Scleroderma (see Scleroderma): antibodies against VWF
Systemic Lupus Erythematosus (SLE)s (see Systemic Lupus Erythematosus): antibodies against VWF (higher MW multimers appear to be more susceptible to degradation by this mechanism)
Dextran (see Dextran): branched polysaccharides of 40 or 70 kDa which inhibit platelet factor-3 availability, adsorb to platelets, and decrease plasma factor VIII-VWF -> inhibit platelet aggregation + secretion
Aortic Stenosis (AS) (see Aortic Stenosis): high intravascular shear forces -> increased clearance of high MW multimers
Heyde’s Syndrome (Constellation of Aortic Stenosis and Gastrointestinal Angiodysplasia): high intravascular shear forces across stenotic aortic valve leads to increased clearance of high MW multimers, possibly due to increased susceptibility to serum proteases
Disseminated Intravascular Coagulation (DIC) (see Disseminated Intravascular Coagulation): hyperfibrinolytic state -> VWF degradation by proteolytic enzymes (such as plasmin)
Essential Thrombocythemia (see Essential Thrombocythemia): increased numbers of platelets may result in increased VWF binding -> increased VWF clearance
Lymphoma (see Lymphoma): adsorption of VWF to lymphoma cells
Heyde’s Syndrome (constellation of aortic stenosis + gastrointestinal angiodysplasia): high intravascular shear forces across stenotic aortic valve leads to increased clearance of high MW multimers, possibly due to increased susceptibility to serum proteases
Von Willebrand Factor (vWF) are Long Stringlike Molecules Synthesized by Vascular Endothelial Cells and Megakaryocytes
vWF is Synthesized as a Single VWF Precursor: cleavage and assembly into disulfide-linked multimers occurs in plasma
VWF Activity is Distributed Among a Series of Plasma Multimers: ranging in size from MW 400k-20 million
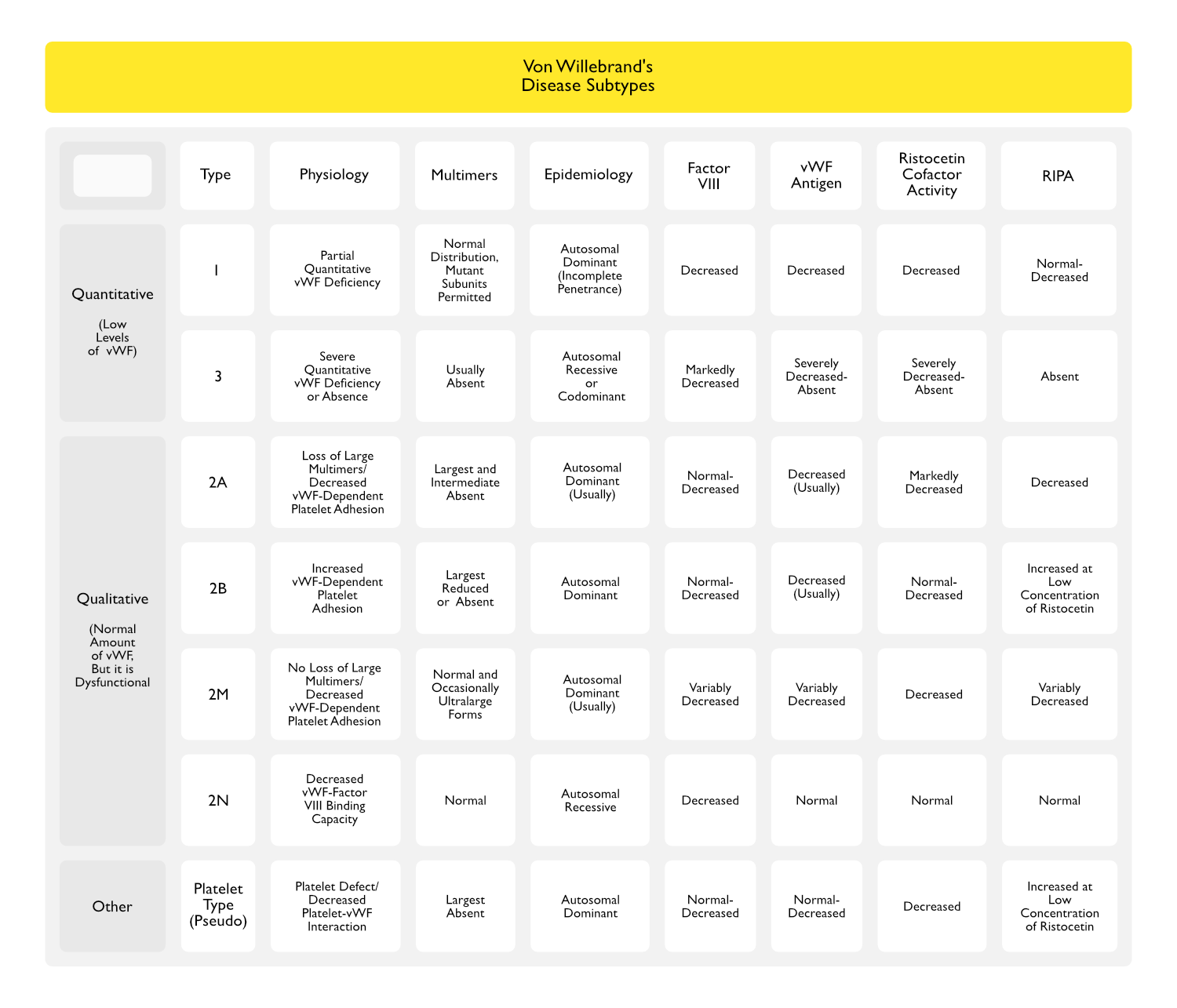
Modest Reduction in Plasma VWF Concentration OR Selective Loss of One of the High Molecular Weight Multimers Results in Decreased Platelet Adhesion and Clinical Bleeding
Locations of Von Willebrand Factor
VWF Circulates as a Series of Multimers Formed from a Basic Dimer Subunit
Ultralarge Von Willebrand Factor Multimers Attach to the Endothelial Surface
Von Willebrand Factor Binds to the Platelet GP1b Receptor
Platelet Granule Release of Procoagulant Molecules (from Alpha Granules) and Cofactors (from Dense Granules)
Receptor Activation and Expression
Functions of Von Willebrand Factor in Primary Hemostasis
VWF Forms an Adhesive Bridge Between Platelets and Exposed Vascular Subendothelial Basement Membrane
VWF Forms an Adhesive Bridge Between Adjacent Platelets at Sites of Endothelial Injury
VWF is the Plasma Carrier Protein for Factor VIII While it is Inactive in the Circulation: factor VIII degrades rapidly when not bound to vWF
Diagnosis
INR: prolonged with deficiency of factor VII and common pathway factors (fibrinogen, II, V, and X)
PTT: prolonged with deficiency/inhbitors of factors VIII, IX, XI, XII, as well as common pathway factors
However, PTT is less sensitive for deficiency/inhbitors of common pathway factors -> this is why vitamin K deficiency (with decreased factors II, VII, IX, X) prolongs INR more than PTT
Thrombin Time: measures how fast given amount of thrombin turns fibrinogen into fibrin -> therefore, is designed to detect quantitative or qualitative problems with fibrin
Can be prolonged by high levels of fibrin degradation products
Very sensitive to heparin
Reptilase Time: used to determine if prolonged thrombin time is due to heparin
Insensitive to heparin
1:1 Mix: mix control plasma (with 100% activity of each factor) + patient plasma to determine if a factor deficiency vs inhibitor is present
As factor levels of 50% or higher are sufficient for a normal INR/PTT, 1:1 mix will correct INR/PTT in presence of a factor deficiences, but not in presence of a factor inhibitor
PTT with Polybrene or Heparinase:used to neutralize heparin in the sample to determine if prolonged PTT is due to heparin
PTT with Excess Phospholipid: used to detect presence of anti-phospholipid antibody (lupus anticoagulant, etc)
Bleeding Time: assesses for platelets defects (relatively insensitive for factor deficiencies or inhibitors)
Platelet Function Analysis (PFA): essentially an in vitro bleeding time assay which assesses different components of platelet activation (in response to ADP, epinephrine, collagen)
Von Willebrand Factor Antigen: quanitifies the amount of Von Willebrand factor -> decreased in Von Willebrand Disease
Normal Level of VWF: 10 mg/L
Ristocetin Cofactor Test: evaluates function of Von Willebrand factor by testing ristocetin-induced platelet aggregation of normal platelets in presence of patient’s plasma
Most sensitive and specific test for Von Willebrand disease -> decreased in all types of Von Willebrand disease
Assesses the binding of Von Willebrand factor to platelet GP1b
Ristocetin-Induced Platelet Aggregation (RIPA): evaluates function of Von Willebrand factor by testing ristocetin-induced platelet aggregation of patient’s platelets in presence of patient’s plasma
Less sensitive and specific than ristocetin cofactor test
Usually decreased in Von Willebrand disease, but may be normal in some cases
In type IIB Von Willebrand disease: platelets are hyperresponive to ristocetin (platelets aggregate in response to abnormally low ristocetin concentration)
Factor VIII Activity/Level (factor VIII activity assay is performed -> level is inferred from activity): decreased in factor VIII deficiency and Von Willebrand disease
Von Willebrand factor normally carries factor VIII (this prolongs factor VIII half-life) -> therefore, if Von Willebrand factor binding of factor VIII is impaired or Von Willebrand factor is low, then, factor VIII level is low
Stepwise Evaluation of Coagulopathy
Step 1 (assessment for platelet problem): platelet count, PFA
Step 2 (assessment for single factor deficiency): INR/PTT, factor assays
Step 3 (assessment for multiple factor deficiency): INR/PTT, thrombin time, factor assays
Step 4 (assessment for circulating anticoagulant): PTT with polybrene or heparinase, PTT with 1:1 mix, PTT with excess phospholipid, thrombin time
Tranexamic Acid (Lysteda, Cyklokapron) (see Tranexamic Acid)
Administration: IV
Adverse Effects:
Acquired Von Willebrand Disease
DDAVP and Plasma Derivatives are Often Not Effective: therapy should focus on treating the primary etiology
References
High dose of tranexamic acid for treatment of severe menorrhagia in patients with von Willebrand disease. J Thromb Thrombolysis. 2002 Dec;14(3):255-7
Acquired and Reversible von Willebrand Disease With High Shear Stress Aortic Valve Stenosis. Ann Thorac Surg 2006;81:490-494
Acquired von Willebrand Syndrome After Continuous-Flow Mechanical Device Support Contributes to a High Prevalence of Bleeding During Long-Term Support and at the Time of Transplantation. J Am Coll Cardiol, 2010; 56:1207-1213