Disseminated Intravascular Coagulation (DIC) is Observed in Approximately 1% of Admissions to Tertiary Care Hospitals
In a Japanese Series of 123,231 Patients Admitted to University Hospitals, Approximately 1,286 Patients were Diagnosed with Disseminated Intravascular Coagulation (DIC) (Prevalence: 1%) (Pol J Pharmacol, 1996) [MEDLINE]
Etiology
Relative Frequencies of Etiologies of Disseminated Intravascular Coagulation (DIC)
The Most Common Etiologies of Disseminated Intravascular Coagulation (DIC) are Infection, Malignancy, and Trauma/Surgery (Thromb Haemost, 1978) [MEDLINE] (Thromb Haemost, 1980) [MEDLINE]
Each Account for Approximately 10-20% of the Total Cases (Depending on the Study)
Hereditary Homozygous Protein C Deficiency Commonly Presents in Early Infancy with Purpura Fulminans, But Older Patients are Also Occasionally Seen
In Contrast, Heterozygous Protein C Deficiency with Venous Thromboembolism Typically Does Not Have Disseminated Intravascular Coagulation (DIC) as a Component of its Pathogenesis
Severe Cases of Heparin-Induced Thrombocytoepnia Can Be Associated with Disseminated Intravascular Coagulation (DIC) in Some Patients (J Thromb Haemost, 2017) [MEDLINE]
Management
Although Standard Anticoagulant Therapy for Heparin-Induced Thrombocytopenia Would Be Expected to Be Effective, Published Experience Indicates Frequent Failure of Partial Thromboplastin Time (PTT)-Adjusted Anticoagulants (Argatroban, Bivalirudin), Probably Related to Underdosing in the Setting of Heparin-Induced Thrombocytopenia-Associated Disseminated Intravascular Coagulation (DIC), Know as “PTT Confounding”
Therefore, Non-PTT-Adjusted Therapies (Using Danaparoid, Fondaparinux, Apixaban, Rivaroxaban) are Suggested, Especially for Long-Term Management of Persistent Heparin-Induced Thrombocytopenia
Malaria (Severe) (see Malaria) (Parasitol Res, 2008) [MEDLINE]
In a Series of 35 Patients Who Met Criteria for Systemic Inflammatory Response Syndrome (SIRS) for ≥4 Consecutive Days, Disseminated Intravascular Coagulation (DIC) was Observed in 83% of Cases (Lancet, 1997) [MEDLINE]
In a Study of Patients Hospitalized with SARS-CoV-2 Pneumonia, Disseminated Intravascular Coagulation (DIC) was Diagnosed (Using ISTH Criteria) in Only 1 Patient Who Survived vs 15 Patients (71%) Who Died (J Thromb Haemost, 2020) [MEDLINE]
Median Time from Admission to Development of Disseminated Intravascular Coagulation (DIC) was 4 Days (Range: 1-12 Days)
Diagnosis of Disseminated Intravascular Coagulation (DIC) Post-Cardiopulmonary Bypass is Clinically Difficult (Since the Identification of Microthrombi is Difficult and Hemolysis and Consumption of Coagulation Factors May Be Commonly Observed Following Cardiopulmonary Bypass)
Pregnancy-Associated Disseminated Intravascular Coagulation (DIC) Accounts for Approximately 1-5% of All Disseminated Intravascular Coagulation (DIC) Cases in Resource-Abundant Countries (with Higher Percetages in Resource-Limited Countries) (Thromb Res, 2009) [MEDLINE]
In Population-Based Studies, the Prevalence of Pregnancy-associated Disseminated Intravascular Coagulation (DIC) Ranges from 0.03-0.35% of Delivery Hospitalizations (J Obstet Gynaecol Can, 2012) [MEDLINE] (Obstet Gynecol, 2012) [MEDLINE] (PLoS One, 2014) [MEDLINE]
In Studies from the United States, the Prevalence Has Been Reported to Be 0.13% (J Obstet Gynaecol Can, 2012) [MEDLINE]
Disseminated Intravascular Coagulation (DIC) is Usually Fulminant in the Obstetric Setting and Associated with Up to 25% of Maternal Deaths (Obstet Gynecol, 2015) [MEDLINE]
Disseminated Intravascular Coagulation (DIC) Has Been Reported in the Perioperative Period Associated with Surgical Repair and Thoracic Endovascular Aortic Repair (TEVAR) of Aortic Dissection (Medicine-Baltimore, 2016) [MEDLINE] (BMC Cardiovasc Disord, 2022) [MEDLINE]
Disseminated Intravascular Coagulation (DIC) Has Been Reported with Aortic Dissection (J Vasc Surg Cases Innov Tech, 2018) [MEDLINE]
Chronic Disseminated Intravascular Coagulation (DIC) Has Been Reported in Both Aortic Aneurysm/Aortic Dissection (Case Rep Hematol, 2019) [MEDLINE]
Clinical
High Preoperative Disseminated Intravascular Coagulation (DIC) Scores are Associated with Communicating-Type Acute Stanford Type A Aortic Dissection and Larger False Lumen Size (J Vasc Surg, 2022) [MEDLINE]
However, Some Consider This to Be a Coagulopathy/Thrombotic Microangiopathy Which is Distinct from Disseminated Intravascular Coagulation (DIC) (Semin Thromb Hemost, 2010) [MEDLINE]
Disseminated Intravscular Coagulation (DIC) is Associated with Microvascular Thrombi, Which Contain Fibrin and Platelets
In Contrast, Some of the other thrombotic microangiopathies (TMAs), such as thrombotic thrombocytopenic purpura (TTP) and complement-mediated hemolytic uremic syndrome (HUS), are characterized by platelet-rich microthrombi without significant Fibrin Clot Formation or Consumption Coagulopathy
Therefore, Other Thrombotic Microangiopathies Generally Present with Thrombocytopenia with Niormal Coagulation Studies
Diagnosis
General Comments
Findings Such as Thrombocytopenia, Hypofibrinogenemia, and Elevated D-Dimer are Considered to Be Relatively Sensitive for the Diagnosis of Disseminated Intravascular Coagulation (DIC), But Not Specific
However, Data from Clinical Trials Addressing Sensitivity and Specificity are Lacking
Many of the Laboratory Abnormalities Used to Diagnose Disseminated Intravascular Coagulation (DIC) are Present in Normal Pregnancy
Testing is Often Repeated Serially to Determine if Coagulation and Fibrinolysis are Worsening or Improving
The Frequency of Repeat Testing Depends on the Severity of Clinical Findings
Thromboelastography (TEG)/Rotational thromboelastometry (ROTEM) (see Thromboelastography)
Thromboelastography Provides a Global Assessment of Hemostasis Using a Whole Blood Sample
Includes Assessment of the Contributions of Platelets, Fibrinogen, and Coagulation Factors, as Well as Fibrinolysis
Thromboelastography Can Be Particularly Useful in the Diagnosis of Dilutional Coagulopathy, Which May Occur in the Setting of Postpartum Hemorrhage with Ongoing Active Transfusion (Scand J Trauma Resusc Emerg Med, 2012) [MEDLINE]
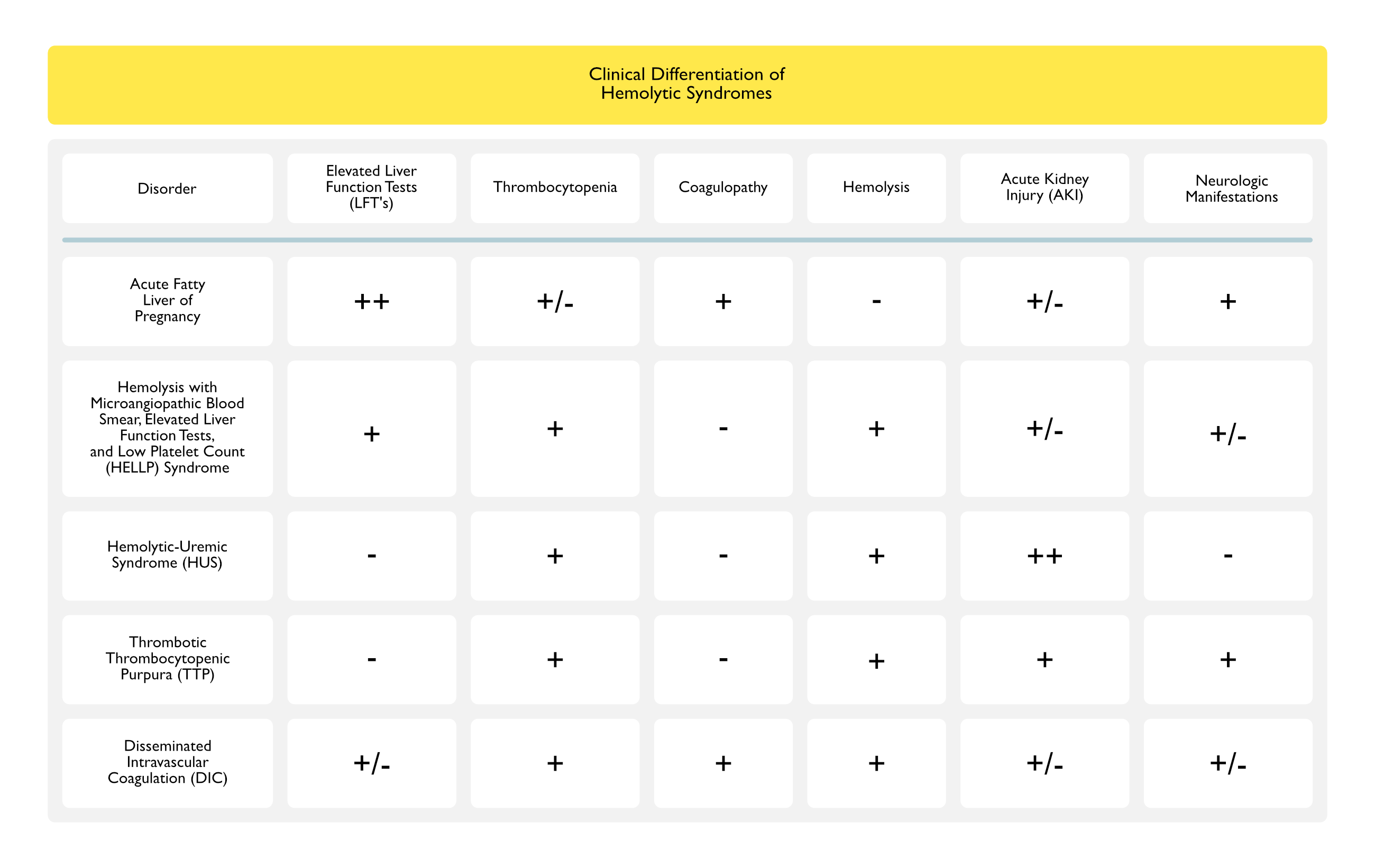
Clinical Differentiation of Hemolytic Syndromes
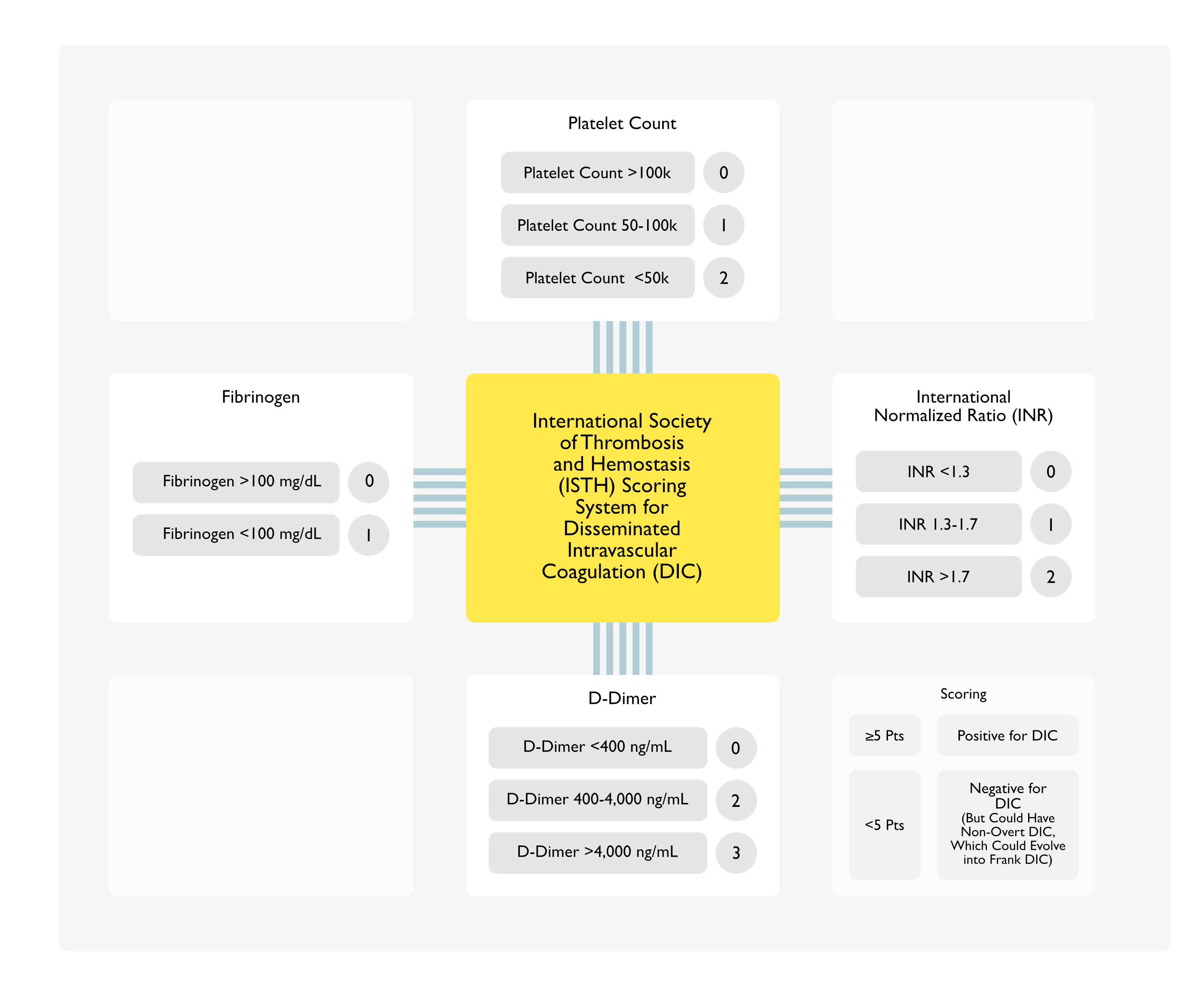
International Society of Thrombosis and Hemostasis Disseminated Intravascular Coagulation (DIC) Scoring System (Thromb Res, 2015) [MEDLINE] (Ann Lab Med, 2016) [MEDLINE]
General Comments
The International Society of Thrombosis and Hemostasis (ISTH) Disseminated Intravascular Coagulation (DIC) Scoring System Utilizes Laboratory Features, Including the International Normalized Ratio (INR), Platelet Count, Fibrinogen Level, and D-Dimer
Scoring System Has Been Validated, But is Not Widely Used
International Society of Thrombosis and Hemostasis Disseminated Intravascular Coagulation (DIC) Scoring System Adapted for Use in Pregnancy (PLoS One, 2014) [MEDLINE]
Parameters
Platelets <50k or 100-185k or Fibrinogen 400-450 mg/dL: 1 points
Platelets 50k-100k: 2 points
PT Difference 0.5-1.0: 5 points
Fibrinogen 300-400 mg/dL): 6 points
PT Difference 1-1.5: 12 points
PT Difference >1.5 or Fibrinogen ≤300 mg/dL: 25 points
Score
Cutoff Point of ≥26 Had a Sensitivity of 88%, a Specificity of 96%, Positive Likelihood Ratio of 22, and a Negative Likelihood Ratio of 0.125 for the Diagnosis of Disseminated Intravascular Coagulation (DIC)
Differentiation of Disseminated Intravascular Coagulation (DIC) from Severe Liver Disease (see Cirrhosis)
Liver Disease Severe Enough to Impair the Hepatic Synthesis of Coagulation Factors Can Result in a Severe Coagulopathy
Severe Liver Disease is Associated with Decreases in Both Procoagulant and Anticoagulant Factors as Well as Thrombocytopenia (and Therefore, May Result in Bleeding or Thrombosis)
Similar to Disseminated Intravascular Coagulation (DIC)
The Decrease in Coagulation Factors and Thrombocytopenia in Severe Liver Disease are Due to a Combination of Hypersplenism and Thrombopoietin Deficiency
Liver is the Primary Site of Thrombopoietin Synthesis
Patients with Severe Liver Disease Typically Present with a Known Source of Liver Injury (Such as Acute Hepatitis or Alcoholic Cirrhosis) and Abnormal Liver Function Tests (Although the Transaminases May Appear to Normalize if Liver Synthetic Function is Severely Impaired)
Dissimilar to Disseminated Intravascular Coagulation (DIC)
Some Clinicians Utilize the Measurement of Factor VIII Levels to Aid in the Differentiation of Disseminated Intravascular Coagulation (DIC) from Severe Liver Disease, Since Factor VIII is Not Produced by Hepatocytes and Therefore, is Frequently Decreased in Disseminated Intravascular Coagulation (DIC) and Increased in Severe Liver Disease
Differentiation of Disseminated Intravascular Coagulation (DIC) from Thrombotic Microangiopathy (TMA) (see xxxx)
XXX
Differentiation of Disseminated Intravascular Coagulation (DIC) from Hemophagocytic Lymphohistiocytosis (HLH) (see Hemophagocytic Lymphohistiocytosis)
Hemophagocytic Lymphohistiocytosis is an Aggressive, Life-Threatening Syndrome of Excessive Immune Activation Which, Untreated, Can Result in Tissue Damage and a High Mortality Rate
Acute Illness with Cytopenias, Prolonged Clotting Times, Hypofibrinogenemia, and Increased D-Dimer May Be Present
Similar to Disseminated Intravascular Coagulation (DIC)
Patients May Also Have Fever, Hepatic Dysfunction, Neurologic Deficits, and Severe Hyperferritinemia
Patients with Hemophagocytic Lymphohistiocytosis (HLH) Have Evidence of Immune Activation, with Pathogenic Variants in One of Several Immune Regulatory Genes and Often Including Low/Absent Natural Killer (NK) Cell Activity, Increased Soluble Interleukin 2 (IL-2) Receptor α (sCD25) and/or CXCL19
Dissimilar to Disseminated Intravascular Coagulation (DIC)
Patients with Hemophagocytic Lymphohistiocytosis (HLH) Typically Require Treatment Directed at the Underlying Etiology (if Present), as Well as Treatment Directed at Stopping the Immune Activation
Dissimilar to Disseminated Intravascular Coagulation (DIC)
The Most Impaired Coagulation Tests are the Prothrombin Iime/International Normalized Ratio (INR), Partial Thromboplastin Time, Thrombin Time, and the Platelet Count
The Degree of Abnormality of These Coagulation Tests is Correlated to the Degree of Organ Involvement
However, Since Patients with Sepsis/Malignancy/Other Inflammatory Disorders May Have Significantly Increased Fibrinogen Synthesis (as Fibrinogen is an Acute Phase Reactant), a Normal Plasma Fibrinogen Level May Represent a Substantial Consumption (and a Significant Abnormality) for that Patient Despite the Value Being in the Normal Range
Since Factor VIII is Not Synthesized by the Liver, it is Often High in the Setting of Liver Disease, But is Decreased in the Setting of Disseminated Intravascular Coagulation (DIC)
Changes Consistent with Microangiopathic Hemolytic Anemia (MAHA) (see Hemolytic Anemia): schistocytes, helmet cells, etc
Microangiopathic Changes May Be Less Pronounced than Those Observed in Other Thrombotic Microangiopathies (such as Thrombotic Thrombocytopenic Purpura, TTP)
Severe Anemia Due to Microangiopathic Hemolytic Anemia is Uncommon (Although Most of the Underlying Etiologies of Disseminated Intravascular Coagulation Can Cause Anemia by Other Mechanisms, Such as Bone Marrow Suppression, Anemia of Chronic Disease/Inflammation, etc)
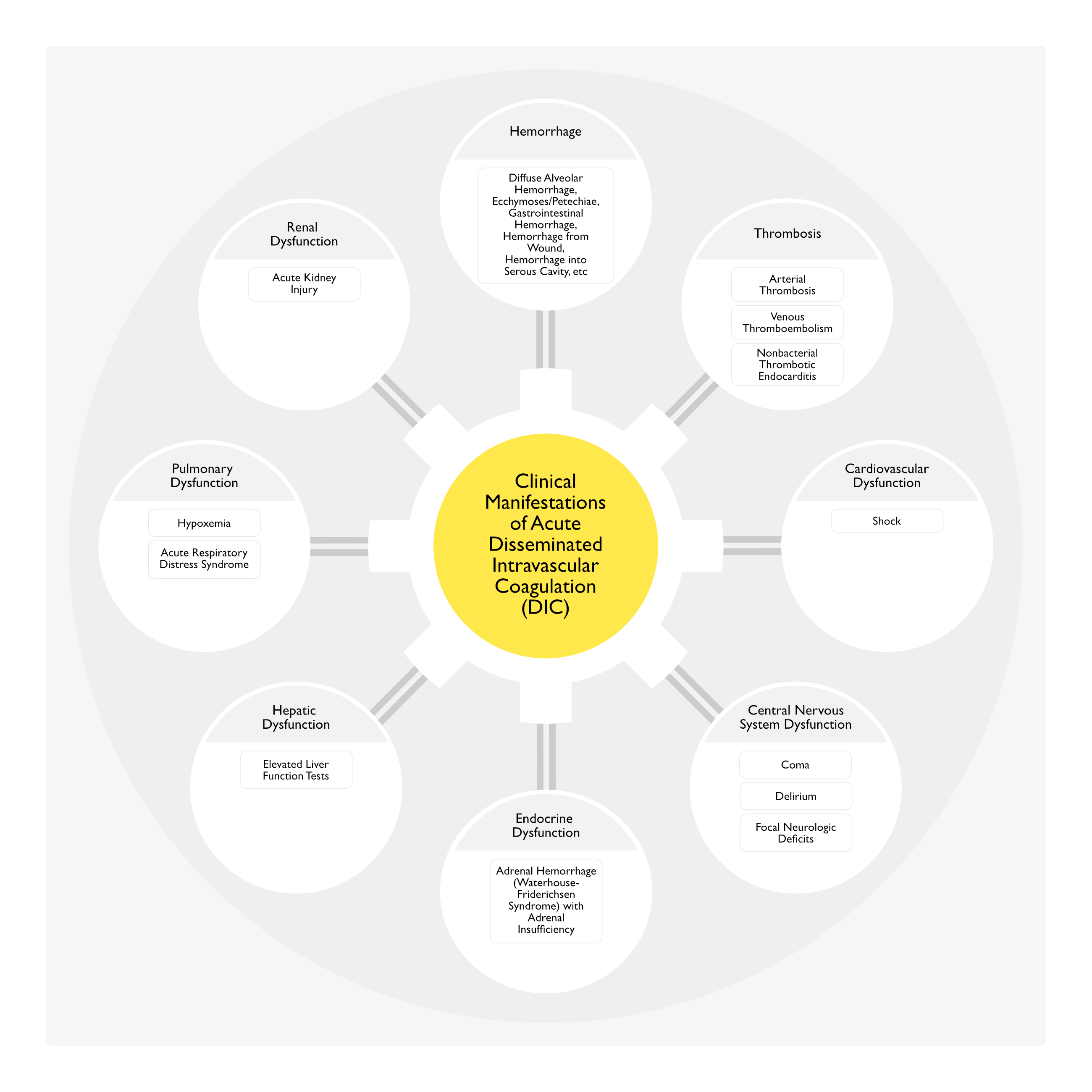
Clinical
General Comments
In Trauma-Associated Cases, Pulmonary Dysfunction is Common, While Hepatic/Renal Dysfunction are Rare (Thromb Haemost, 1978) [MEDLINE]
In Contrast, in Infection-Associated Cases, Hepatic/Renal Dysfunction are Common, While Pulmonary Dysfunction is Rare (Thromb Haemost, 1978) [MEDLINE]
This Variability Indicates that the Clinical Manifestations are Affected Not Only by the Process of Intravascular Coagulation, But Also by the Underlying Clinical Disorder
Hemorrhage
General Comments
Hemorrhage is More Common in Acute Disseminated Intravascular Coagulation (DIC) Than in Chronic Disseminated Intravascular Coagulation (DIC)
Hemorrhage Occurs in 64% of Acute Disseminated Intravascular Coagulation (DIC) Cases (Thromb Haemost, 1978) [MEDLINE]
Acute Kidney Injury Occurs in 25% of Acute Disseminated Intravascular Coagulation (DIC) Cases (Thromb Haemost, 1978) [MEDLINE]
Prognosis
The mortality (overall 54.7%) increased independently with age, with the number of clinical manifestations and with the degree of abnormality of the above-mentioned four most impaired coagulation tests (Thromb Haemost, 1978) [MEDLINE]
In addition, older patients were more likely to have an increased number of clinical manifestations and more impaired coagulation tests
Mortality was similar in the various etiologies except for trauma patients in whom it was lower (30%)
Thrombin Time is More Sensitive than INR/PTT to the Effects of Increased D-Dimers and Fibrin Degradation Products in Chronic Disseminated Intravascular Coagulation (DIC)
Changes Consistent with Microangiopathic Hemolytic Anemia (MAHA) (see Hemolytic Anemia): schistocytes, helmet cells, etc
Microangiopathic Changes May Be Less Pronounced than Those Observed in Other Thrombotic Microangiopathies (such as Thrombotic Thrombocytopenic Purpura, TTP)
Severe Anemia Due to Microangiopathic Hemolytic Anemia is Uncommon (Although Most of the Underlying Etiologies of Disseminated Intravascular Coagulation Can Cause Anemia by Other Mechanisms, Such as Bone Marrow Suppression, Anemia of Chronic Disease/Inflammation, etc)
Clinical
Chronic Disseminated Intravascular Coagulation (DIC) May Be Asymptomatic
xx
Hemorrhage
General Comments
Hemorrhage is More Common in Acute Disseminated Intravascular Coagulation (DIC) Than in Chronic Disseminated Intravascular Coagulation (DIC)
Thrombosis
General Comments
Thrombosis is More Common in Chronic Disseminated Intravascular Coagulation (DIC) Than in Acute Disseminated Intravascular Coagulation (DIC)
Typically in the Setting of a Solid Tumor
Clinical Types
Arterial Thrombosis (Especially without a Clear Precipitating Factor) with Organ Ischemia
Hemodynamic Support (Pressors, Intravenous Fluids): as required
Mechanical Ventilation: as required
Treatment of Thrombotic Complications
Anticoagulation: as required to treat thrombotic complications
Treatment of Bleeding Complications
Antifibrinolytic Agents (Tranexamic Acid, Epsilon-Aminocaproic Acid, Aprotinin): contraindicated (since blockade of the fibrinolytic system may increase the risk of thrombosis)
However, these agents may be used in patients who have severe bleeding associated with a hyperfibrinolytic state
Antithombin: trials have shown this to be ineffective in DIC
One unit of cryoprecipitate (10-20 ml) contains the cold insoluble protein from one unit of FFP (contains vWF, factor VIII, factor XIII, fibrinogen, and fibrinonectin)
Some blood suppliers now provide one bag of pre-pooled cryoprecipitate which contains 5 (or more) units in 120-160 mL: use two bags of pre-pooled cryoprecipitate (ie: from 10 units of FFP)
Fresh Frozen Plasma (FFP) (see Fresh Frozen Plasma): as required to treat coagulopathy in the setting of significant hemorrhage or need for invasive procedures
Packed Red Blood Cells (see Packed Red Blood Cells): as required to treat hemorrhage-related anemia
Transfuse for Platelet Count <50k: in the setting of significant hemorrhage or need for invasive procedures
Transfuse for Platelet Count <10k: in all patients (due to the risk of spontaneous hemorrhage)
Prothrombin Complex Concentrates: likely contraindicated (due to risk of more thrombotic complications in the setting of an already hypercoagulable state)
Fresh Frozen Plasma (FFP) (see Fresh Frozen Plasma): the administration of FFP as a source of protein C is problematic because of the short plasma half-life of protein C
Due to short plasma protein C half-life, FFP 2-3 units may be administered approximately every 6 hrs
Protein C Concentrate (see Protein C Concentrate): proven to decrease mortality rate in purpura fulminans
Expected Course of Resolution
Factors Impacting the Rate of DIC Resolution: DIC does not usually resolve immediately once the inciting factor is corrected
Resolution requires the synthesis of coagulant factors (which are synthesized at different rates)
Resolution requires hepatic clearance of anticoagulant factors and fibrin degradation products
Resolution requires bone marrow production of new platelets (which may take several days)
Resolution of DIC-Related Laboratory abnormalities: usually improve within a few days after the inciting stimulus is removed
Impact of Renal Failure on the Rate of DIC Resolution: does not impact the rate DIC resolution (unless there is a component of hepatorenal syndrome or if the kidneys are a major site of thrombosis)
References
Epidemiology
Clinical aspects of DIC–disseminated intravascular coagulation. Pol J Pharmacol. 1996;48(1):73 [MEDLINE]
Etiology
Clinical and laboratory aspects of disseminated intravascular coagulation (DIC): a study of 118 cases. Thromb Haemost. 1978;39(1):122 [MEDLINE]
Maternal morbidity and mortality in 442 pregnancies with hemolysis, elevated liver enzymes, and low platelets (HELLP syndrome). Am J Obstet Gynecol. 1993;169(4):1000 [MEDLINE]
Use of protein-C concentrate, heparin, and haemodiafiltration in meningococcus-induced purpura fulminans. Lancet. 1997;350(9091):1590 [MEDLINE]
Multiorgan dysfunction and disseminated intravascular coagulation in children receiving lamotrigine and valproic acid. Neurology. 1997;49(5):1442-1444. doi:10.1212/wnl.49.5.1442 [MEDLINE]
Amniotic fluid embolism: decreased mortality in a population-based study. Obstet Gynecol. 1999;93(6):973 [MEDLINE]
Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost. 2001;86(5):1327 [MEDLINE]
Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br J Haematol. 2009;145(1):24 [MEDLINE]
Disseminated intravascular coagulation (DIC) in pregnancy and the peri-partum period. Thromb Res. 2009;123 Suppl 2:S63 [MEDLINE]
Snakebite doesn’t cause disseminated intravascular coagulation: coagulopathy and thrombotic microangiopathy in snake envenoming. Semin Thromb Hemost. 2010 Jun;36(4):444-51 [MEDLINE]
Acute disseminated intravascular coagulation in obstetrics: a tertiary centre population review (1980 to 2009). J Obstet Gynaecol Can. 2012 Apr;34(4):341-7 [MEDLINE]
Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstet Gynecol. 2012 Nov;120(5):1029-36 [MEDLINE]
DIC score in pregnant women–a population based modification of the International Society on Thrombosis and Hemostasis score. PLoS One. 2014;9(4):e93240 [MEDLINE]
Disseminated Intravascular Coagulation Syndromes in Obstetrics. Obstet Gynecol. 2015;126(5):999 [MEDLINE]- Amniotic Fluid Embolism. Obstet Gynecol Clin North Am. 2016;43(4):779 [MEDLINE]
Markers of Inflammation and Infection in Sepsis and Disseminated Intravascular Coagulation. Clin Appl Thromb Hemost. 2019 Jan-Dec:25:1076029619843338. doi: 10.1177/1076029619843338 [MEDLINE]
Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18(4):844 [MEDLINE]
Rare association of consumptive coagulopathy in visceral leishmaniasis: A case report. Trop Doct. 2021;51(1):120 [MEDLINE]
Diagnosis
Clinical and laboratory aspects of disseminated intravascular coagulation (DIC): a study of 118 cases. Thromb Haemost. 1978;39(1):122 [MEDLINE]
The use of D-dimer with new cutoff can be useful in diagnosis of venous thromboembolism in pregnancy. Eur J Obstet Gynecol Reprod Biol. 2010;148(1):27 [MEDLINE]
Current management of massive hemorrhage in trauma. Scand J Trauma Resusc Emerg Med. 2012;20:47 [MEDLINE]
DIC score in pregnant women–a population based modification of the International Society on Thrombosis and Hemostasis score. PLoS One. 2014;9(4):e93240 [MEDLINE]
Management of disseminated intravascular coagulation: a survey of the International Society on Thrombosis and Haemostasis. Thromb Res. 2015;136(2):239 [MEDLINE]
Current Pathological and Laboratory Considerations in the Diagnosis of Disseminated Intravascular Coagulation. Ann Lab Med. 2016;36(6):505 [MEDLINE]
Clinical
Clinical and laboratory aspects of disseminated intravascular coagulation (DIC): a study of 118 cases. Thromb Haemost. 1978;39(1):122 [MEDLINE]