Acute Pharyngitis is One of the Most Common Conditions Encountered in Outpatient Clinical Practice
Most Cases of Acute Pharyngitis are Caused by Respiratory Viruses and are Self-Limited
However, Acute Pharyngitis May Also Be Caused by Treatable Bacterial Infections (Such as Streptococcus Pyogenes)
Acute Pharyngitis Accounts for Approximately 12 Million Ambulatory Care Visits (or 1-2% of All Ambulatory Visits) Annually in the United States (Scand J Infect Dis, 2002) [MEDLINE]
Incidence of Acute Pharyngitis Peaks in Childhood/Adolescence (50% of Cases Occur Before Age 18) (Scand J Infect Dis, 2002) [MEDLINE] (Pediatrics, 2007) [MEDLINE]
In Adults, Most Cases of Acute Pharyngitis Occure Prior to Age 40 and the Incidence Decreases After Age 40
Etiology
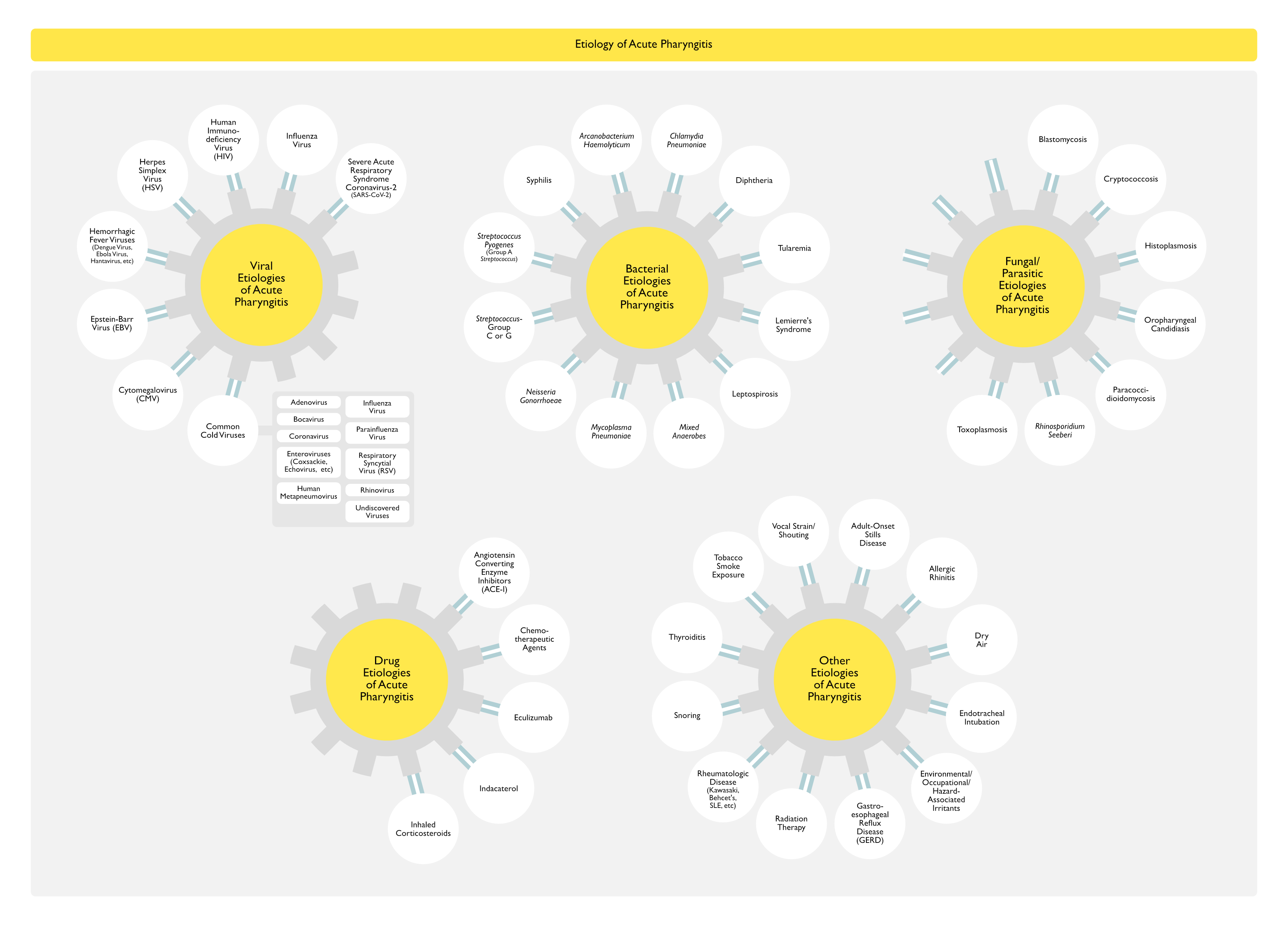
Infection
Viral
General Comments
Respiratory Viruses are the Most Common Etiology of Acute Pharyngitis (Account for 25-45% of Pharyngitis Cases) (Ann Intern Med, 1989) [MEDLINE] (NEJM, 2001) [MEDLINE]
Patients with Pharyngitis Caused by Respiratory Viruses Usually Have Other Symptoms/Signs of Upper Respiratory Tract Infection (Such as Fatigue, Nasal Congestion, Cough, Coryza, Conjunctivitis, Sneezing, Hoarseness, Ear Pain, Sinus Discomfort, Oral Ulcers, and/or a Viral Exanthem)
Pharyngitis Occurs Most Commonly as Part of the Common Cold Syndrome and is, Therefore, is Usually Associated with the Same Viruses Which Cause the Common Cold
Severe Exudative Pharyngitis (with Cervical Lymphadenopathy and Less Frequent Fever/Oropharyngeal Ulcers) (see Lymphadenopathy): primary Herpes-Simplex virus infection may account for as many as 5% of adult pharyngitis cases (Pediatr Infect Dis J, 1993) [MEDLINE]
Pharyngitis May Occur in the Setting of Primary Human Immunodeficiency Virus Infection
Risk is Increased in Patients with Demographic Risk Factors (Age 15-24 y/o, Men Who Have Sex with Men, History of Sexually-Transmitted Disease, Unmarried Status, Lowe Socioeconomic Status, High School Education or Less, Admission to Correctional Facility, Illicit Drug Use) and Behavioral Risk Factors (New Sex Partner in Past 60 Days, Multiple or Anonymous Sex Partners, Inconsistent Condom Use in Non-Monogamous Relationship, Trading Sex for Money for Drugs, Sexual Contact with Sex Workers)
Acute Retroviral Syndrome (i.e Symptomatic Acute HIV Infection): acute HIV infection is symptomatic in 40-90% of cases, symptoms occur 2-4 wks after infection (Curr Opin HIV AIDS, 2008)[MEDLINE]
Francisella Tularensis (Tularemia-Pharyngeal/Oropharyngeal) (see Tularemia)
Epidemiology
Rare
Typically Associated with Ingestion of Contaminated Food or Water (Comp Immunol Microbiol Infect Dis, 2014) [MEDLINE] (MMWR Morb Mortal Wkly Rep, 2015) [MEDLINE]
Clinical
Ulceroglandular Fever
Painful Cervical Lymphadenopathy (Particularly Posterior and Bilateral) (see Lymphadenopathy)
Possible Association with Recurrent or Persistent Pharyngitis
Physiology
Fusobacterium Necrophorum is an Anaerobe Which May Colonizes the Oropharynx (in 2-10% of Normal Young Adults) and is Considered a Putative Cause of Pharyngitis
Rates of Oropharyngeal Detection is Higher (15-20% of Cases) of Adults with Acute Pharyngitis
Rates of Oropharyngeal Detection is Even Higher (45% of Cases) of Adults with Recurrent Pharyngitis
Co-Pathogens are Frequently Also Detected with Fusobacterium Necrophorum
However, Fusobacterium Necrophorum is Considered a True Pathogen in Lemierre’s Syndrome
Mucous Patches on the Oral Mucosa and Tongue (Round/Oval Elevated Lesion, Covered by a Pink-Gray Membrane)
Pharyngitis is Common (Occurs in 50% of Secondary Syphilis Cases): sore throat may precede the mucosal ulcers, generalized lymphadenopathy and palmar-plantar rash
Rash on Palms/Soles (Palmar-Plantar Rash)
Fungal
Blastomyces Dermatitidis (Blastomycosis) (see Blastomycosis)
Epidemiology
Rare Etiology of Acute Pharyngitis
Cryptococcus Neoformans (Crytptococcosis) (see Crytptococcosis)
Epidemiology
Rare Etiology of Acute Pharyngitis
Histoplasma Capsulatum (Histoplasmosis) (see Histoplasmosis)
Associated with Either Smoking or Second-Hand Smole Exposure
Vocal Strain/Shouting
Epidemiology
Sore Throat/Pharyngitis is Common with Vocal Strain (Due to Excessive Speaking, etc) (Codas, 2016) [MEDLINE] (J Voice, 2016) [MEDLINE]
Physiology
Pain of Pharyngitis
Mediated by Kinins (Which are Potent Stimulators of Nerve Endings)
Bradykinin is Present in Nasal Secretions in the Common Cold
Experimental Topical Application of Bradykinin Induces a Sore Throat and Nasal Symptoms
Lysylbradykinin is Present in Nasal Secretions in the Common Cold
Diagnosis
Oropharyngeal (Throat) Swab with Rapid Antigen Detection Test (RADT) for Streptococcus Pyogenes (see Streptococcus Pyogenes)
General Comments
For Most Adults with Suspected Streptococcus Pyogenes Pharyngitis, Testing with Rapid Antigen Detection Test is Sufficient to Establish the Diagnosis (Clin Infect Dis, 2012) [MEDLINE
In Patient with a Negative Rapid Antigen Detection Test for Streptococcus Pyogenes, Further Testing with Oropharyngeal Culture is Indicated for Specific Groups of Patients (See Below)
Recommendations (Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America) (Clin Infect Dis, 2012) [MEDLINE]
How Should the Diagnosis of Streptococcus Pyogenes Pharyngitis Be Established?
Oropharyngeal Swab Testing for Streptococcus Pyogenes Pharyngitis (Rapid Antigen Detection Test and/or Oropharyngeal Culture for Streptococcus Pyogenes) Should Be Performed Since Clinical Features Alone Do Not Reliably Discriminate Between Streptococcus Pyogenes Pharyngitis and Viral Pharyngitis (Except When Overt Viral Clinical Features Such as Rhinorrhea, Cough, Oral Ulcers, and/or Hoarseness are Present)
In Children/Adolescents, a Negative Rapid Antigen Detection Test for Streptococcus Pyogenes Should Be Followed by a Oropharyngeal Culture for Streptococcus Pyogenes (Strong Recommendation, High Quality of Evidence)
A Positive Rapid Antigen Detection Test for Streptococcus Pyogenes Does Not Necessitate a Back-Up Oropharyngeal Culture Because the Rapid Antigen Detection Test is Highly Specific (Strong Recommendation, High Quality of Evidence)
For Those with a Negative Rapid Antigen Detection Test for Streptococcus Pyogenes, Routine Use of Back-Up Oropharyngeal Culture for Streptococcus Pyogenes is Not Necessary for Adults (with the Exceptions Discussed Below), Because of the Low Incidence of Streptococcus Pyogenes Pharyngitis in Adults and Because the Risk of Subsequent Acute Rheumatic Fever is Generally Exceptionally Low in Adults with Acute Pharyngitis (Strong Recommendation, Moderate Quality of Evidence)
Physicians Who Wish to Ensure that They are Achieving Maximal Sensitivity in Diagnosis May Continue to Use Conventional Oropharyngeal Culture for Streptococcus Pyogenes or to Back-Up a Negative Rapid Antigen Detection Test for Streptococcus Pyogenes with a Subsequent Oropharyngeal Culture for Streptococcus Pyogenes
Anti-Streptococcal Antibody Titers are Not Recommended in the Routine Diagnosis of Acute Pharyngitis as They Reflect Past But Not Current Events (Strong Recommendation, High Quality of Evidence)
Who Should Undergo Testing for Streptococcus Pyogenes Pharyngitis?
Testing for Streptococcus Pyogenes Pharyngitis is Not Usually Recommended for Children/Adults with Acute Pharyngitis with Clinical and Epidemiological Features Which Strongly Suggest a Viral Etiology (Rhinorrhea, Cough, Oral Ulcers, and/or Hoarseness) (Strong Recommendation, High Quality of Evidence)
Diagnostic Studies for Streptococcus Pyogenes Pharyngitis are Not Indicated for Children <3 y/o Because Acute Rheumatic Fever is Rare in Children <3 y/o and the Incidence of Streptococcal Pharyngitis and the Classic Presentation of Streptococcal Pharyngitis are Uncommon in this Age Group
Selected Children <3 y/o Who Have Other Risk Factors (Such as an Older Sibling with Streptococcus Pyogenes Infection) May Be Considered for Testing (Strong Recommendation, Moderate Quality of Evidence)
Follow-Up Post-Treatment Oropharyngeal Cultures for Streptococcus Pyogenes or Rapid Antigen Detection Test for Streptococcus Pyogenes are Not Recommended Routinely But May Be Considered in Special Circumstances (Strong Recommendation, High Quality of Evidence)
Diagnostic Testing or Empiric Treatment of Asymptomatic Household Contacts of Patients with Acute Streptococcal Pharyngitis is Not Routinely Recommended (Strong Recommendation, Moderate Quality of Evidence)
For Most Adults with Suspected Streptococcus Pyogenes Pharyngitis, Testing with Rapid Antigen Detection Test (See Above) is Sufficient to Establish Diagnosis (Clin Infect Dis, 2012) [MEDLINE
However, the Following Patients with a Negative Rapid Antigen Detection Test for Streptococcus Pyogenes Should Undergo Further Testing to Definitively Exclude the Diagnosis of Streptococcus Pyogenes Pharyngitis
Patient at Hight Risk for Severe Infection or Complications from Streptococcus Pyogenes Pharyngitis
Immunocompromised State
Patient with History of Acute Rheumatic Fever
Patient in Close Contact with Individual at Hight Risk for Complications
Patient Caring for Infants or Living with Immunocompromised Individuals)
Young Adult Patient Living in College Dormitory or Other Setting Where the prevalence of Streptococcus Pyogenes Pharyngitis is Higher than that of the General Adult Population
Patient Living in Area where Acute Rheumatic Fever is Endemic or Where There is an Active Acute Rheumatic Fever Epidemics
Patient in Whom Clinical Suspicion for Streptococcus Pyogenes is High Despite a Negative Rapid Antigen Detection Test
Person with Centor Score ≥3 Who Have Additional Risk Factors for Streptococcus Pyogenes Pharyngitis (Such as Exposure to a Person with Streptococcus Pyogenes Infection)
Technique
Oropharyngeal Culture Samples Should Be Obtained Prior to Antibiotic Administration to maximize Diagnostic Yield (Pediatr Infect Dis J, 1987) [MEDLINE] (Pediatrics, 1993) [MEDLINE]
Specimen Collection Requires Vigorous Swabbing of Both Tonsils (or Tonsillar Fossa, in Those with Prior Tonsillectomy) and Posterior Pharynx
Specimens Collected from the Tongue, Buccal Mucosa, or Hard Palate are Not Adequate
Sensitivity of Oropharyngeal Culture Correlates with the Bacterial Inoculum Obtained by Swabbing
Streptococcus Pyogenes Remains Viable on Dry Swabs for Approximately 48-72 hrs After Collection
Therefore, a Second Swab Collected for Rapid Antigen Detection Test Can Be Later Sent for Culture After the Rapid Antigen Detection Test Has Resulted
Oropharyngeal Culture Generally Requires Around 24-48 hrs
Due to Short Processing Time Required, Empiric Treatment is Not Recommended (Since Short Delay in Initiating Antibiotic Therapy for Streptococcus Pyogenes Infection is Not Generally Associated with Increased Complication Rates)
Sensitivity/Specificity with Proper Collection/Processing (Clin Infect Dis, 2012) [MEDLINE]
Sensitivity: 90-95%
Specificity: 95-99%
Recommendations (Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America) (Clin Infect Dis, 2012) [MEDLINE]
How Should the Diagnosis of Streptococcus Pyogenes Pharyngitis Be Established?
Oropharyngeal Swab Testing for Streptococcus Pyogenes Pharyngitis (Rapid Antigen Detection Test and/or Oropharyngeal Culture for Streptococcus Pyogenes) Should Be Performed Since Clinical Features Alone Do Not Reliably Discriminate Between Streptococcus Pyogenes Pharyngitis and Viral Pharyngitis (Except When Overt Viral Clinical Features Such as Rhinorrhea, Cough, Oral Ulcers, and/or Hoarseness are Present)
In Children/Adolescents, a Negative Rapid Antigen Detection Test for Streptococcus Pyogenes Should Be Followed by a Oropharyngeal Culture for Streptococcus Pyogenes (Strong Recommendation, High Quality of Evidence)
A Positive Rapid Antigen Detection Test for Streptococcus Pyogenes Does Not Necessitate a Back-Up Oropharyngeal Culture Because the Rapid Antigen Detection Test is Highly Specific (Strong Recommendation, High Quality of Evidence)
For Those with a Negative Rapid Antigen Detection Test for Streptococcus Pyogenes, Routine Use of Back-Up Oropharyngeal Culture for Streptococcus Pyogenes is Not Necessary for Adults (with the Exceptions Discussed Below), Because of the Low Incidence of Streptococcus Pyogenes Pharyngitis in Adults and Because the Risk of Subsequent Acute Rheumatic Fever is Generally Exceptionally Low in Adults with Acute Pharyngitis (Strong Recommendation, Moderate Quality of Evidence)
Physicians Who Wish to Ensure that They are Achieving Maximal Sensitivity in Diagnosis May Continue to Use Conventional Oropharyngeal Culture for Streptococcus Pyogenes or to Back-Up a Negative Rapid Antigen Detection Test for Streptococcus Pyogenes with a Subsequent Oropharyngeal Culture for Streptococcus Pyogenes
Anti-Streptococcal Antibody Titers are Not Recommended in the Routine Diagnosis of Acute Pharyngitis as They Reflect Past But Not Current Events (Strong Recommendation, High Quality of Evidence)
Who Should Undergo Testing for Streptococcus Pyogenes Pharyngitis?
Testing for Streptococcus Pyogenes Pharyngitis is Not Usually Recommended for Children/Adults with Acute Pharyngitis with Clinical and Epidemiological Features Which Strongly Suggest a Viral Etiology (Rhinorrhea, Cough, Oral Ulcers, and/or Hoarseness) (Strong Recommendation, High Quality of Evidence)
Diagnostic Studies for Streptococcus Pyogenes Pharyngitis are Not Indicated for Children <3 y/o Because Acute Rheumatic Fever is Rare in Children <3 y/o and the Incidence of Streptococcal Pharyngitis and the Classic Presentation of Streptococcal Pharyngitis are Uncommon in this Age Group
Selected Children <3 y/o Who Have Other Risk Factors (Such as an Older Sibling with Streptococcus Pyogenes Infection) May Be Considered for Testing (Strong Recommendation, Moderate Quality of Evidence)
Follow-Up Post-Treatment Oropharyngeal Cultures for Streptococcus Pyogenes or Rapid Antigen Detection Test for Streptococcus Pyogenes are Not Recommended Routinely But May Be Considered in Special Circumstances (Strong Recommendation, High Quality of Evidence)
Diagnostic Testing or Empiric Treatment of Asymptomatic Household Contacts of Patients with Acute Streptococcal Pharyngitis is Not Routinely Recommended (Strong Recommendation, Moderate Quality of Evidence)
Polymerase Chair Reaction (PCR) Assay for Streptococcus Pyogenes
General Comments
PCR-Based Assays for Streptococcus Pyogenes are More Sensitive than Rapid Antigen Detection Tests for Streptococcus Pyogenes and Oropharyngeal Culture for Streptococcus Pyogenes (Particularly When the Bacterial Burden is Low (J Clin Microbiol, 2016) [MEDLINE]
However, PCR-Based Assays for Streptococcus Pyogenes are Not Routinely Available in Clinical Practice
Diagnostic Testing for Pathogens Other than Streptococcus Pyogenes
In Any Patient Presenting with an Acute Respiratory Illness, Oropharyngeal Swab with Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) Testing for SARS-CoV-2 is Required for the Purpose of Infection Control
Should Be Performed in Patient with Non-Streptococcus Pyogenes Pharyngitis Who Does Not Clinically Respond to Symptomatic Therapy within 5-7 Days (Clin Infect Dis, 2012) [MEDLINE]
Diagnostic Testing for Corynebacterium Diphtheriae (Diphtheria) (see Diphtheria)
Should Be Considered in Patient with Appropriate Clinical Risk Factors
Diagnostic Testing for Francisella Tularensis (Tularemia) (see Tularemia)
Should Be Considered in Patient with Appropriate Clinical Risk Factors
Diagnostic Testing for Human Immunodeficiency Virus (HIV) (see Human Immunodeficiency Virus) –Combination Antigen/Antibody Immunoassay (and HIV Viral Load Test) is the Preferred Mode of Testing
Pharyngeal Swab Testing for Nucleic Acid Amplification test (NAAT) for Neisseria Gonorrhoeae is the Preferred Diagnostic Test for gonococcal Pharyngitis
Screening for Sexually-Transmitted Infection (STI’s)
Standardized Screening for Sexually-Transmitted Infections (Neisseria Gonorrhoeae, Chlamydia Trachomatis, etc) is Determined by the Presence of Various Risk Factors (see Urethritis)
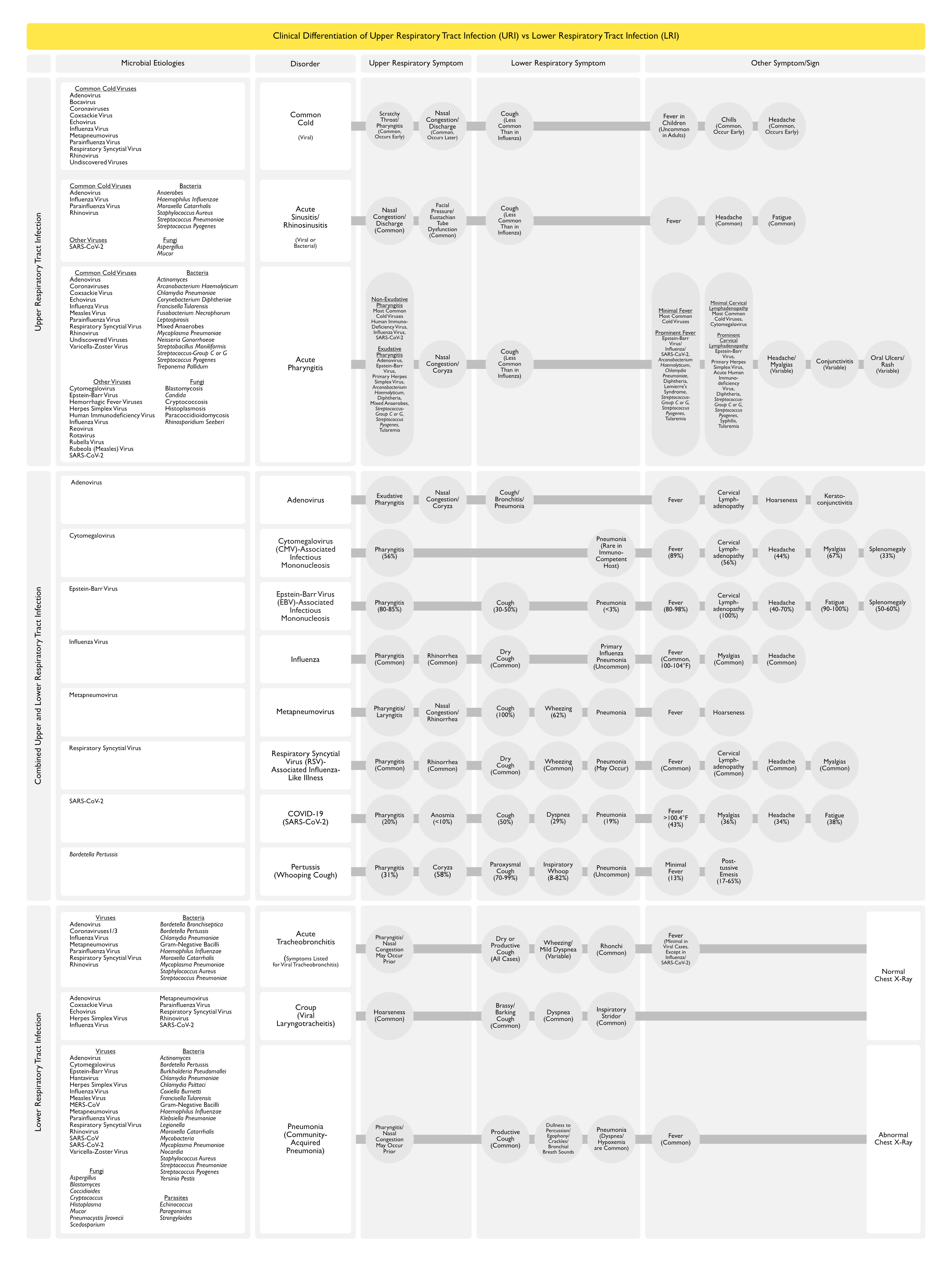
Clinical Differentiation of Upper Respiratory Tract Infection vs Lower Respiratory Tract Infection
Clinical Manifestations
Otolaryngologic Manifestations
Pharyngeal Exudates
Clinical Features of Viral Pharyngitis
Pharyngeal Exudates are Typically Absent in Pharyngitis Due to Rhinovirus, Coronavirus, Influenza Virus, and Respiratory Syncytial Virus
Pharyngeal Exudates May Occur in Adenovirus Pharyngitis (see Adenovirus)
Pharyngeal Exudates are Prominent (and Palatal Petechiae May Occur) in Epstein-Barr Virus Infectious Mononucleosis (see Epstein-Barr Virus)
Pharyngeal Exudates are Prominent in Primary Herpes Simplex Virus Infection in Adults (see Herpes Simplex Virus)
Clinical Features of Bacterial Pharyngitis
In General, Pharyngeal Exudates are More Prominent
Pharyngeal Exudates are Prominent in Arcanobacterium Haemolyticum Pharyngitis (see Arcanobacterium Haemolyticum)
Pharyngeal Pseudomomembrane is Prominent in Corynebacterium Diphtheriae Pharyngitis (see Diphtheria)
Pharyngeal Ulcers/Pseudomomembrane May Occur in Lemierre’s Syndrome (see Lemierre’s Syndrome)
Pharyngeal Exudates are Prominent in in Mixed Anaerobic Infection (Vincent’s Angina, Peritonsillar Abscess)
Pharyngeal Exudates are Prominent in Neisseria Gonorrhoeae Pharyngitis (see Neisseria Gonorrhoeae)
Trismus (Irritation and Reflex Spasm of the Internal Pterygoid Muscle) (see Trismus)
Treatment
Treatment of Acute Viral Pharyngitis
Supportive Care
Antibiotics are Contraindicated in Acute Viral Pharyngitis and Most Patients with Recover within 5-7 Days without Specific Therapy, (Ann Intern Med, 2001) [MEDLINE]
Failure to Clinically Improve
In Patients with Negative Rapid Antigen Detection Testing for Streptococcus Pyogenes and a Lack of Clinical Improvement within 5-7 Days, Other Potential Diagnoses Should Be Considered (Clin Infect Dis, 2012) [MEDLINE]
Treatment of Streptococcus Pyogenes (Group A Streptococcus) Pharyngitis
Antibiotic Therapy
Patients with Documented Streptococcus Pyogenes Pharyngitis Generally Recover within 24-74 hrs of Starting Antibiotics
Failure to Clinically Improve
In Patients with Positive Rapid Antigen Detection Testing for Streptococcus Pyogenes and a Lack of Clinical Improvement, Suppurative Complications (Peritonsillar Abscess, etc) or an Alternative Diagnosis Superimposed on Streptococcus Pyogenes Chronic Carriage Should Be Considered (Clin Infect Dis, 2012) [MEDLINE]
Recommendations (Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America) (Clin Infect Dis, 2012) [MEDLINE]
Patients with Acute Streptococcus Pyogenes Pharyngitis Should Be Treated with an Appropriate Antibiotic (at Appropriate Dose) Usually for 10 Days to Eradicate the Organism from the Oropharynx
In Patients Who are Not Penicillin-Allergic, Penicillin/Amoxicillin are the Recommended First-Line Antibiotics for the Treatment of Streptococcus Pyogenes Pharyngitis (Strong Recommendation, High Quality of Evidence)
This Recommendation is Based on the Narrow Spectrum of Activity, Infrequency of Adverse Reactions, and Modest Cost of Penicillins
In Patients Who are Penicillin-Allergic, Treatment of Streptococcus Pyogenes Pharyngitis Should Include One of the Following (Strong Recommendation, Moderate Quality of Evidence)
For Those Not Anaphylactically Penicillin-Sensitive, First-Generation Cephalosporin x 10 Days (see Cephalosporins)
For Those Not Anaphylactically Penicillin-Sensitive, Clindamycin x 10 Days (see Clindamycin)
For Those Not Anaphylactically Penicillin-Sensitive, Azithromycin x 5 Days (see Azithromycin)
For Those Not Anaphylactically Penicillin-Sensitive, Clarithromycin x 10 Days (see Clarithromycin)
If Warranted (and Not Contraindicated), Adjunctive Use of an Analgesic/Antipyretic (Acetaminophen, NSAID) for the Treatment of Moderate-Severe Symptoms or Control of High Fever Should Be Considered in Addition to Antibiotic Therapy in the Treatment of Streptococcus Pyogenes Pharyngitis (Strong Recommendation, High Quality of Evidence)
Aspirin Should Be Avoided in Children (Strong Recommendation, Moderate Quality of Evidence)
Adjunctive Therapy with a Corticosteroid is Not Recommended in the Treatment of Streptococcus Pyogenes Pharyngitis (Weak Recommendation, Moderate Quality of Evidence)
Relationship Between Recurrent Episodes of Apparent Streptococcus Pyogenes Pharyngitis and Chronic Pharyngeal Streptococcus Pyogenes Carriage
Clinicians Caring for Patients with Recurrent Episodes of Pharyngitis Associated with Laboratory Evidence of Streptococcus Pyogenes Pharyngitis Should Consider that the Patient May Be Experiencing >1 Episode of Bona Fide Streptococcal Pharyngitis at Close Intervals, But They Should Also Be Alert to the Possibility that the Patient May Actually Be a Chronic Pharyngeal Streptococcus Pyogenes Carrier Who is Experiencing Repeated Viral Pharyngitis (Strong Recommendation, Moderate Quality of Evidence)
Streptococcus Pyogenes Carriers Do Not Ordinarily Justify Efforts to Identify Them, Nor Do They Generally Require Antimicrobial Therapy Because Streptococcus Pyogenes Carriers are Unlikely to Spread Streptococcus Pyogenes Pharyngitis to Their Close Contacts and are at Little or No Risk for Developing Suppurative or Non-Suppurative Complications (Such as Acute Rheumatic Fever) (Strong Recommendation, Moderate Quality of Evidence)
Tonsillectomy is Not Recommended Solely to Reduce the Frequency of Streptococcus Pyogenes Pharyngitis (Strong Recommendation, High Quality of Evidence)
References
General
Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):1279 [MEDLINE]
Guideline for the management of acute sore throat. Clin Microbiol Infect. 2012;18 Suppl 1:1 [MEDLINE]
Epidemiology
The prediction of streptococcal pharyngitis in adults. J Gen Intern Med. 1986;1(1):1 [MEDLINE]
Incidence and pathogenicity of Arcanobacterium haemolyticum during a 2-year study in Ottawa. Clin Infect Dis. 1995;21(1):177 [MEDLINE]
Epidemiologic evidence for Lancefield group C beta-hemolytic streptococci as a cause of exudative pharyngitis in college students. J Clin Microbiol. 1997;35(1):1 [MEDLINE]
The clinical presentation of Fusobacterium-positive and streptococcal-positive pharyngitis in a university health clinic: a cross-sectional study. Ann Intern Med. 2015;162(4):241 [MEDLINE]
Upper respiratory tract infections in general practice: diagnosis, antibiotic prescribing, duration of symptoms and use of diagnostic tests. Scand J Infect Dis. 2002;34(12):880 [MEDLINE]
Burden of acute sore throat and group A streptococcal pharyngitis in school-aged children and their families in Australia. Pediatrics. 2007;120(5):950 [MEDLINE]
Etiology
Transmission of the common cold to volunteers under controlled conditions. 1 The common cold as a clinical entity. Arch Intern Med 1958; 101: 267–78 [MEDLINE]
Group A streptococci, mycoplasmas, and viruses associated with acute pharyngitis. JAMA. 1967;202(6):455 [MEDLINE]
Pharyngitis in adults: the presence and coexistence of viruses and bacterial organisms. Ann Intern Med. 1989;110(8):612 [MEDLINE]
Pharyngitis associated with herpes simplex virus in college students. Pediatr Infect Dis J. 1993;12(4):280 [MEDLINE]
Acute pharyngitis: etiology and diagnosis. Pediatrics. 1996;97(6 Pt 2):949 [MEDLINE]
Pharyngitis. Prim Care. 1996 Dec;23(4):719-39. doi: 10.1016/s0095-4543(05)70359-6 [MEDLINE]
Acute pharyngitis. N Engl J Med. 2001;344(3):205 [MEDLINE]
Effects of acetylsalicylic acid on sore throat pain and other pain symptoms associated with acute upper respiratory tract infection. Pain Med. 2003 Jun;4(2):118-24. doi: 10.1046/j.1526-4637.2003.03019.x [MEDLINE]
Aetiology of acute pharyngitis: the role of atypical bacteria. J Med Microbiol. 2004 Jul;53(Pt 7):645-51 [MEDLINE]
Prevalence of Fusobacterium necrophorum and other upper respiratory tract pathogens isolated from throat swabs. Br J Biomed Sci. 2005;62(2):66 [MEDLINE]
Fusobacterium necrophorum as the cause of recurrent sore throat: comparison of isolates from persistent sore throat syndrome and Lemierre’s disease. J Infect. 2005;51(4):299 [MEDLINE]
Detection of Fusobacterium necrophorum subsp. funduliforme in tonsillitis in young adults by real-time PCR. Clin Microbiol Infect. 2007;13(7):695 [MEDLINE]
A six-month audit of the isolation of Fusobacterium necrophorum from patients with sore throat in a district general hospital. Br J Biomed Sci. 2007;64(2):63 [MEDLINE]
Clinical presentation and diagnosis of primary HIV-1 infection. Curr Opin HIV AIDS. 2008 Jan;3(1):10-5. doi: 10.1097/COH.0b013e3282f2e295 [MEDLINE]
Role of non-group a streptococci in acute pharyngitis. J Am Board Fam Med. 2009;22(6):663 [MEDLINE]
The role of Mycoplasma in upper respiratory infections. Curr Infect Dis Rep. 2009;11(3):198 [MEDLINE]
Postoperative sore throat: more answers than questions. Anesth Analg. 2010;111(4):831 [MEDLINE]
Environmental and non-infectious factors in the aetiology of pharyngitis (sore throat). Inflamm Res. 2012;61(10):1041 [MEDLINE]
Notes from the Field: Increase in Human Cases of Tularemia–Colorado, Nebraska, South Dakota, and Wyoming, January-September 2015. MMWR Morb Mortal Wkly Rep. 2015;64(47):1317 [MEDLINE]
Syphilis Trends among Men Who Have Sex with Men in the United States and Western Europe: A Systematic Review of Trend Studies Published between 2004 and 2015. PLoS One. 2016;11(7):e0159309 [MEDLINE]
Teacher’s voice: vocal tract discomfort symptoms, vocal intensity and noise in the classroom. Codas. 2016;28(2):168 [MEDLINE]
Vocal Tract Discomfort and Risk Factors in University Teachers. J Voice. 2016;30(4):507.e1. [MEDLINE]
Diagnosis
Streptococcal antigen in the pharynx after initiation of antibiotic therapy. Pediatr Infect Dis J. 1987;6(5):489 [MEDLINE]
Duration of positive throat cultures for group A streptococci after initiation of antibiotic therapy. Pediatrics. 1993;91(6):1166 [MEDLINE]
Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):1279 [MEDLINE]
Guideline for the management of acute sore throat. Clin Microbiol Infect. 2012;18 Suppl 1:1 [MEDLINE]
Reassessment of the Role of Rapid Antigen Detection Tests in Diagnosis of Invasive Group A Streptococcal Infections. J Clin Microbiol. 2016;54(4):994 [MEDLINE]
Treatment
Principles of appropriate antibiotic use for acute pharyngitis in adults. Ann Intern Med. 2001;134(6):506 [MEDLINE]
Impact on antibiotic prescription of rapid antigen detection testing in acute pharyngitis in adults: a randomised clinical trial. Br J Gen Pract. 2011;61(586):e244 [MEDLINE]
Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):1279 [MEDLINE]
Guideline for the management of acute sore throat. Clin Microbiol Infect. 2012;18 Suppl 1:1 [MEDLINE]