Low or Low-Normal Plasma Renin Activity and Aldosterone Level
Metabolic Acidosis
Normal Renal Function
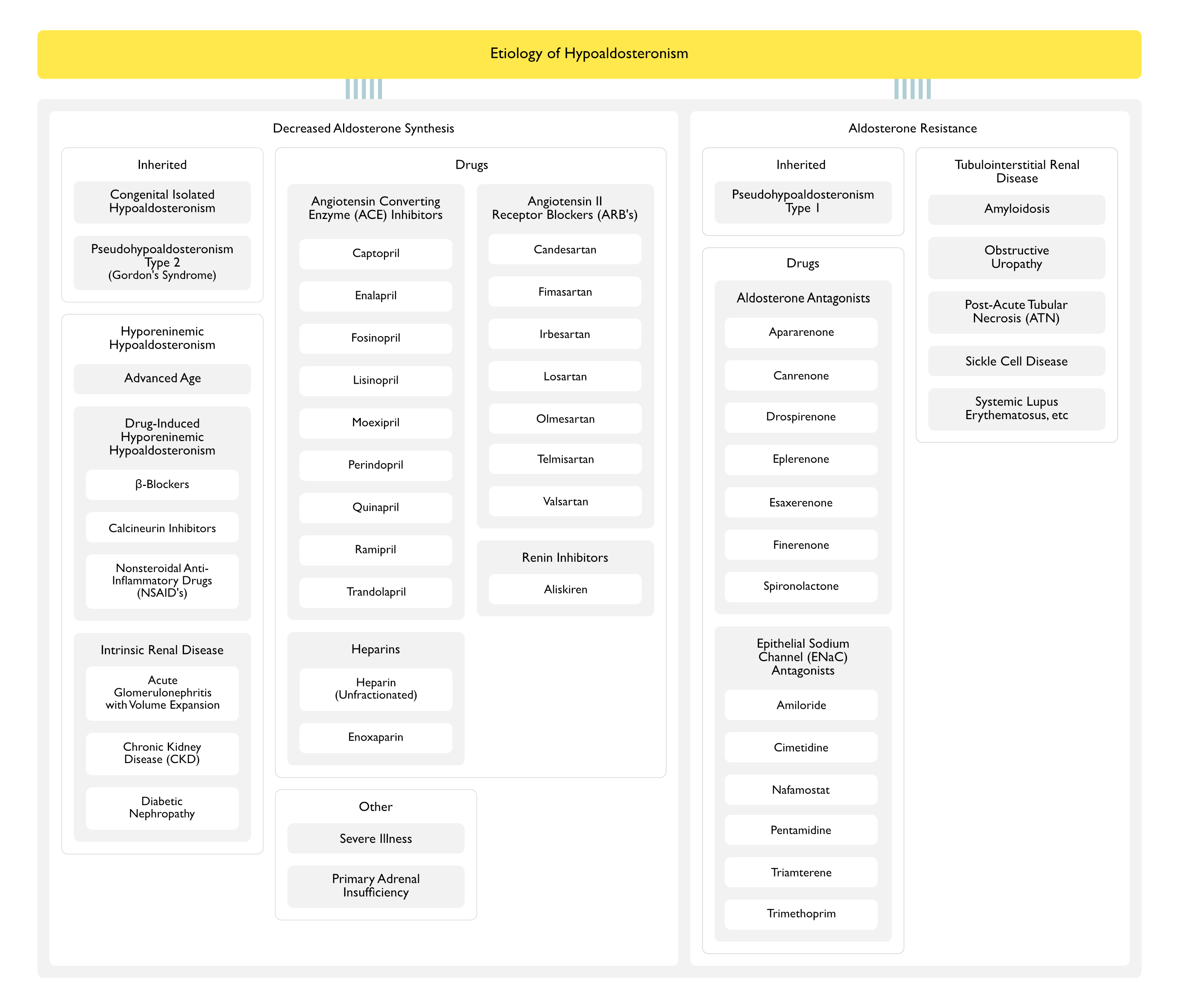
Hyporeninemic Hypoaldosteronism
General Comments
Hyporeninemic Hypoaldosteronism is Characterized by a Combination of Decreased Renin Release and an Intra-Adrenal Defect, Resulting in Decreased Systemic and Intra-Adrenal Angiotensin II Synthesis, Culminating in Decreased Aldosterone Secretion
The intra-adrenal defect may be related to the local renin-angiotensin system: this is supported by the fact that angiotensin II produced locally within the adrenal gland may stimulate the release of aldosterone
Many of these patients may also have decreased aldosterone responsiveness, since they require a higher mineralocorticoid dose for physiologic replacement
Physiology: due to decreased secretion of aldosterone and decreased responsiveness to aldosterone (likely due to decreased mineralocorticoid receptor expression)
Physiology: impair the conversion of angiotensin I to angiotensin II systemically (and possibly within the adrenal zona glomerulosa) -> since the normal stimulatory effect of hyperkalemia on aldosterone release may be mediated in part by the adrenal generation of angiotensin II, ACE inhibitors can decrease both angiotensin II-mediated and potassium-mediated aldosterone release
In contrast to ARB’s and renin inhibitors, ACE inhibitors increase renin levels
Physiology: heparins have a direct toxic effect on the adrenal zona glomerulosa cells (this may be mediated by a decrease in the number and affinity of adrenal angiotensin II receptors)
May occur even with the low doses of heparin used for deep venous thrombosis prophylaxis
Note: in contrast, pituitary disease does not result in hypoaldosteronism, since corticotropin (ACTH) does not play a major role in the regulation of aldosterone release
Aldosterone Resistance
Inherited Disorders
Pseudohypoaldosteronism Type 1
Subtypes
Autosomal Recessive Pseudohypoaldosteronism Type 1
Autosomal Dominant/Sporadic Pseudohypoaldosteronism Type 1
Physiology: resistance to action of aldosterone
Drugs
Aldosterone Antagonists: antagonize the activity of aldosterone on the collecting tubule cells by competition for the aldosterone receptor
Drospirenone (Yasmin, Yasminelle, Yaz, Beyaz, Ocella, Zarah, Angeliq) (see Drospirenone): synthetic hormone used in birth control pills
Epithelial Sodium Channel (ENaC) Antagonists (see Epithelial Sodium Channel Antagonists): these agents act to close sodium channels on the luminal membrane of cells in the collecting tubule (collecting tubule is the site of action of aldosterone)
Normal Physiologic Action of Aldosterone: aldosterone increases the number of open sodium channels on the luminal membrane of the principal cells in the cortical collecting tubule -> results in sodium reabsorption
The removal of sodium from the tubular fluid makes the lumen electronegative, creating an electrical gradient that favors the secretion of cellular potassium into the lumen through potassium channels on the luminal membrane
Diagnosis
Plasma Renin
Technique: should be performed after the administration of a loop diuretic or 3 hrs in the upright position (as these will increase renin and aldosterone release in normal individuals)
Conditions
Hyporeninemic Hypoaldosteronism: usually low
Primary Adrenal Insufficiency: high (due to volume depletion and/or hypotension)
Serum Aldosterone
Technique: should be performed after the administration of a loop diuretic or 3 hrs in the upright position (as these will increase renin and aldosterone release in normal individuals)
Conditions
Hyporeninemic Hypoaldosteronism: low
Primary Adrenal Insufficiency: low
Serum Cortisol
Technique: should be performed after the administration of a loop diuretic or 3 hrs in the upright position (as these will increase renin and aldosterone release in normal individuals)
Clinical: hyperkalemia is usually mild-moderate (except in the setting of other risk factors for hyperkalemia, such as ACE inhibitors, renal insufficiency, etc)
Mechanisms of Decreased Urinary Ammonium Excretion
Impaired Potassium Excretion with Potassium Entry into Cells -> Consequent Movement of Sodium and Hydrogen Ion into the Extracellular Fluid (to Maintain Electroneutrality) -> Alkalosis in Kidney Decreases Ammonium Synthesis in the Proximal Tubule
Hyperkalemia Decreases Medullary Cycling by Inhibiting Ammonium Reabsorption in Thick Ascending Limb: ammonium is normally reabsorbed into the medullary interstitium and then is re-secreted into the medullary collecting tubule
Potassium Competition for the Collecting Duct Na-NH4 Exchanger (i.e. the Basolateral Na-K-ATPase) Which Functions to Permit Uptake of Ammonium from the Interstitium and Allow Its Secretion into the Urine: potassium impairs the capacity of this pump to carry ammonium into the cell
Although aldosterone normally acts to increase sodium retention, hypoaldosteronism is not usually associated with significant sodium wasting (except in young children)
This is due to the compensatory action of other sodium-retaining stimuli (such as angiotensin II and norepinephrine)
In the absence of hypovolemia-induced stimulation of ADH release (with normal plasma cortisol, which is an inhibitor of ADH release), hyponatremia is uncommon
When hyponatremia is present, primary adrenal insufficiency should be suspected: in primary adrenal insufficiency, the concurrent lack of cortisol potently stimulates secretion of ADH secretion, resulting in water retention and hyponatremia
Treatment
Primary Adrenal Insufficiency
Fludrocortisone (Florinef) (see Fludrocortisone): dose of 0.05 to 0.2 mg/day
Fludrocortisone (Florinef) (see Fludrocortisone): dose of 0.2 to 1 mg/day
Dose Considerations: note that this replacement dose is higher than that required in primary adrenal insufficiency, as these patients have some degree of aldosterone resistance (due to their underlying renal disease)
Rationale: to correct the hyperkalemia
Contraindications: these are commonly present and may be exacerbated by fludrocortisone