Obesity is Characterized by Increased Oxygen Consumption and Carbon Dioxide Production
Physiology
Increased Metabolic Activity in Excess Adipose Tissue and Increased Work Required of the Supportive Tissues [Semin Anesth. 2002; 21:46]
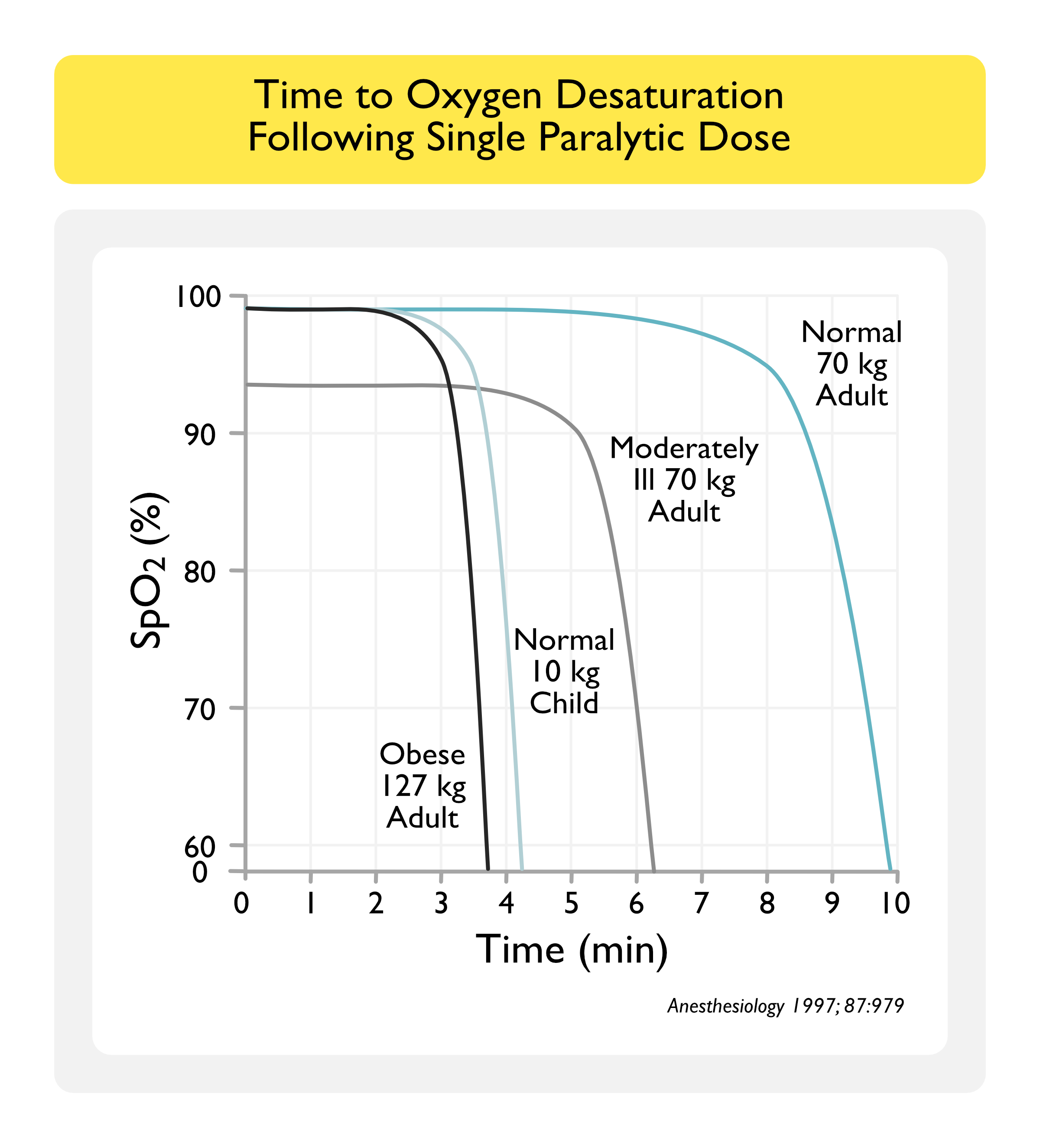
Consequently, the Time to Desaturation (and the “Safe Apnea Period” During Rapid Sequence Intubation) are Decreased (Anesthesiology, 1997) [MEDLINE]
Obesity Does Not Appear to Impact the Normal Age-Related Decrease in Lung Function
Lung Function Gradually Decreases with Age in Healthy Individuals (Am J Respir Crit Care Med, 2001) [MEDLINE]
Maximal Inspiratory Pressure (Which is a Measure of Respiratory Muscle Strength Has Been Demonstrated to Decrease by About 0.8-2.7 cm H2O Per Year Between the Ages of 65 to 85, with Larger Declines Observed in Men (Am J Respir Crit Care Med, 1994) [MEDLINE]
However, There is No Clear Evidence that Obesity Increases or Reduces the Rate of Lung Function Decline with Age
Diagnosis
XXXXXXX
xxxx
Clinical Classification of Obesity
Body Mass Index (BMI)
BMI = Body Weight (in kg)/Height (in m²)
Clinical Classification of Obesity by Body Mass Index (BMI)
Overweight: BMI ≥25.0-29.9 kg/m²
Class I Obesity: BMI 30.0-34.9 kg/m²
Class II Obesity (Formerly Known as Morbid Obesity): BMI 35.0- 39.9 kg/m²
Class III Obesity (Formerly Known as Severe Obesity, Also Known as Extreme Obesity): BMI ≥40 kg/m²
Obesity/Overweight Increases the Risk of Hypertension in Children/Young Adults and Risk Increases with the Severity of Obesity (BMJ, 2012) [MEDLINE] (NEJM, 2015) [MEDLINE]
Longitudinal Investigation of Thromboembolism Etiology (LITE) Study Demonstrated that Obesity Increased the Risk of Venous Thromboembolism Using Age/Race/Sex-Adjusted Hazard Ratios for BMI (BMI <25 = 1.0, BMI 25-30 = 1.5, BMI 30-35 = 2.2, BMI 35-40 = 1.5, and BMI ≥40 = 2.7) (Arch Intern Med, 2002) [MEDLINE]
Meta-Analysis Indicated that Obesity (Risk 2.33), Hypertension (Risk 1.51), Diabetes Mellitus (Risk 1.42), Smoking (Risk 1.15), and Hypercholesterolemia (Risk 1.16) Increased the Risk of Venous Thromboembolism (Circulation, 2008) [MEDLINE]
Obesity Increased the Risk of Pulmonary Embolism (Relative Risk 2.03), But Decreased the Mortality of Pulmonary Embolism in Hospitalized Patients (Thromb Res, 2011) [MEDLINE]
Obesity is a Weak Risk Factor for Venous Thromboembolism (with Odds Ratio <2) (Eur Heart J, 2020) [MEDLINE]
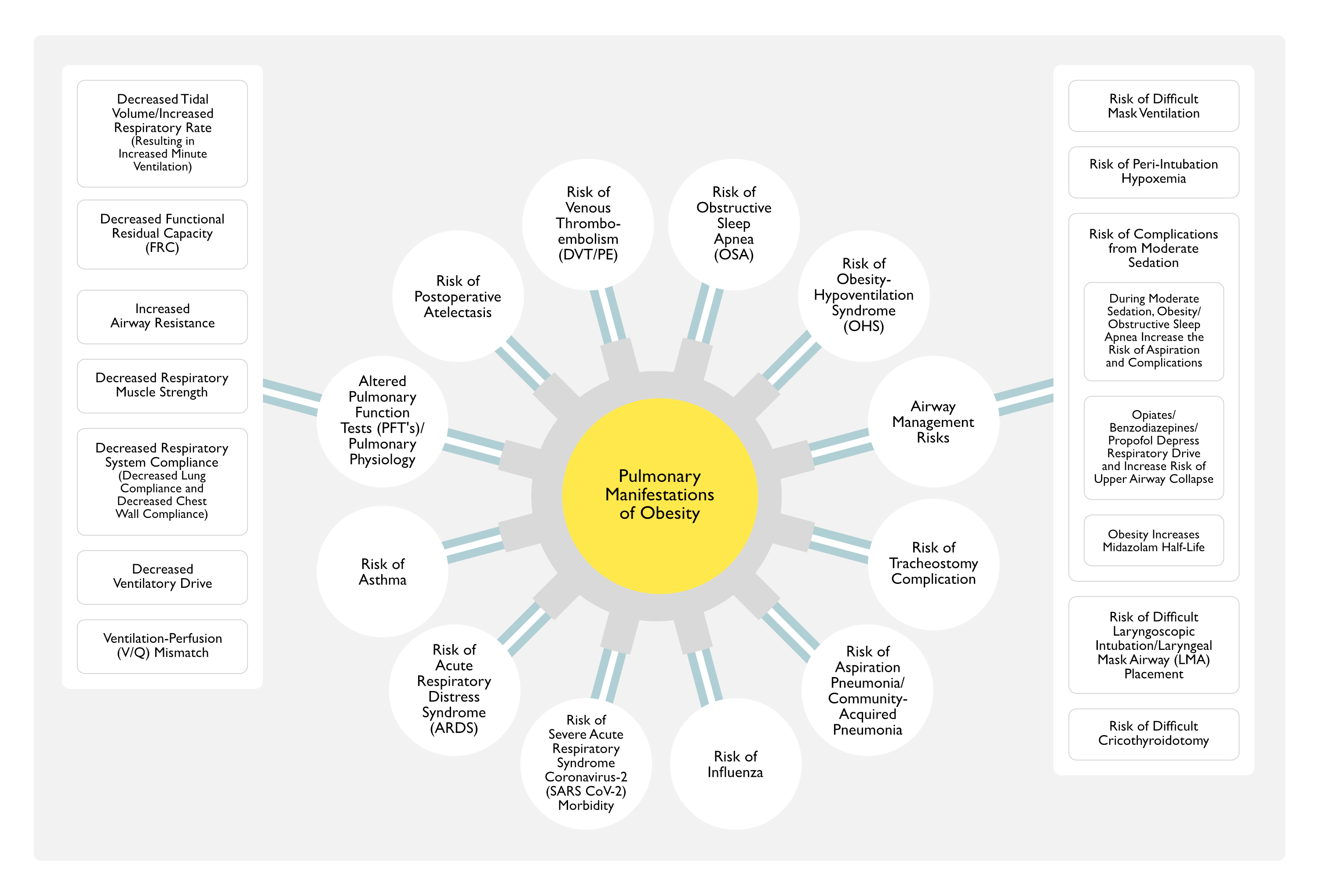
Since Obesity Increases the Risk of Bag-Valve-Mask (BVM) Ventilation, Extraglottic Device Ventilation, Laryngoscopy, Endotracheal Intubation, and Cricothyroidotomy/Tracheostomy, Airway Management in the Obese Patient Should Always Be Considered Potentially Difficult (Emerg Med Clin North Am, 2003) [MEDLINE]
Risk of Difficult Bag-Valve-Mask (BVM) Ventilation
Redundant Upper Airway Soft Tissue and Increased Body Mass Result in Increased Airway Resistance
Consequently, Higher Airway Pressures are Required to Ventilate the Obese Patient Effectively, Resulting in Difficulty Maintaining a Mask Seal
Predictors of Difficult Mask Ventilation: the presence of two of these factors had a 72% sensitivity and 73% specificity (Anesthesiology, 2000) [MEDLINE] and (Anesthesiology, 2006) [MEDLINE]
Age >55 y/o: age is associated with increased pharyngeal resistance to airflow (from choanae to epiglottis) in men, but not in women
BMI >26 kg/m2: obesity is associated with decreased posterior airway space behind the base of the tongue, impaired airway patency during sleep, and is a risk factor for OSA
Lack of Teeth
Presence of Beard
History of Snoring
Limited Mandibular Protrusion
Risk of Difficult Cricothyroidotomy (Anesth Analg, 2012) [MEDLINE]
Per the SMART Mnemonic, Obesity is a Risk Factor for Difficult Cricothyroidotomy
Obese Patients May Have Altered Upper Airway Anatomy, Resulting in a Poor Glottic View, Despite Optimal Laryngoscopic Technique
In Addition, the Presence of a Short, Thick Neck May Limit Mobility and Make it Difficult to Place the Patient in an Optimal Sniffing Position for Endotracheal Intubation
Increased Fat Deposition in Pharyngeal Tissues, Altering Obesity Upper Airway Anatomy, Predisposing to Pharyngeal Wall Collapse (and Complicating the Performance of Rapid Sequence Intubation) (Anesthesiol Clin North America, 2002) [MEDLINE]
Despite All of These Factors, the Association Between Class I/II Obesity and Difficult Laryngoscopy/Difficult Intubation is Unclear
Airway Study in Morbidly Obese Patients (Anesth Analg, 2002) [MEDLINE]
In 100 Morbidly Obese Patients, Neither Obesity Nor Body Mass Index (BMI) Predicted Problems with Endotracheal Intubation
However, a High Mallampati Score (≥3) and Large Neck Circumference May Increase the Potential for Difficult Laryngoscopy and Difficult Endotracheal Intubation
Emergency Department Study (Emerg Med Australas, 2004) [MEDLINE]
Difficult Intubation Rate was 15.5% in Obese Patients and 2.2% in Lean Patients
None of the Risk Factors for Difficult Intubation Described in the Lean Population was Satisfactory in the Obese Patients
There was a High Risk of Oxygen Desaturation in Obese Patients with Difficult Intubation
Danish Anesthesia Database Study (Anesthesiology, 2009) [MEDLINE]
High Body Mass Index (BMI) is a Weak (But Statistically Significant) Predictor of Difficult and Failed Intubation and May Be More Appropriate than Weight in Multivariate Models of Prediction of Difficult Endotracheal Intubation
Study Predicting Difficult Airways Using the Intubation Difficulty Scale (J Clin Anesth, 2009)[MEDLINE]
Difficult Intubation was More Prevalent Among Obese than Non-Obese Patients, But Intubation Duration and Lowest Oxygen Saturation Levels During Intubation were Not
Moreover, the Modified Mallampati Test was Found to Be a Moderately Good (60%) Predictor of Difficult Intubation in Obese Patients
Study of the Influence of Morbid Obesity on Difficult Intubation and Difficult Mask Ventilation (J Anesth, 2019) [MEDLINE]
Morbidly Obese Patients Did Not Have a Higher Incidence of Difficult Intubation, as Compared to Non-Morbidly Obese Patients
However, They Had a Significantly Higher Incidence of Difficult Mask Ventilation
Other Factors Which are Predictive of Both Difficult Mask Ventilation and Difficult Intubation Included Age >46 y/o, Male Sex, and Mallampati 3-4
Risk of Failed Video Laryngoscopic Intubation
Single-Center Observational Study of Video Laryngoscopy and Difficult Airway Characteristics in the ICU (Ann Am Thorac Soc, 2017) [MEDLINE]
Presence of Blood in the Airway, Airway Edema, Cervical Immobility, and Obesity are Associated with Higher Odds of First-Attempt Failure with Video Laryngoscopy
Risk of Complications from Laryngeal Mask Airway (LMA) Use
Obesity (with BMI >35 kg/m2) is a General Contraindication to Use of Laryngeal Mask Airway
When Used for Airway Management During Surgery, Obesity Increases the Amount of Time Required for Laryngeal Mask Airway Insertion (Cochrane Database Syst Rev, 2013) [MEDLINE]: probably not clinically important (although the failure rate of LMA’s is approximately 3-5%)
Risk of Complications from Moderate Sedation (see Sedation)
During Moderate Sedation, Obesity/Obstructive Sleep Apnea (OSA) Increase the Risk of Aspiration and Complications (Ann Emerg Med, 2007) [MEDLINE] (Anesthesiology, 2018) [MEDLINE] (Ann Emerg Med, 2019) [MEDLINE]
Obesity Increases Midazolam Half-Life (see Midazolam)
Due to Increased Volume of Distribution with No Difference in Clearance (Anesthesiology, 1984) [MEDLINE] (Clin Pharmacokinet, 2014) [MEDLINE]
Opiates/Benzodiazepines/Propofol Depress Respiratory Drive and Increase the Risk of Upper Airway Collapse (Anesthesiol Clin North America, 2002) [MEDLINE] (see Opiates, Benzodiazepines, and Propofol)
Risk of Peri-Intubation Hypoxemia (Anesthesiology, 1997) [MEDLINE]
Mechanisms of Peri-Intubation Hypoxemia in the Obese Patient
Abnormally Elevated Diaphragms
Decreased Capacity to Pre-Oxygenate Patient (Crit Care Clin, 2001) [MEDLINE] (Crit Care Clin, 2003) [MEDLINE]
Decreased Functional Residual Capacity (FRC), Due to Added Weight of Abdominal Fat on the Inferior Portions of the Lung (Especially in the Supine Position)
Increased Airway Resistance
Increased Carbon Dioxide Production
Increased Oxygen Consumption
Increased Work of Breathing (Due to Restrictive Lung/Chest Wall Physiology with Abnormal Chest Wall Elasticity and Decreased Caudal Diaphragmatic Excursion)
Limited Ventilatory Capacity (Especially in the Supine Position)
Alterations in Pulmonary Function Tests (PFT’s)/Pulmonary Physiology (see Pulmonary Function Tests) (Expert Rev Respir Med, 2018) [MEDLINE]
Decreased Tidal Volume/Increased Respiratory Rate, Resulting in Increased Minute Ventilation
Tidal Volume is Slightly Lower in Obesity (J Appl Physiol Respir Environ Exerc Physiol, 1983) [MEDLINE]
However, in Obesity, There is a Slight Increase in the Respiratory Rate (Which Compensates for the Shallow Breathing Pattern), Such that the Overall Minute Ventilation is Increased Significantly
Slightly Decreased FEV1 and FVC (with Normal FEV1/FVC Ratio)
However, in Patients with Extreme Obesity (BMI >62 kg/m2), Decreased FEV1, Decreased FEF25-75%, Decreased Maximal Voluntary Ventilation (MVV), and Normal DLCO are Observed (Am J Med Sci, 1999) [MEDLINE]
Abdominal Obesity Independent of BMI) Appears to Be a Risk Factor for Decreased FEV1/FVC Ratio (Am J Respir Crit Care Med, 2009) [MEDLINE]
Decreased Functional Residual Capacity (FRC)
Functional Residual Capacity is Defined as the Amount of Gas Left in the Lungs After a Normal Expiration
Functional Residual Capacity Acts as a Buffer by Preventing Rapid Changes in Alveolar Gas Tensions from Inspired Air
Functional Residual Capacity Serves as a Oxygen Reserve During Procedures, Such as Apneic Rapid Sequence Intubation (RSI)
Consequently, the Decreased Functional Residual Capacity in Obesity Limits that Oxygen Reserve During Apneic Rapid Sequence Intubation (RSI) and Leads to More Rapid Oxygen Desaturation
Since Obesity Adds the Weight of Abdominal Fat on the Inferior Portions of the Lung (and Similar to Any Process Which Increases Abdominal Size, Such as Pregnancy, Ascites, Abdominal Compartment Syndrome, etc), it Decreases the Functional Residual Capacity (FRC)
Obesity-Associated Decrease in Functional Residual Capacity (FRC) is Observed in Both Males and Females (Eur Respir J, 2005) [MEDLINE]
Reduction in Functional Residual Capacity (FRC) is Proportional to the Severity of Obesity (in the Absence of Asthma) (Chest, 2006) [MEDLINE]
Overweight: 10% decrease in functional residual capacity (FRC)
Mildly Obese: 22% decrease in functional residual capacity (FRC)
Severe Obesity: 33% decrease in functional residual capacity (FRC)
Normal Residual Volume (RV) (Chest, 2006) [MEDLINE]
Residual Volume (RV)/(Total Lung Capacity (TLC) Ratio is Also Normal-Slightly Increased (Chest, 2006) [MEDLINE]
RV/TLC Ratio is an Indicator of Gas Trapping
Decreased Expiratory Reserve Volume (ERV)
Decreased Strength/Endurance of Respiratory Muscles
In Patients with Mean BMI 39 +/- 6 kg/m2, Decreased Maximal Inspiratory Pressure (MIP) was Observed, as Compared to Control Patients (Respir Physiol Neurobiol, 2009) [MEDLINE]
Decreased Ventilatory Drive
Obesity May Impair Upper Airway Mechanical Function and Neuromuscular Strength, and Increase Oxygen Consumption, Which in Turn, Increase the Work of Breathing and Impair Ventilatory Drive (Respirology, 2012) [MEDLINE]
This Association is Higher in Males and Weaker in Females (Eur Respir J, 2005) [MEDLINE]
Decreased Respiratory System Compliance
Despite Conflicting Data, Several Studies Suggest that Both Chest Wall and Lung Compliance are Decreased in Obesity
Normal/Mildly Decreased Total Lung Capacity (TLC)
Several Studies Have Demonstrated Small Reductions in Total Lung Capacity (TLC) with Increasing Body Mass Index, But Total Lung Capacity (TLC) is Usually Well-Preserved Even in Patients with Severe Obesity
Ventilation-Perfusion (V/Q) Mismatch
In Obese Patients (with Severely Decreased Expiratory Reserve Volume) in the Upright Seated Position, Ventilation is Preferentially Distributed to the Poorly-Perfused Upper Lung Zones (J Clin Invest, 1967) [MEDLINE]
Severely Obese Patients (Who are Otherwise Healthy) Have Decreased Arterial pO2 and Increased Alveolar-Arterial pO2 Difference (Chest, 2015) [MEDLINE]
Obesity as an Important Risk Factor for the Development of Acute Respiratory Distress Syndrome (ARDS) (PLoS One, 2016) [MEDLINE]
Paradoxically, Acute Respiratory Distress Syndrome (ARDS) Outcomes are Improved in Obese Patients, as Compared to Patients with a Normal Body Mass Index
Postoperative Atelectasis May Persist for >24 hrs in Severely Obesity, in Contrast to Non-Obesity, Where Complete Resorption of Atelectasis is Observed in That Same Period of Time (Anesth Analg, 2002) [MEDLINE]
In Ambulatory Patients (NHANES), Plasma Leptin Levels Correlated Positively with Annual Risk of Respiratory Infection Independent of BMI (JCI Insight, 2016) [MEDLINE]
In patients with severe pneumonia resulting in ARDS (ARDSNet-ALVEOLI), plasma leptin levels were found to correlate positively with subsequent mortality
In Systematic Review/Meta-Analysis, Obesity was Found to Be Associated an Increased Risk of H1N1 Influenza (Obesity Reviews, 2011) [MEDLINE]
Severely obese H1N1 patients (body mass index ≥ 40 kg m(-2), n = 804) were as twice as likely to be admitted to ICU or die (odds ration: 2.01, 95% confidence interval: 1.29-3.14, P < 0.002) compared with H1N1 patients who were not severely obese
Individuals with Obesity are More Likely than normal-weight individuals to have respiratory complications during influenza season and are more likely to be hospitalized with influenza
Risk of Postoperative/Nosocomial/Respiratory/Skin and Soft Tissue Infection
Epidemiology
XXXX
Risk of Postoperative Complications
Epidemiology
There is No Evidence that High BMI is a Major Risk Factor for Postoperative Respiratory Complications in Otherwise Healthy Obese Patients
Postpneumonectomy Complications are Higher in Obese Patients (Eur J Cardiothorac Surg, 2011) [MEDLINE] (see Lung Resection)
Postoperative Atelectasis May Persist for >24 hrs in Severely Obesity, in Contrast to Non-Obesity, Where Complete Resorption of Atelectasis is Observed in That Same Period of Time (Anesth Analg, 2002) [MEDLINE]
Management
Postoperative Ventilation Can Be Optimized in Obesity by Placing the Patient in the Reverse Trendelenburg Position (Curr Opin Anaesthesiol 2007) [MEDLINE]
Risk of Tracheostomy Complication (see Tracheostomy)
Epidemiology
Morbid Obesity is Associated with Increased Risk of Life-Threatening Complications with Surgical Tracheostomy (Crit Care, 2007) [MEDLINE]
Obesity is Associated with Increased Risk of Post-Tracheostomy Tracheal Stenosis
Risk Factors for Post-Tracheostomy Tracheal Stenosis (Otolaryngol Head Neck Surg, 2018) [MEDLINE]
Endotracheal Tube Cuff Pressure ≥30 mm H2O
Failure to Create a Bjork Flap
Insertion of an Initial Tracheostomy Tube Size >6
Obesity
Percutaneous Tracheostomy Insertion Technique
Tracheostomy After 10 Days of Endotracheal Intubation
Other Manifestations
xxxx
Treatment
Bariatric Surgery
Epidemiology
Bariatric Surgery Use Has Increased from 1993 to 2016 (Ann Surg, 2020) [MEDLINE]
1,903,273 patients underwent bariatric surgery in the United States between 1993 and 2016
Mean age was 43.9 years (79.9% women, 70.9% white race, 70.7% commercial insurance)
These and other characteristics changed over time
Surgeries were exclusively open operations in 1993 (n = 8,631; gastric bypass and vertical banded gastroplasty, 49% each) and 98% laparoscopic (n = 162,969; 69.8% sleeve gastrectomy and 27.8% gastric bypass) in 2016
Complication and mortality rates peaked in 1998 (11.7% and 1%) and progressively decreased to 1.4% and 0.04% in 2016
Utilization increased from 0.07% in 1993 to 0.62% in 2004 and remained low at 0.5% in 2016
References
General
The effects of body weight on airway calibre. Eur Respir J 2005;25:896–901 [MEDLINE]
The association between obesity and asthma: interactions between systemic and airway inflammation. Am J Respir Crit Care Med 2008;178:469–475 [MEDLINE]
Physiology
Critical hemoglobin desaturation will occur before return to an unparalyzed state following 1 mg/kg intravenous succinylcholine . Anesthesiology. 1997 Oct;87(4):979-82. doi: 10.1097/00000542-199710000-00034 [MEDLINE]
Anesthetic management of morbidly obese patients. Semin Anesth. 2002; 21:46
Clinical
Effect of age, gender, and obesity on midazolam kinetics. Anesthesiology. 1984;61(1):27-35 [MEDLINE]
Relative risk analysis of factors associated with difficult intubation in obstetric anesthesia. Anesthesiology. 1992;77(1):67 [MEDLINE]
The airway: problems and predictions in 18,500 patients. Can J Anaesth. 1994;41(5 Pt 1):372 [MEDLINE]
Value of oropharyngeal Mallampati classification in predicting difficult laryngoscopy among obese patients. Eur J Anaesthesiol. 1998;15(3):330 [MEDLINE]
Prediction of difficult mask ventilation. Anesthesiology 2000;92:1229–1236 [MEDLINE]
Morbid obesity and tracheal intubation. Anesth Analg. 2002;94(3):732 [MEDLINE]
Cardiovascular risk factors and venous thromboembolism incidence: the longitudinal investigation of thromboembolism etiology. Arch Intern Med. 2002;162(10):1182 [MEDLINE]
Management of the difficult airway: alternative airway techniques and adjuncts. Emerg Med Clin North Am. 2003;21(2):259 [MEDLINE]
Difficult tracheal intubation is more common in obese than in lean patients. Anesth Analg. 2003;97(2):595 [MEDLINE]
Emergency management of the morbidly obese. Emerg Med Australas. 2004;16(4):309 [MEDLINE]
Incidence and predictors of difficult or impossible mask ventilation. Anesthesiology 2006;105:885–891 [MEDLINE]
Fasting and emergency department procedural sedation and analgesia: a consensus-based clinical practice advisory. Ann Emerg Med. 2007;49(4):454 [MEDLINE]
High body mass index is a weak predictor for difficult and failed tracheal intubation: a cohort study of 91,332 consecutive patients scheduled for direct laryngoscopy registered in the Danish Anesthesia Database. Anesthesiology. 2009;110(2):266 [MEDLINE]
Predicting difficult airways using the intubation difficulty scale: a study comparing obese and non-obese patients. J Clin Anesth. 2009;21(4):264 [MEDLINE]
The association between obesity and difficult prehospital tracheal intubation. Anesth Analg. 2011;112(5):1132 [MEDLINE]
Cardiovascular disease risk in healthy children and its association with body mass index: systematic review and meta-analysis. BMJ. 2012;345:e4759 [MEDLINE]
Accuracy of identification of the cricothyroid membrane in female subjects using palpation: an observational study. Anesth Analg. 2012 May;114(5):987-92 [MEDLINE]
Supraglottic airway devices versus tracheal intubation for airway management during general anaesthesia in obese patients. Cochrane Database Syst Rev. 2013 Sep 9;(9):CD010105. doi: 10.1002/14651858.CD010105.pub2 [MEDLINE]
Midazolam pharmacokinetics in morbidly obese patients following semi-simultaneous oral and intravenous administration: a comparison with healthy volunteers. Clin Pharmacokinet. 2014;53(10):931-941. doi:10.1007/s40262-014-0166-x [MEDLINE]
The use of VivaSight™single lumen endotracheal tube in morbidly obese patients undergoing laparoscopic sleeve gastrectomy. BMC Anesthesiol. 2014;14:31 [MEDLINE]
Cardiometabolic Risks and Severity of Obesity in Children and Young Adults. N Engl J Med. 2015;373(14):1307 [MEDLINE]
The impact of obesity on adult tracheostomy complication rate. Laryngoscope. 2015 Jan;125(1):105-10 [MEDLINE]
Difficult Airway Characteristics Associated with First-Attempt Failure at Intubation Using Video Laryngoscopy in the Intensive Care Unit. Ann Am Thorac Soc. 2017 Mar;14(3):368-375. doi: 10.1513/AnnalsATS.201606-472OC [MEDLINE]
Risk Factors for Posttracheostomy Tracheal Stenosis. Otolaryngol Head Neck Surg. 2018 Aug 21:194599818794456 [MEDLINE]
Practice Guidelines for Moderate Procedural Sedation and Analgesia 2018: A Report by the American Society of Anesthesiologists Task Force on Moderate Procedural Sedation and Analgesia, the American Association of Oral and Maxillofacial Surgeons, American College of Radiology, American Dental Association, American Society of Dentist Anesthesiologists, and Society of Interventional Radiology. Anesthesiology 2018; 128:437-79 [MEDLINE]
Unscheduled Procedural Sedation: A Multidisciplinary Consensus Practice Guideline. Ann Emerg Med. 2019;73(5):e51 [MEDLINE]
The influence of morbid obesity on difficult intubation and difficult mask ventilation. J Anesth. 2019;33(1):96 [MEDLINE]
Changes in Utilization of Bariatric Surgery in the United States From 1993 to 2016. Ann Surg 2020; 271:201 [MEDLINE]