Esophageal Varices with Active Bleeding: vascular supply to esophageal varices originates from stomach and traverses the gastroesophageal (GE) junction -> this allows mechanical compression of variceal blood supply
Mallory-Weiss Tear with Active Bleeding: use of Sengstaken-Blakemore or Minnesota tube has been reported in some cases to control active bleeding
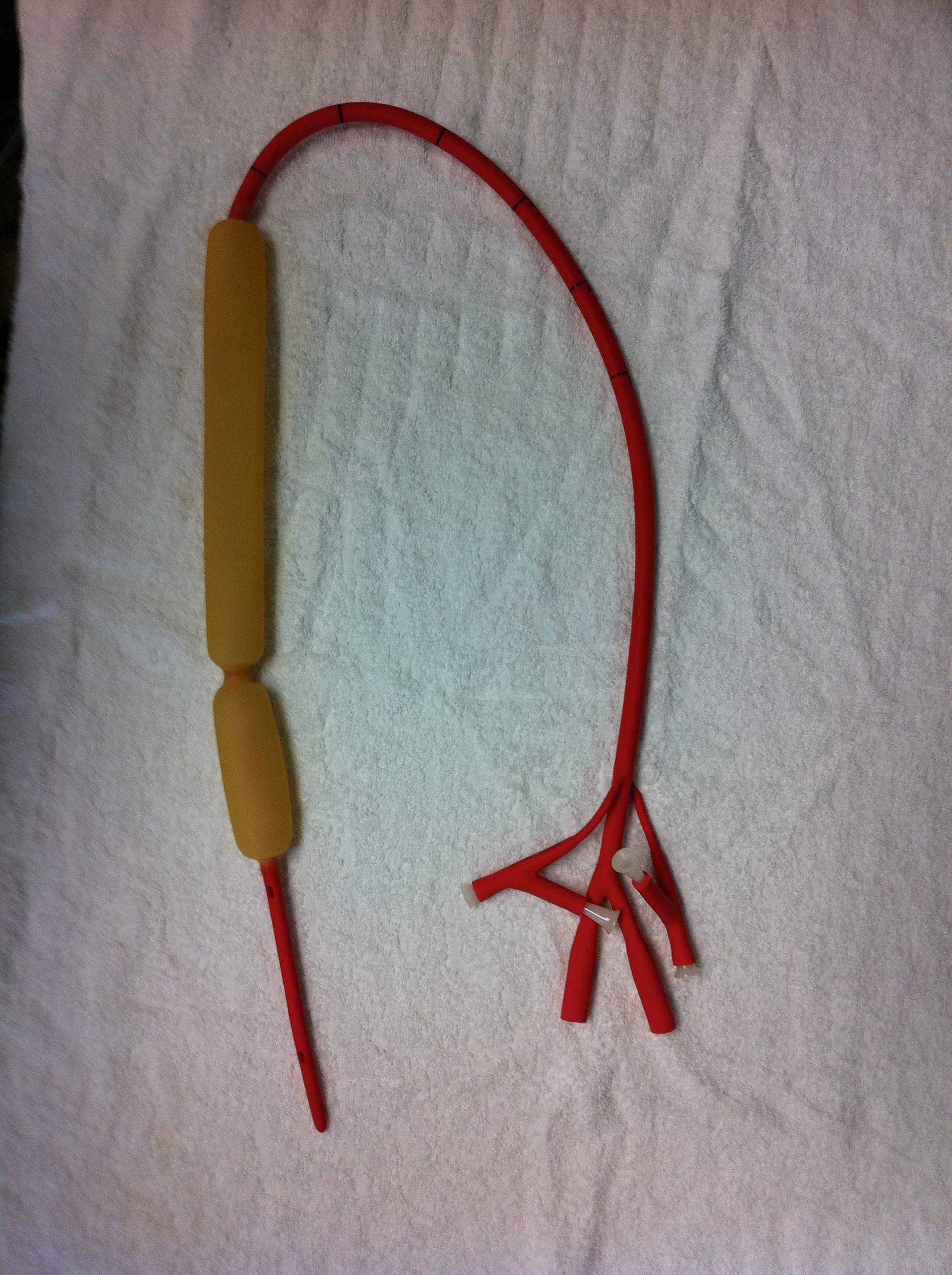
Tube Structure: 3-lumen with gastric aspiration port (may require additional NG tube placement, is esophageal aspiration is required)
Directions for Tube Placement
Intubate patient for airway protection
Place patient supine or in left lateral decubitus position
Place hockey helmet
Remove white pegs from esophageal and gastric balloon ports -> test balloons with air
Deflate balloons completely, lubricate tube, and insert to at least 50 cm
Using 60 ml catheter-tip syringe and blue tubing clamps, inflate gastric balloon with 200 ml of air
Tug tube back -> should feel resistance, if gastric balloon is properly in stomach
Secure tube to rung of hockey helmet using chest tube white tie, keeping tension (take note of the tube marking at the rung)
Add additional 250 ml of air to gastric balloon -> total volume = 450 ml of air
Keep clamped and place white peg back into gastric balloon port
Optionally (though usually not necessary), inflate esophageal balloon using manometer to 25-40 mm Hg
Connect esophageal/gastric aspiration ports to low-intermittent suction
Obtain CXR and KUB to confirm placement and confirm ETT positioning
Deflate esophageal balloon for 10 min out of every 2 hrs -> esophageal balloon inflation should not be used for >12-24 hrs in total duration
Complications
Migration of Gastric Balloon into Esophagus: causes abrupt tracheal compression and high peak inspiratory pressure (PIP) on ventilator
Esophageal Necrosis: in cases where esophageal balloon is not periodically deflated
Minnesota Tube
Indications: same as above for Sengstaken-Blakemore tube
Tube Structure: 4-lumen with esophageal gastric aspiration ports (does not require additional NG tube placement)
Also, Minnesota tube has larger gastric balloon than Sengstaken-Blakemore tube
Directions for Tube Placement: same as above for Sengstaken-Blakemore tube
Complications: same as above for Sengstaken-Blakemore tube
References
Prevalence of paraesophageal varices and gastric varices in patients achieving variceal obliteration by banding ligation and by injection sclerotherapy. Gastrointest Endosc. 1999 Apr;49(4 Pt 1):428-36