Common Cold is the Most Frequent Acute Illness in the United States and in the Industrialized World (Prim Care, 1996) [MEDLINE]
Preschool Children Have an Average Incidence of 5-7 Common Cold Episodes Per Year (Epidemiol Rev, 1994) [MEDLINE]
Absences from School Amount to 26 Million Days Annually (Allergy Asthma Immunol, 1997) [MEDLINE]
Adults Have an Average Incidence of 2-3 Common Cold Episodes Per Year (Epidemiol Rev, 1994) [MEDLINE]
Absences from Work Amount to 23 Million Days Annually (Allergy Asthma Immunol, 1997) [MEDLINE]
Economic Burden of the Common Cold
Common Cold is Associated with a Significant Loss of Work Productivity and Substantial Medical Expenditures (Ann Allergy Asthma Immunol, 1997) [MEDLINE]
Approximately 500 Million Non-Influenza Viral Respiratory Illnesses were Reported (Between 2000-2001) (Arch Intern Med, 2003) [MEDLINE]
Accounted for Direct Costs of $17 Billion Annually
Accounted for Indirect Costs of $22.5 Billion Annually
Seasonal Variation in Incidence of the Common Cold
Approximately 200 Viruses are Associated with the Common Cold
During a Single Season, a Single Antigenic Type of Virus Accounts for Only <1% of Colds
It is Generally Not Possible to Determine the Viral Pathogen Based on the Clinical Symptoms, as All of the Viral Etiologies May Result in Similar Symptoms (Epidemiol Infect, 1993) [MEDLINE]
Most of the Respiratory Viruses Which Cause the Common Colds are Capable of Reinfection after Reexposure (Prim Care, 1996) [MEDLINE]
However, Subsequent Infections with the Same (or Similar) Virus are Clinically Milder and of Shorter Duration (J Clin Invest, 1959) [MEDLINE]
The Molecular Mechanism for Incomplete Immunity Following Infection with One Common Cold Virus Strain is Not Well-Understood, But Data from Rhinoviruses Suggest that it May Involve the Significant Degree of Structural and Molecular Variability within Serotypes and Between Divergent Strains Which Result from Mutation of a Given Reference Virus Strain (Science, 2009) [MEDLINE]
Bocaviruses are Members of the Parvovirus (Parvoviridae) Family (see Parvoviruses)
Human Bocavirus 1 (1HBoV1) was Discovered in 2005
HBoV1 is Associated with Respiratory Disease in Children (Common Cold, Acute Otitis Media, Pneumonia, Bronchiolitis, and Asthma Exacerbation) (Lancet Child Adolesc Health, 2019) [MEDLINE]
Other Bocaviruses were Subsequently Discovered in 2009-2010
Small Particle Droplets (Droplet Nuclei or Aerosols) Which Become Airborne Via Coughing or Sneezing
Large Particle Droplets (Classic Droplet Transmission) Which Require Close Contact with an Infected Person
Hand Contact (Via COntact with an Infected Person or Via Indirect Contact with a Contaminated Surface
Virus Viability
Common Cold Viruses Remain Viable on the Surface of the Skin for Up to 2 hrs
Rhinovirus Remains Viable on Environmental Surfaces for Several Hours
Porous Materials (Tissues, Cotton Handkerchiefs) are Poor Substrates for Viral Survival and, Therefore, are Inefficient Modes of Common Cold Viral Transmission
Decontamination of Surfaces with Virucidal Disinfectants (Phenol, Alcohol, etc) Decrease the Risk of Common Cold Viral Transmission
Unsurprisingly, Use of Antibacterial Home Cleaning Products Did Not Impact the Incidence of Respiratory Symptoms in Study Patients, as Compared to Standard Cleaning Products (Ann Intern Med, 2004) [MEDLINE]
Saliva is a Poor Mode of Common Cold Viral Transmission, as >90% of Patients with Common Cold Have No Detectable Virus in Their Saliva (Prim Care, 1996) [MEDLINE]
Impact of Airplane Air Recirculation on Incidence of the Common Cold
Aircraft Cabin Air Recirculation Did Not Increase the Risk of Upper Respiratory Tract Symptoms in Passengers Traveling on Commercial Jet Airplanes (JAMA, 2002) [MEDLINE]
Period of Infectivity
With Rhinovirus, Peak Viral Shedding Occurs on the 2nd Day of Illness (Am Rev Respir Dis, 1966) [MEDLINE] (J Clin Virol, 2004) [MEDLINE]
Peak Viral Shedding Occurs on the 3rd Day of the Illness After Inoculation (This is the Period of Peak Symptoms)
Lower Levels of Viral Shedding May Persist for as Long as 2 wks
Period of Viral Shedding Does Not Correlate with the Period of Clinical Disease
In Rhinovirus Infection, Asymptomatic Viral Shedding is Common
Positive Rhinovirus PCR Has Been Reported in 6% of Asymptomatic Adults and 35% of Asymptomatic Children at Any Given Point in Time (mSphere, 2018) [MEDLINE] (Pediatrics, 2014) [MEDLINE] (J Infect Dis, 2018) [MEDLINE]
In Any Patient Presenting with an Acute Respiratory Illness, an Oropharyngeal Swab with Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) Testing for SARS-CoV-2 is Required for the Purpose of Infection Control
Note that in Rhinovirus Infection, Asymptomatic Viral Shedding is Common, Making Multiplex Testing of Unclear Utility (Since No Specific Therapy is Available, Regardless)
Positive Rhinovirus PCR Has Been Reported in 6% of Asymptomatic Adults and 35% of Asymptomatic Children at Any Given Point in Time (mSphere, 2018) [MEDLINE] (Pediatrics, 2014) [MEDLINE] (J Infect Dis, 2018) [MEDLINE]
Nasal Bacterial Cultures are Not Recommended For Evaluation of the Common Cold
Study of Nasal Bacterial Cultures (Nasal Aspirate) in Patients with Common Cold (Lancet, 1996) [MEDLINE]
Only 61 Out of 300 Patients Had Nasal Bacterial Cultures Positive for Potential Pathogens (Haemophilus Influenzae, Moraxella Catarrhalis, or Streptococcus Pneumoniae)
In Terms of Symptom Scores, Antibiotic Therapy (Amoxicillin-Clavulanate) Benefited Patients Only in This Group
While Not Standardly Used, Serum Procalcitonin May Help Avoid Unneccesary Antibiotic Exposure in the Outpatient Management of Upper Respiratory Tract Infections
Clinical Efficacy
Procalcitonin Use Decreased Antibiotic Use in the Treatment of Respiratory Tract Infections the Primary Care Setting (Arch Intern Med, 2008) [MEDLINE] (Clin Chem Lab Med, 2017) [MEDLINE]
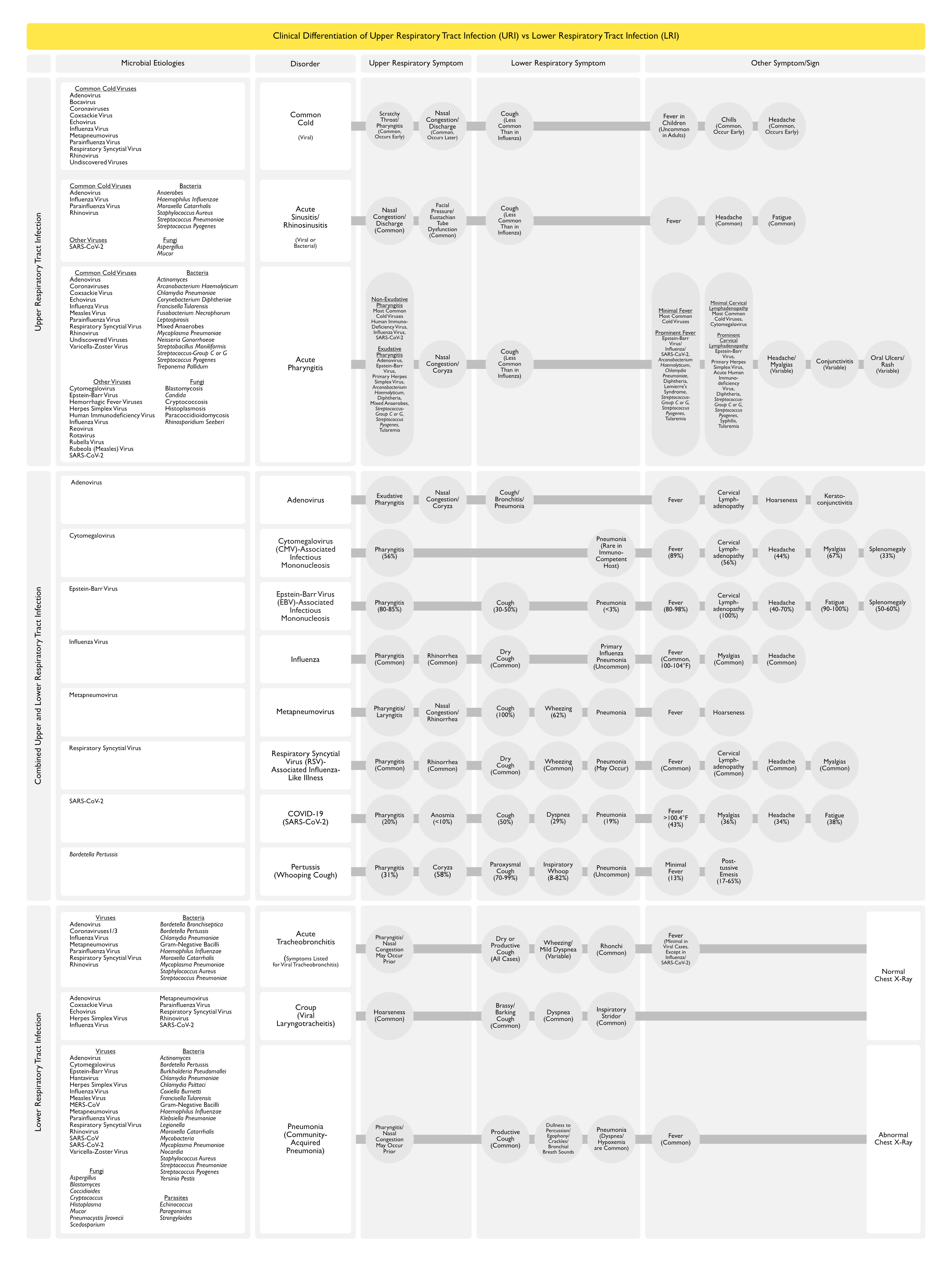
Clinical Differentiation of Upper Respiratory Tract Infection vs Lower Respiratory Tract Infection
Anatomy
General Comments
Although Not Universally Agreed Upon, the Larynx Separates the Upper and Lower Respiratory Tracts
Upper vs Lower Respiratory Tract
Upper Respiratory Tract is Generally Includes the Nasal Cavity, Pharynx, and Larynx
Lower Respiratory Tract is Generally Includes the Larynx, Bronchi, Bronchioles, and Alveoli of the Lungs
Combined Upper and Lower Respiratory Tract Infections May Involve Both the Upper and Lower Respiratory Tracts
Clinical Manifestations
General Comments
Incubation Period
Incubation Period: 24-72 hrs
However, in Experimental Settings, Incubation Periods as Short as 10-12 hrs Have Been Observed (Lancet, 2003) [MEDLINE]
Clinical Course
Symptoms Increase Rapidly (Peaking 2-3 Days After Infection) (Lancet Infect Dis, 2005) [MEDLINE]
Symptoms of the Common Cold are Generally Due to the Immune Response to Infection, Rather than Direct Viral Damage to the Respiratory Tract
In Contrast, Influenza Virus Causes Damage to Respiratory Epithelium (see Influenza Virus) (J Virol, 2018) [MEDLINE]
Intensity and Type of Clinical Symptoms of the Common Cold May Be Related to the Type of infecting Virus and Host Factors (Including Age, Underlying Illness, and Prior Immunological Experience) (Lancet Infect Dis, 2005) [MEDLINE]
Consequently, Upper Respiratory Tract Infections May Be Asymptomatic, May Be Associated with an Acute Self-Limiting Illness, or May Be Lethal
Jackson Cold Scale (AMA Arch Intern Med, 1958) [MEDLINE]
Sensitivity: 81%
Specificity: 66%
Wisconsin Upper Respiratory Symptom Survey (WURSS) (Health Qual Life Outcomes, 2009) [MEDLINE]
Sensitivity: 85%
Specificity: 44%
Duration of Illness
Duration of Illness (Normal Host): 3-10 days (Prim Care, 1996) [MEDLINE] (Lancet, 2003) [MEDLINE]
Duration of Illness May Be as Long as 2-3 wks in Up to 25% of Patients (Particularly Smokers) (Ann Allergy Asthma Immunol, 1997) [MEDLINE] (Lancet Infect Dis, 2005) [MEDLINE]
Nasal Congestion is Common (and Occurs Later in Course) (Arch Intern Med, 1958) [MEDLINE] (Lancet Infect Dis, 2005) [MEDLINE]
Nasal Congestion/Obstruction Increases in Severity Over the First Week of Symptoms (Arch Intern Med, 1958) [MEDLINE]
Physiology
Due to Dilation of the Large Veins in the Nasal Epithelium (Venous Sinuses) in Response to the Vasodilator Mediators of Inflammation (Bradykinin, etc) (Lancet Infect Dis, 2005) [MEDLINE]
Rhinorrhea/Nasal Discharge is Common (Occurs Later in Course) (Arch Intern Med, 1958) [MEDLINE] (Lancet Infect Dis, 2005) [MEDLINE]
Clinical
Nasal Discharge May Be Clear or Purulent
Although Clinicians Commonly Use the Presence of Purulence to Determine if Antibiotics are Required (for a Sinus Infection), its Presence Alone Does Not Distinguish Between the Common Cold and a Sinus Infection (Lancet, 1997) [MEDLINE]
In a Sinus CT Study of Rhinovirus-Associated Common Cold, Sinus Abnormalities were Common (87% of Cases Demonstrated Abnormalities of One or Both Maxillary Sinus Cavities, 65% of Cases Demonstrated Abnormalities of the Ethmoid Sinuses, 32% of Cases Demonstrated Abnormalities of the Frontal Sinuses) (NEJM, 1944) [MEDLINE]
However, Since Asymptomatic Patients May Demonstrate Radiographic Abnormalities on Sinus X-Rays/CT, These Studies are Not Routinely Recommended in the Evaluation of the Common Cold (Arch Otolaryngol Head Neck Surg, 1988) [MEDLINE] (Laryngoscope, 1991) [MEDLINE]
Clinical
True Symptomatic Sinusitis is Uncommon (Although Sinus Mucosal Thickening Can Often Be Demonstrated on Sinus CT Scan)
In Contrast to the Common Cold, Acute Rhinosinusitis Presents with Facial Pain and Purulent Nasal Discharge (see Acute Rhinosinusitis)
Sneezing is Common (Occurs Early in Course) (Arch Intern Med, 1958) [MEDLINE] (Lancet Infect Dis, 2005) [MEDLINE]
Physiology
Sneezing is Mediated by the Trigeminal Nerve (Which Supplies the Nasal Epithelium and the Anterior Region of the Nasopharynx with Sensory Fibers) (Lancet Infect Dis, 2005) [MEDLINE]
Cough is Generally Less Common in the Common Cold, as Compared to Influenza
Physiology
Common Cold Viruses Usually Do Not Cause Any Significant Damage to the Airway Epithelium, Such that the Common Cold Often Occurs with Little, if Any, Cough (Acta Otolaryngol Suppl, 1984) [MEDLINE]
Symptoms of the Common Cold are Largely Due to the Immunologic Response to Infection
In Contrast, Influenza May Cause Significant Respiratory Epithelial Damage, Such that Influenza Infection is Usually Associated with Cough (Lancet Infect Dis, 2005) [MEDLINE]
Regarding the General Mechanism of Cough, it is Mediated Via the Vagus Nerve (Cough is Initiated by Airway by Stimulation of Sensory Nerves at the Level of the Larynx or Below) (Lancet Infect Dis, 2005) [MEDLINE]
Clinical
In Studies of Experimental Inoculation with Infectious Secretions from Patents with Presumed Common Colds, Cough Occurred Later in Course After the Onset of Nasal Obstruction/Discharge (Arch Intern Med, 1958) [MEDLINE]
Normal Lung Exam (Unless Bronchospasm is Present)
Cough is Less Prominent in Common Cold than in Influenza (for the Above Reason Related to Lack of Damage to the Airway Epithelium)
When Present, Cough May Persist for Weeks After the Resolution of Other Clinical Symptoms (Such as Nasal Obstruction and Sore Throat) (Ann Fam Med, 2013) [MEDLINE]
Viral Upper Respiratory Tract Infection Frequently Causes iEustachian Tube Dysfunction with Resulting Impaired Clearance and Pressure Dysregulation in the Middle Ear, Which May Predispose to the Development of Acute Otitis Media (Particularly in Children) (Lancet, 2004) [MEDLINE]
Viral Upper Respiratory Tract Infection Has Been Associated with Up to 40% of Acute Asthma Exacerbations in Adults (Chest, 1997) [MEDLINE] (J Infect Dis, 2007) [MEDLINE]
Rhinovirus is the Common Cold Virus Most Associated with Asthma Exacerbation
In Addition, Rhinovirus-Induced Changes in Airway Reactivity May Persist for Up to 4 wks After Infection (Am J Respir Crit Care Med, 1995) [MEDLINE]
Lower Respiratory Tract Disease
Most Patients with the Common Cold Do Not Have Lower Respiratory Tract Symptoms
However, Some Etiologies of the Common Cold Can (Influenza Virus, Respiratory Syncytial Virus, Parainfluenza Virus) Also Produce Lower Respiratory Tract Findings (Such as Acute Tracheobronchitis, Bronchiolitis, and Pneumonia)
For Example, Respiratory Syncytial Virus Can Cause Both Upper Respiratory Tract Disease (Such as the Common Cold) and Lower Respiratory Tract Disease in Children/Older Adults/Immunocompromised Patients (see Respiratory Syncytial Virus)
Prevention
Hand Hygiene
Clinical Efficacy
Hand Hygiene Decreases the Spread of Respiratory Viruses (Especially Among Children) (Cochrane Database Syst Rev, 2010) [MEDLINE]
Face Mask
Clinical Efficacy of Masks for Protection Against Transmission of Viruses
All Types of Face Masks Decrease Exposure to Viral Respiratory Pathogens (PLoS One, 2008) [MEDLINE]
This was Unaffected by the Duration of Wear or Type of Activity, But There was a High Degree of Individual Variation
Cotton Masks, Surgical Masks, and N95 Masks Provide Some Protection Against the Transmission of SARS-CoV-2 Droplets/Aerosols (mSphere. 2020) [MEDLINE]
Face Masks Decrease Respiratory Particle Emissions by Up to 90% (Sci Rep, 2020) [MEDLINE]
In a Study of an Outbreak of SARS-CoV-2 on the USS Theodore Roosevelt, Wearing Faec Masks Decreased Infections by Up to 70% (MMWR, 2020) [MEDLINE]
Face Masks Decrease Cases of Influenza, Respiratory Syncytial Virus, and Other Viral Respiratory Infections (BMJ, 2020) [MEDLINE] (Int J Infect Dis, 2021) [MEDLINE]
Face Masks Decrease SARS-CoV-2 Transmission ((JAMA, 2021) [MEDLINE]
Probiotics
Clinical Efficacy
In a Meta-Analysis, Probiotics (Lactobacillus, Bifidobacterium) were Better than Placebo in Terms of Decreasing the Number of Participants Experiencing Episodes of Acute Upper Respiratory Tract Infection, the Mean Duration of an episode of Acute Upper Respiratory Tract Infection, Antibiotic Use, and Common Cold-Related School Absence (Cochrane Database Syst Rev. 2015) [MEDLINE]
Evidence Quality was Low/Very Low
Exercise
Clinical Efficacy
One Year of Moderate-Intensity Exercise Training Decreased the Incidence of the Common Cold in Postmenopausal Women (Am J Med, 2006) [MEDLINE]
Randomized Trial Compared No Intervention with Exercise (45 min Daily at Home Plus 2.5 hrs Per Week of Group Sessions) or Mindfulness Meditation Had No Effect on the Incidence of Acute Respiratory Illness, Severity of Symptoms, or Missed Work Days (Ann Fam Med, 2012) [MEDLINE]
However, There was a Trend Toward Meditation Being Associated with Decreased Self-Reported Global Symptom Severity and Fewer Missed Work Days
In a Systematic Review/Meta-Analysis, There was an Unclear Effect of Exercise on Prevention of the Common Cold (Cochrane Database Syst Rev, 2015) [MEDLINE]
Sleep
Clinical Efficacy
In Patients Experimentally Inoculated with Rhinovirus, Patients Who Slept <5 Hours Per Night at Baseline were Almost 3-Fold More Likely to Develop a Common Cold than Patients Who Slept >7 Hours Per Night (Cochrane Database Syst Rev, 2013) [MEDLINE]
In Children, Zinc Sulfate (Taken for a Minimum of 5 Months) Decreased the Incidence of the Common Cold and School Absence (Cochrane Database Syst Rev, 2013) [MEDLINE]
Importantly, Intranasal Zinc May Cause Anosmia and Any Potential Benefit to its Use May Be Outweighed by This Risk (see Anosmia)
Serum 25(OH)D Levels were Found to Be Inversely Correlated with Recent Upper Respiratory Tract Infections (Arch Intern Med, 2009) [MEDLINE]
In a Randomized Trial, Monthly Administration of 100,000 IU of Vitamin D Did Not Decrease the Incidence/Severity of Upper Respiratory Tract Infections in Health Adults (JAMA. 2012) [MEDLINE]
In a Randomized Trial, Supplementation with 1000 IU/Day Vitamin D(3) Did Not Significantly Decrease the Incidence/Duration of Upper Respiratory Tract Infections in Adults with a Baseline Serum 25-Hydroxyvitamin D Level ≥12 ng/mL (Clin Infect Dis, 2013) [MEDLINE]
In a Post-Hoc Analysis, Vitamin E (200 IU/Day) Modestly Decreased the Incidence of the Common Cold (0.67 vs 0.81 per Person Pear Year, Relative Risk 0.83 with 95% CI: 0.68-1.01) (JAMA, 2004) [MEDLINE]
High-Dose (≥400 IU/Day) Vitamin E Supplementation Increased the All-Cause Mortality Rate (Ann Intern Med, 2005) [MEDLINE]
Echinacea is Not Efficacious in the Prevention of Community-Acquired Upper Respiratory Tract Infection (Arch Fam Med, 1998) [MEDLINE] (Am J Med, 1999) [MEDLINE]
In a Systematic Review, Echinacea Had a Positive (But Not Significant) Trend (Absolute Risk Reduction of 10%) Toward Decreasing the Incidence of the Common Cold (Cochrane Database Syst Rev. 2014) [MEDLINE]
Aspirin 500 mg and 1000 mg and Acetaminophen 500 mg and 1000 mg were Effective Against Fever and Other Symptoms of Upper Respiratory Tract Infection, as Compared to Placebo (Clin Ther, 2005) [MEDLINE]
NSAID’s are Somewhat Effective in Relieving Discomfort Caused by the Common Cold , But There is No Clear Evicence that They Decrease Respiratory Symptoms (Cochrane Database Syst Rev, 2015) [MEDLINE]
Ibuprofen Might Provide Short-Term Control of Symptoms in Patients with Chest infections (BMJ, 2013) [MEDLINE]
Aspirin 500 mg and 1000 mg and Acetaminophen 500 mg and 1000 mg were Effective Against Fever and Other Symptoms of Upper Respiratory Tract Infection, as Compared to Placebo (Clin Ther, 2005) [MEDLINE]
NSAID’s are Somewhat Effective in Relieving Discomfort Caused by the Common Cold , But There is No Clear Evicence that They Decrease Respiratory Symptoms (Cochrane Database Syst Rev, 2015) [MEDLINE]
Antihistamine/Decongestant Combinations
Clinical Efficacy
Antihistamine/Analgesic/Decongestant Combinations Had Some General Benefit in Adults and Older Children in Treatment of the Common Cold (Cochrane Database Syst Rev, 2012) [MEDLINE]
Benefits Must Be Weighed Against the Risk of Adverse Effects (Drowsiness, Dry Mouth, Insomnia, Dizziness)
There was No Evidence of Effectiveness Demonstrated in Young Children
Sodium Cromoglycate Administered Both by Inhalation and Intranasally was an Effective Treatment for the Symptoms of Upper Respiratory Tract Infections (Clin Exp Allergy, 1996) [MEDLINE]
Intranasal ipratropium Bromide was Likely Effective in Decreasing Rhinorrhea in Treatment of the Common Cold (Cochrane Database Syst Rev, 2013) [MEDLINE]
There was 2-Fold Increased Risk of Adverse Effects (Nasal Dryness, Blood-Tinged Mucous, Epistaxis) with Ipratropium Use
Treatments with Minimal/Uncertain Efficacy
Dextromethorphan
Clinical Efficacy
Dextromethorphan Likely Has a Small Benefit (12-36% Decrease in Cough Events) When Used in the Treatment of the Common Cold (Clin Exp Allergy, 1996) [MEDLINE] (Cochrane Database Syst Rev, 2013) [MEDLINE]
The Sale of Pseudoephedrine is Restricted in the US, as it Can Be Used to Manufacture Amphetamines [LINK]
Clinical Efficacy
A Single Oral Dose of Nasal Decongestant in the Common Cold is Modestly Effective (6% Decrease in Symptoms) for the Short-Term Relief of Nasal Congestion in Adults and These Drugs Also Provide Benefit (4% Decrease in Symptoms) in Some Patients After Regular Use Over 3-5 Days (Cochrane Database Syst Rev, 2007) [MEDLINE]
Insufficient Evidence that Oral Phenylephrine is Effective for Nonprescription Use as a Nasal Decongestant (Ann Pharmacother, 2007) [MEDLINE]
During a 6 hr Observation Period After Grass Pollen Challenge, a Single Dose of Pseudoephedrine (Oral, 60 mg), But Not Phenylephrine (Oral, 12 mg), Resulted in a Significant Improvement in Nasal Congestion (Ann Allergy Asthma Immunol, 2009) [MEDLINE]
Neither Phenylephrine Nor Pseudoephedrine Had an Effect on Non-Nasal Symptoms
Antihistamine/Analgesic/Decongestant Combinations Had Some General Benefit in Adults and Older Children in Treatment of the Common Cold (Cochrane Database Syst Rev, 2012) [MEDLINE]
Benefits Must Be Weighed Against the Risk of Adverse Effects (Drowsiness, Dry Mouth, Insomnia, Dizziness)
There was No Evidence of Effectiveness Demonstrated in Young Children
Recommendations/Precautions
Topical Decongestant (Afrin, etc) Use Should Be Limited to 2-3 Days, as Rebound Rhinitis Can Occur with Longer Duration of Use (see Oxymetazoline)
Topical Decongestant May Occasionally Be Complicated by Epistaxis, Agitation, Insomnia, and Worsened Hypertension in Patients with Preexisting Hypertension
Saline Nasal Spray
Clinical Efficacy
In a Systematic Review, Nasal Saline Irrigation Possibly Had Clinical Benefit for the Relief of Upper Respiratory Tract Symptoms (Cochrane Database Syst Rev, 2015) [MEDLINE]
However, the Included trials were Small and Had a High Risk of Bias
In a Randomized Trial, Guaifenesin Had a Marginal Effect,as Compared to Placebo, on Cough (Ann Allergy Asthma Immunol, 1997) [MEDLINE]
In a Systematic Review, Evaluation of Overall Efficacy of the Effect of Over-the-Counter Medications (Guaifenesin, Mucolytics, and Combination Medications) for Acute Cough in Children/Adults was Difficult (Cochrane Database Syst Rev, 2014) [MEDLINE]
Herbal Products
Clinical Efficacy
Elderberry Extract May Be Useful in the Treatment of Influenza A/B Infection (J Int Med Res, 2004) [MEDLINE]
Findings Need to Be Confirmed in Larger Studies
Pelargonium Sidoides Decreased the Severity of Symptoms and Shortened the Duration of the Common Cold, as Compared to Placebo (Explore-NY, 2007) [MEDLINE]
Pelargonium Sidoides (EPs 7630) was a Well-Tolerated and Effective Treatment for Acute Bronchitis in Adults (Outside the Very Restricted Indication for an Antibiotic Therapy) (Curr Med Res Opin, 2007) [MEDLINE]
In a Systematic Review, Sambuci Fructus (from European Elder) May Be Useful in the Treatment of Influenza Infection (Phytother Res, 2010)[MEDLINE]
Intranasal Zinc (Zicam) Use (Due to Risk of Permanent Anosmia) (see Anosmia) [US FDA Advisory]
Homeopathic Preparation of Intranasal Zinc Gluconate Has Been Associated with Hyposmia/Anosmia (Arch Otolaryngol Head Neck Surg, 2010) [MEDLINE]
Clinical Efficacy
Zinc Sulfate Syrups/Lozenges are Better Tolerated than Zinc Tablets (Cochrane Database Syst Rev, 2011) [MEDLINE]
In a Systematic Review, Oral Zinc Lozenges (at High Daily Dose >75 mg) Decreased the Duration of Common Cold Symptoms (Open Respir Med J, 2011) [MEDLINE]
In a Systematic Review/Meta-Analysis, Oral Zinc Decreased the Duration of Common Cold Symptoms (CMAJ, 2012) [MEDLINE]
Adverse Effects (Bad Taste, Nausea) were Common
Zinc (Dose of ≥75 mg/Day) Taken within 24 hrs of Symptom Onset Decreased the Duration of Common Cold Symptoms (Cochrane Database Syst Rev, 2013) [MEDLINE]
Treatments with No Efficacy
Antibiotics
Clinical Efficacy
In a Systematic Review in Children/Adults with Upper Respiratory Symptoms for <7 Days, Antibiotics Did Not Impact the Duration of Symptoms (Cochrane Database Syst Rev, 2013) [MEDLINE]
However, Adults Who Received Antibiotics Had a Significantly Higher Risk of Adverse Effects (Risk Ratio 2.62; CI: 1.32-5.18)
Use of Antibiotics in the Treatment of the Common Cold are Not of Clinical Benefit (Ann Intern Med, 2016) [MEDLINE]
Clinical Data-Inappropriate Antibiotic Use
In a Low-Risk Elderly Cohort (n = 180,000, Age ≥66 y/o), 46% of Patients with a Nonbacterial Acute Upper Respiratory Infection (Predominantly Common Colds) were Inappropriately Prescribed Antibiotics (Ann Intern Med, 2017) [MEDLINE]
Patients were More Likely to Receive Antibiotic Prescriptions from Mid or Late-Career Physicians with High Patient vVolumes and from Physicians Who were Trained Outside of Canada or the United States
First-Generation Antihistamines May Decrease Symptoms of Rhinorrhea and Sneezing in the Common Cold, But Their Use is Limited by Adverse Side Effects (Sedation, Dry Eyes, Dry Nose, Dry Mouth) (Ann Allergy Asthma Immunol. 1997) [MEDLINE]
In a Systematic Review of Patients with the Common Cold, Antihistamines Had a Limited (on Days 1-2 of Treatment) Beneficial Effect on Overall Symptom Severity, But No Effect in the Mid to Long-Term (Cochrane Database Syst Rev, 2015) [MEDLINE]
There was No Clinical Efficacy on Nasal Obstruction, Rhinorrhea, or Sneezing
Side Effects were More Common with Sedating Antihistamines
There was No Evidence of Clinical Efficacy of Antihistamine Use in Children
Antivirals
Clinical Efficacy
In a Trial of Combined NSAID’s (Ibuprofen), Antihistamines (Chlorpheniramine), and Antiviral Agent (Intranasal Interferon-α2b, Which is Active Against Rhinovirus) in the Treatment of Experimentally-Induced Common Cold, Patients Receiving the Interferon-α2b Regimen Had a 33-73% Decrease in Symptoms, Decreased Nasal Mucous Volume, and Decreased Virus Concentration in Nasal Mucous (J Infect Dis. 2002) [MEDLINE]
This Data is Applicable Only to Rhinovirus-Associated Common Colds
In a Meta-Analysis (29 Trials), Routine/Regular Supplementation with Vitamin C (at Least 200 mg/Day) Resulted in a Modest 8% Decrease in the Duration of Common Cold Symptoms (Cochrane Database Syst Rev, 2013) [MEDLINE]
Vitamin C Given Therapeutically After Common Cold Symptom Onset Did Not Decrease Symptom Duration or Severity
Codeine Has No Clinical Benefit in Treatment of the Common Cold (Cochrane Database Syst Rev, 2014) [MEDLINE]
Intranasal Glucocorticoids
Clinical Efficacy
Intranasal Glucocorticoids Have No Clinical Benefit in Treatment of the Common Cold (Cochrane Database Syst Rev, 2015) [MEDLINE]
Heated, Humidified Air
Clinical Efficacy
Heated, Humidified Air Has No Clinical Benefit in the Treatment of the Common Cold (BMJ, 2013) [MEDLINE] (Cochrane Database Syst Rev, 2017) [MEDLINE]
Incidence of Mild Thermal Injury is Low (Around 2%)
References
General
Transmission of the common cold to volunteers under controlled conditions. 1 The common cold as a clinical entity. Arch Intern Med, 1958; 101: 267–78 [MEDLINE]
Transmission of the common cold to volunteers under controlled conditions. IV. Specific immunity to the common cold. J Clin Invest. 1959 May;38(5):762-9 [MEDLINE]
Computed tomographic study of the common cold. N Engl J Med. 1994 Jan 6;330(1):25-30. doi: 10.1056/NEJM199401063300105 [MEDLINE]
The common cold. Prim Care. 1996;23(4):657 [MEDLINE]
Epidemiology, pathogenesis, and treatment of the common cold. Ann Allergy Asthma Immunol. 1997;78(6):531 [MEDLINE]
The common cold. Lancet. 2003;361(9351):51 [MEDLINE]
Effects of acetylsalicylic acid on sore throat pain and other pain symptoms associated with acute upper respiratory tract infection. Pain Med. 2003 Jun;4(2):118-24. doi: 10.1046/j.1526-4637.2003.03019.x [MEDLINE]
Epidemiology/Risk Factors
Psychological stress and susceptibility to the common cold. N Engl J Med. 1991 Aug;325(9):606-12 [MEDLINE]
Exercise, upper respiratory tract infection, and the immune system. Med Sci Sports Exerc. 1994 Feb;26(2):128-39 [MEDLINE]
Studies of the community and family: acute respiratory illness and infection. Epidemiol Rev. 1994;16(2):351-73 [MEDLINE]
Epidemiology, pathogenesis, and treatment of the common cold. Ann Allergy Asthma Immunol. 1997;78(6):531 [MEDLINE]
The economic burden of non-influenza-related viral respiratory tract infection in the United States. Arch Intern Med. 2003;163(4):487 [MEDLINE]
Sleep habits and susceptibility to the common cold. Arch Intern Med. 2009;169(1):62 [MEDLINE]
Etiology
Human bocaviruses and paediatric infections. Lancet Child Adolesc Health. 2019 Jun;3(6):418-426. doi: 10.1016/S2352-4642(19)30057-4 [MEDLINE]
Physiology
Quantitative rhinovirus shedding patterns in volunteers. Am Rev Respir Dis. 1966;94(2):159 [MEDLINE]
Histopathologic examination and enumeration of polymorphonuclear leukocytes in the nasal mucosa during experimental rhinovirus colds. Acta Otolaryngol Suppl 1984; 413: 19–24 [MEDLINE]
Epidemiology, pathogenesis, and treatment of the common cold. Ann Allergy Asthma Immunol. 1997;78(6):531 [MEDLINE]
Aircraft cabin air recirculation and symptoms of the common cold. JAMA. 2002;288(4):483 [MEDLINE]
Effect of antibacterial home cleaning and handwashing products on infectious disease symptoms: a randomized, double-blind trial. Ann Intern Med. 2004;140(5):321 [MEDLINE]
Viral titers in nasal lining fluid compared to viral titers in nasal washes during experimental rhinovirus infection. J Clin Virol. 2004;30(4):326 [MEDLINE]
Virucidal hand treatments for prevention of rhinovirus infection. J Antimicrob Chemother. 2005;56(5):805 [MEDLINE]
Sequencing and analyses of all known human rhinovirus genomes reveal structure and evolution. Science. 2009;324(5923):55 [MEDLINE]
Influenza A Virus Infection Triggers Pyroptosis and Apoptosis of Respiratory Epithelial Cells through the Type I Interferon Signaling Pathway in a Mutually Exclusive Manner. J Virol. 2018 Jun 29;92(14):e00396-18 [MEDLINE]
Diagnosis
Prevalence of incidental abnormalities on computed tomographic scans of the paranasal sinuses. Arch Otolaryngol Head Neck Surg. 1988;114(8):856 [MEDLINE]
Paranasal sinus bony anatomic variations and mucosal abnormalities: CT analysis for endoscopic sinus surgery. Laryngoscope. 1991;101(1 Pt 1):56 [MEDLINE]
Procalcitonin-guided antibiotic use vs a standard approach for acute respiratory tract infections in primary care. Arch Intern Med. 2008;168(18):2000 [MEDLINE]
Clinical utility of PCR for common viruses in acute respiratory illness. Pediatrics. 2014;133(3):e538 [MEDLINE]
Procalcitonin Levels in Acute Respiratory Infection. Viral Immunol. 2016;29(2):128 [MEDLINE]
Effects of procalcitonin testing on antibiotic use and clinical outcomes in patients with upper respiratory tract infections. An individual patient data meta-analysis. Clin Chem Lab Med. 2017;56(1):170 [MEDLINE]
Syndromic Panel-Based Testing in Clinical Microbiology. Clin Microbiol Rev. 2017 Nov 15;31(1):e00024-17. doi: 10.1128/CMR.00024-17 [MEDLINE]
The role of the NxTAG® respiratory pathogen panel assay and other multiplex platforms in clinical practice. Expert Rev Mol Diagn. 2017 Jan;17(1):9-17. doi: 10.1080/14737159.2017.1266260 [MEDLINE]
Asymptomatic Shedding of Respiratory Virus among an Ambulatory Population across Seasons. mSphere. 2018;3(4) [MEDLINE]
Performance of a multiplex PCR pneumonia panel for the identification of respiratory pathogens and the main determinants of resistance from the lower respiratory tract specimens of adult patients in intensive care units. J Microbiol Immunol Infect. 2019 Dec;52(6):920-928. doi: 10.1016/j.jmii.2019.10.009 [MEDLINE]
Clinical
Transmission of the common cold to volunteers under controlled conditions. I. The common cold as a clinical entity. AMA Arch Intern Med. 1958;101(2):267 [MEDLINE]
Signs and symptoms in common colds. Epidemiol Infect 1993; 111: 143–56 [MEDLINE]
Virus-induced airway hyperresponsiveness. Role of inflammatory cells and mediators. Am J Respir Crit Care Med. 1995;151(5):1666 [MEDLINE] The incidence of respiratory tract infection in adults requiring hospitalization for asthma. Chest. 1997;112(3):591 [MEDLINE]
Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5(11):718 [MEDLINE]
Relations among questionnaire and laboratory measures of rhinovirus infection. Eur Respir J. 2006;28(2):358 [MEDLINE]
Pan-viral screening of respiratory tract infections in adults with and without asthma reveals unexpected human coronavirus and human rhinovirus diversity. J Infect Dis. 2007;196(6):817 [MEDLINE]
Validation of a short form Wisconsin Upper Respiratory Symptom Survey (WURSS-21). Health Qual Life Outcomes. 2009;7:76 [MEDLINE]
How long does a cough last? Comparing patients’ expectations with data from a systematic review of the literature. Ann Fam Med. 2013;11(1):5 [MEDLINE]
Comparison of COVID-19 and common cold chemosensory dysfunction. Rhinology. 2020 Dec 1;58(6):623-625. doi: 10.4193/Rhin20.251 [MEDLINE]
Prevention
Echinacea root extracts for the prevention of upper respiratory tract infections: a double-blind, placebo-controlled randomized trial. Arch Fam Med. 1998;7(6):541 [MEDLINE]
A randomized controlled trial of the effect of fluid extract of Echinacea purpurea on the incidence and severity of colds and respiratory infections. Am J Med. 1999;106(2):13 [MEDLINE]
Vitamin E and respiratory tract infections in elderly nursing home residents: a randomized controlled trial. JAMA. 2004;292(7):828 [MEDLINE]
Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med. 2005;142(1):37 [MEDLINE]
Prevention of upper respiratory tract infections by gargling: a randomized trial. Am J Prev Med. 2005;29(4):302 [MEDLINE]
Montelukast reduces asthma exacerbations in 2- to 5-year-old children with intermittent asthma. Am J Respir Crit Care Med. 2005;171(4):315 [MEDLINE]
Moderate-intensity exercise reduces the incidence of colds among postmenopausal women. Am J Med. 2006;119(11):937 [MEDLINE]
Clinical evaluation of leukotriene receptor antagonists in preventing common cold-like symptoms in bronchial asthma patients. Allergol Int. 2007;56(3):263 [MEDLINE]
Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch Intern Med. 2009;169(4):384 [MEDLINE]
Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev. 2010 Jan 20;(1):CD006207. doi: 10.1002/14651858.CD006207.pub3 [MEDLINE]
North American (Panax quinquefolius) and Asian Ginseng (Panax ginseng) Preparations for Prevention of the Common Cold in Healthy Adults: A Systematic Review. Evid Based Complement Alternat Med. 2011;2011:282151 [MEDLINE]
Effect of vitamin D3 supplementation on upper respiratory tract infections in healthy adults: the VIDARIS randomized controlled trial. JAMA. 2012;308(13):1333 [MEDLINE]
Meditation or exercise for preventing acute respiratory infection: a randomized controlled trial. Ann Fam Med. 2012 Jul;10(4):337-46 [MEDLINE]
Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev. 2013 Jan 31;2013(1):CD000980. doi: 10.1002/14651858.CD000980.pub4 [MEDLINE]
Zinc for the common cold. Cochrane Database Syst Rev. 2013 Jun 18;(6):CD001364. doi: 10.1002/14651858.CD001364.pub4 [MEDLINE]
Vitamin D3 supplementation and upper respiratory tract infections in a randomized, controlled trial. Clin Infect Dis. 2013;57(10):1384 [MEDLINE]
Garlic for the common cold. Cochrane Database Syst Rev. 2014 Nov 11;2014(11):CD006206. doi: 10.1002/14651858.CD006206.pub4. [MEDLINE]
Echinacea for preventing and treating the common cold. Cochrane Database Syst Rev. 2014 Feb 20;2(2):CD000530. doi: 10.1002/14651858.CD000530.pub3. [MEDLINE]
Exercise versus no exercise for the occurrence, severity and duration of acute respiratory infections. Cochrane Database Syst Rev. 2015 Jun 16;(6):CD010596. doi: 10.1002/14651858.CD010596.pub2 [MEDLINE]
Probiotics for preventing acute upper respiratory tract infections. Cochrane Database Syst Rev. 2015 Feb 3;(2):CD006895. doi: 10.1002/14651858.CD006895.pub3 [MEDLINE]
Treatment
Effects of antibiotic treatment in the subset of common-cold patients who have bacteria in nasopharyngeal secretions. Lancet. 1996;347(9014):1507 [MEDLINE]
The effect of inhaled and intranasal sodium cromoglycate on symptoms of upper respiratory tract infections. Clin Exp Allergy. 1996;26(9):1045 [MEDLINE]
Colour of respiratory discharge and antibiotic use. Lancet. 1997;350(9084):1077 [MEDLINE]
Epidemiology, pathogenesis, and treatment of the common cold. Ann Allergy Asthma Immunol. 1997;78(6):531 [MEDLINE]
Combined antiviral-antimediator treatment for the common cold. J Infect Dis. 2002;186(2):147 [MEDLINE]
Randomized study of the efficacy and safety of oral elderberry extract in the treatment of influenza A and B virus infections. J Int Med Res. 2004;32(2):132 [MEDLINE]
Aspirin compared with acetaminophen in the treatment of fever and other symptoms of upper respiratory tract infection in adults: a multicenter, randomized, double-blind, double-dummy, placebo-controlled, parallel-group, single-dose, 6-hour dose-ranging study. Clin Ther. 2005 Jul;27(7):993-1003 [MEDLINE]
Topical glucocorticosteroids in rhinitis: clinical aspects. Acta Otolaryngol. 2006;126(10):1022 [MEDLINE]
Nasal decongestants for the common cold. Cochrane Database Syst Rev. 2007 Jan 24;(1):CD001953. doi: 10.1002/14651858.CD001953.pub3 [MEDLINE]
Efficacy and safety of oral phenylephrine: systematic review and meta-analysis. Ann Pharmacother. 2007;41(3):381 [MEDLINE]
Efficacy of a pelargonium sidoides preparation in patients with the common cold: a randomized, double blind, placebo-controlled clinical trial. Explore (NY). 2007;3(6):573 [MEDLINE]
Treatment of acute bronchitis with a liquid herbal drug preparation from Pelargonium sidoides (EPs 7630): a randomised, double-blind, placebo-controlled, multicentre study. Curr Med Res Opin. 2007;23(2):323 [MEDLINE]
Antibiotic prescribing for self limiting respiratory tract infections in primary care: summary of NICE guidance. BMJ. 2008;337:a437 [MEDLINE]
A placebo-controlled study of the nasal decongestant effect of phenylephrine and pseudoephedrine in the Vienna Challenge Chamber. Ann Allergy Asthma Immunol. 2009;102(2):116 [MEDLINE]
The Bradford Hill criteria and zinc-induced anosmia: a causality analysis. Arch Otolaryngol Head Neck Surg. 2010;136(7):673 [MEDLINE]
A systematic review on the sambuci fructus effect and efficacy profiles. Phytother Res. 2010;24(1):1 [MEDLINE]
Zinc for the common cold. Cochrane Database Syst Rev. 2011 Feb 16;(2):CD001364. doi: 10.1002/14651858.CD001364.pub3 [MEDLINE]
Zinc lozenges may shorten the duration of colds: a systematic review. Open Respir Med J. 2011;5:51-8 [MEDLINE]
Zinc for the treatment of the common cold: a systematic review and meta-analysis of randomized controlled trials. CMAJ. 2012;184(10):E551 [MEDLINE]
Oral antihistamine-decongestant-analgesic combinations for the common cold. Cochrane Database Syst Rev. 2012 Feb 15;(2):CD004976. doi: 10.1002/14651858.CD004976.pub3 [MEDLINE]
Antibiotics for the common cold and acute purulent rhinitis. Cochrane Database Syst Rev. 2013 Jun 4;2013(6):CD000247. doi: 10.1002/14651858.CD000247.pub3 [MEDLINE]
Intranasal ipratropium bromide for the common cold. Cochrane Database Syst Rev. 2013 Jun 19;2013(6):CD008231. doi: 10.1002/14651858.CD008231.pub3. [MEDLINE]
Ibuprofen, paracetamol, and steam for patients with respiratory tract infections in primary care: pragmatic randomised factorial trial. BMJ. 2013;347:f6041 [MEDLINE]
Over-the-counter (OTC) medications for acute cough in children and adults in community settings. Cochrane Database Syst Rev. 2014 Nov 24;2014(11):CD001831. doi: 10.1002/14651858.CD001831.pub5 [MEDLINE]
Echinacea for preventing and treating the common cold. Cochrane Database Syst Rev. 2014 Feb 20;2(2):CD000530. doi: 10.1002/14651858.CD000530.pub3. [MEDLINE]
Antihistamines for the common cold. Cochrane Database Syst Rev. 2015 Nov 29;(11):CD009345. doi: 10.1002/14651858.CD009345.pub2 [MEDLINE]
Corticosteroids for the common cold. Cochrane Database Syst Rev. 2015 Oct 13;(10):CD008116. doi: 10.1002/14651858.CD008116.pub3. [MEDLINE]
Appropriate Antibiotic Use for Acute Respiratory Tract Infection in Adults: Advice for High-Value Care From the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2016;164(6):425 [MEDLINE]
Antibiotic Prescribing for Nonbacterial Acute Upper Respiratory Infections in Elderly Persons. Ann Intern Med. 2017;166(11):765 [MEDLINE]
Heated, humidified air for the common cold. Cochrane Database Syst Rev. 2017 Aug 29;8(8):CD001728. doi: 10.1002/14651858.CD001728.pub6 [MEDLINE]