death without Plausible Clinical Benefit
Follow-Up Chest Imaging After an Episode of Community-Acquired Pneumonia (CAP)
Recommendations-Follow-Up Chest Imaging (American Thoracic Society and Infectious Diseases Society of America 2019 Clinical Practice Guidelines for the Diagnosis and Treatment of Adults with Community-Acquired Pneumonia) (Am J Respir Crit Care Med, 2019) [MEDLINE]
In Adults with Community-Acquired Pneumonia Whose Symptoms Have Resolved within 5-7 Days, Routinely Follow-Up Chest Imaging is Not Recommended (Conditional Recommendation, Low Quality of Evidence
Reported Rates of Malignancy in Patients Recovering from Community-Acquired Pneumonia Range from 1.3-4%
Almost All Patients with Malignancy in the Reported Series were Smokers or Ex-Smokers
Prognosis
Factors Associated with Hospital Readmission for Community-Acquired Pneumonia
Clinical Data
Study of Factors Related to Hospital Readmission for Pneumonia (Clin Infect Dis, 2013) [MEDLINE]
Hospital Readmission Rate for Pneumonia: 20%
Patients with HCAP were 7.5x More Likely to Be Readmitted than Patients with CAP
Criteria in HCAP that Associated with the Risk of Hospital Readmission
Admission from Long-term Care (adjusted odds ratio [AOR], 2.2 [95% CI, 1.4-3.4])
Presence of Heart Failure Increases the Mortality Rate of Community-Acquired Pneumonia
Clinical Data
Retrospective Cohort Study of Comorbidities in Patients with Community-Acquired Pneumonia (Am J Med Open, 2022) [MEDLINE]: n = 783,702 (61 US hospitals)
27% of Patients Had a Diagnosis of Heart Failure
Of These, 26.5% Had Acute Heart Failure, 22.7% Had Chronic Heart Failure, and 51% Had a Diagnosis of Unspecified Heart Failure
In Multivariable-Adjusted Models, Having Any Heart Failure was Associated with Increased Mortality (Odds Ratio 1.35; 95% CI: 1.33 – 1.38), as Compared to Those without Heart Failure
Increased Mortality was Associated with Acute Heart Failure (Odds Ratio 1.19; 95% CI: 1.15 – 1.22), But Not Chronic Heart Failure (Odds Ratio 0.92, 95% CI: 0.89 – 0.96)
Machine Learning Models May Allow Prediction of Mortality in Community-Acquired Pneumonia
Clinical Data
Study of Machine Learning Model for Prediction in Community-Acquired Pneumonia (Chest, 2022) [MEDLINE]: n = 4,531 (derivation cohort) and n = 1,034 (validation cohort)
In the Derivation Cohort, the Areas Under the Curve of SepsisFinder Adapted for Community-Acquired Pneumonia (SeF-ML), CURB-65, SOFA, PSI, and qSOFA were 0.801, 0.759, 0.671, 0.799, and 0.642, Respectively, for 30-Day Mortality Prediction
In the Validation Study, the Area Under the Curve of SepsisFinder Adapted for Community-Acquired Pneumonia (SeF-ML) was 0.826, Concordant with the Area Under the Curve (0.801) in the Derivation Data (P = 0.51)
The Area Under the Curve of SepsisFinder Adapted for Community-Acquired Pneumonia (SeF-ML) was Significantly Higher than Those of CURB-65 (0.764; P = .03) and qSOFA (0.729, P = .005)
However, it Did Not Differ Significantly from Those of PSI (0.830; P = .92) and SOFA (0.771; P = .14)
SepsisFinder Adapted for Community-Acquired Pneumonia (SeF-ML) Shows Potential for Improving Mortality Prediction in Patients with Community-Acquired Pneumonia, Using Structured Health Data
Risk of Future Cognitive Dysfunction
In a Study of Pneumonia and Cognitive Dysfunction, Small Subclinical Changes in Cognition Increased the Risk of Pneumonia (β= -0.02; P < 0.001) and Patients with Pneumonia were Subsequently at an Increased Risk of Dementia (Hazard Ratio of 2.24; 95% CI: 1.62-3.11]; P = 0.01) (Am J Respir Crit Care Med, 2013) [MEDLINE]
References
Treatment
General
The cost of treating community-acquired pneumonia. Clin Ther 1998; 20: 820–37 [MEDLINE]
Severity assessment tools to guide ICU admission in community-acquired pneumonia: systematic review and meta-analysis. Intensive Care Med 2011;37:1409–1420 [MEDLINE]
Association of Intensive Care Unit Admission With Mortality Among Older Patients With Pneumonia. JAMA. 2015 Sep 22-29;314(12):1272-9. doi: 10.1001/jama.2015.11068 [MEDLINE]
Antibiotics
Variations in etiology of ventilator-associated pneumonia across four treatment sites: implications for antimicrobial prescribing practices. Am J Respir Crit Care Med. 1999;160(2):608-613 [MEDLINE]
PneumA Trial. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290(19):2588-2598 [MEDLINE]
Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community-acquired pneumonia. Arch Intern Med 2004; 164:637–44 [MEDLINE]
Antimicrobial stewardship programs: mandatory for all ICUs. Crit Care. 2012;16:179. doi:10.1186/cc11853 [MEDLINE]
Impact of regular collaboration between infectious diseases and critical care practitioners on antimicrobial utilization and patient outcome. Crit Care Med. 2013;41:2099–2107. doi: 10.1097/CCM.0b013e31828e9863 [MEDLINE]
Efficacy of single-dose antibiotic against early-onset pneumonia in comatose patients who are ventilated. Chest. 2013 May;143(5):1219-25. doi: 10.1378/chest.12-1361 [MEDLINE]
Antibiotic stewardship in hospital-acquired pneumonia. Chest. 2013;143:1195–1196. doi:10.1378/chest.12-2729 [MEDLINE]
Association of azithromycin with mortality and cardiovascular events among older patients hospitalized with pneumonia. JAMA. 2014 Jun 4;311(21):2199-208. doi: 10.1001/jama.2014.4304 [MEDLINE]
What can be expected from antimicrobial de-escalation in the critically ill? Intensive Care Med 2014; 40:92–5 [MEDLINE]
CAP-START Trial. Antibiotic treatment strategies for community-acquired pneumonia in adults. N Engl J Med. 2015 Apr 2;372(14):1312-23. doi: 10.1056/NEJMoa1406330 [MEDLINE]
A Systematic Review of the Definitions, Determinants, and Clinical Outcomes of Antimicrobial De-escalation in the Intensive Care Unit. Clin Infect Dis. 2016 Apr 15;62(8):1009-17. doi: 10.1093/cid/civ1199 [MEDLINE]
Duration of Antibiotic Treatment in Community-Acquired Pneumonia. A Multicenter Randomized Clinical Trial. JAMA Intern Med. 2016 Jul 25. doi: 10.1001/jamainternmed.2016.3633 [MEDLINE]
Clinical Practice Guidelines by the Infectious Diseases Society of America: 2018 Update on Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management of Seasonal Influenza. Clin Infect Dis. 2019;68(6):e1 [MEDLINE]
Empirical Anti-MRSA vs Standard Antibiotic Therapy and Risk of 30-Day Mortality in Patients Hospitalized for Pneumonia. JAMA Intern Med. 2020 Feb 17. doi: 10.1001/jamainternmed.2019.7495 [MEDLINE]
Appropriate Use of Short-Course Antibiotics in Common Infections: Best Practice Advice From the American College of Physicians. Ann Intern Med. 2021 Apr 6. doi: 10.7326/M20-7355 [MEDLINE]
Time to antibiotic administration and patient outcomes in community-acquired pneumonia: results from a prospective cohort study. Clin Microbiol Infect. 2021 Mar;27(3):406-412. doi: 10.1016/j.cmi.2020.08.037 [MEDLINE]
Time to first antibiotic dose for community-acquired pneumonia: a challenging balance. Clin Microbiol Infect. 2021 Mar;27(3):322-324. doi: 10.1016/j.cmi.2020.10.025 [MEDLINE]
Guideline-Concordant Antibiotic Therapy for the Hospital Treatment of Community-Acquired Pneumonia and 1-Year All-Cause and Cardiovascular Mortality in Older Adult Patients Surviving to Discharge. Chest. 2023 Jun;163(6):1380-1389. doi: 10.1016/j.chest.2022.12.035 [MEDLINE]
Adjuvant steroid therapy in community-acquired pneumonia: a systematic review and meta-analysis. J Hosp Med. 2013 Feb;8(2):68-75 [MEDLINE]
Efficacy and Safety of Corticosteroids for Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis. Chest. 2016 Jan;149(1):209-19. doi: 10.1378/chest.15-1733 [MEDLINE]
Corticosteroids for pneumonia. Cochrane Database Syst Rev. 2017 Dec 13;12:CD007720. doi: 10.1002/14651858.CD007720.pub3 [MEDLINE]
Corticosteroids in Patients Hospitalized With Community-Acquired Pneumonia: Systematic Review and Individual Patient Data Metaanalysis. Clin Infect Dis. 2018 Jan 18;66(3):346-354. doi: 10.1093/cid/cix801 [MEDLINE]
The Cost-Effectiveness of Corticosteroids for the Treatment of Community-Acquired Pneumonia. Chest. 2019 Apr;155(4):787-794. doi: 10.1016/j.chest.2018.11.001 [MEDLINE]
Effect of Corticosteroids on Mortality and Clinical Cure in Community-Acquired Pneumonia: A Systematic Review, Meta-analysis, and Meta-regression of Randomized Control Trials. Chest. 2023 Mar;163(3):484-497. doi: 10.1016/j.chest.2022.08.2229. Epub 2022 Sep 7 [MEDLINE]
Hydrocortisone in Severe Community-Acquired Pneumonia. N Engl J Med. 2023 Mar 21. doi: 10.1056/NEJMoa2215145 [MEDLINE]
Efficacy and safety of adjunctive corticosteroids in the treatment of severe community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials. Crit Care. 2023 Jul 8;27(1):274. doi: 10.1186/s13054-023-04561-z [MEDLINE]
Respiratory Support
Acute respiratory failure in patients with severe community-acquired pneumonia. A prospective randomized evaluation of noninvasive ventilation. Am J Respir Crit Care Med. 1999 Nov;160(5 Pt 1):1585-91 [MEDLINE]
Non-invasive mechanical ventilation in acute respiratory failure due to chronic obstructive pulmonary disease: correlates for success. Thorax. 1995 Jul;50(7):755-7 [MEDLINE]
Predictors of failure of noninvasive ventilation in patients with severe community-acquired pneumonia. J Crit Care. 2010 Sep;25(3):540.e9-14. doi: 10.1016/j.jcrc.2010.02.012 [MEDLINE]
The role of noninvasive positive pressure ventilation in community-acquired pneumonia. J Crit Care. 2015 Feb;30(1):49-54. doi: 10.1016/j.jcrc.2014.09.021. Epub 2014 Oct 2 [MEDLINE]
British Thoracic Society Emergency Oxygen Guideline Group BTS Emergency Oxygen Guideline Development Group. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax 2017;72(Suppl 1):ii1-90. 10.1136/ thoraxjnl-2016-209729 pmid:28507176 [MEDLINE]
Oxygen therapy for acutely ill medical patients: a clinical practice guideline. BMJ. 2018 Oct 24;363:k4169. doi: 10.1136/bmj.k4169 [MEDLINE]
Prognosis
Readmission following hospitalization for pneumonia: the impact of pneumonia type and its implication for hospitals. Clin Infect Dis. 2013 Aug;57(3):362-7 [MEDLINE]
Editorial commentary: “excess readmissions” for pneumonia: a dilemma with a penalty. Clin Infect Dis. 2013 Aug;57(3):368-9 [MEDLINE]
Machine-learning model for mortality prediction in patients with community-acquired pneumonia: development and validation study. Chest. Published online July 15, 2022:S0012-3692(22)01243-0. doi:10.1016/j.chest.2022.07.005 [MEDLINE]
Acute but not chronic heart failure is associated with higher mortality among patients hospitalized with pneumonia: An analysis of a nationwide database. Am J Med Open. 2022 Jun;7:100013. doi: 10.1016/j.ajmo.2022.100013 [MEDLINE]