Distinction Between Heart with Preserved Ejection Fraction (HFpEF), Heart Failure with Reduced Ejection Fraction (HFrEF), and High-Output Heart Failure (see Heart Failure)
Most Patients with Heart Failure Have Either Preserved or Reduced Ejection Fraction, While a Small Percentage Have a High Cardiac Output (CO) State with Decreased Systemic Vascular Resistance (SVR)
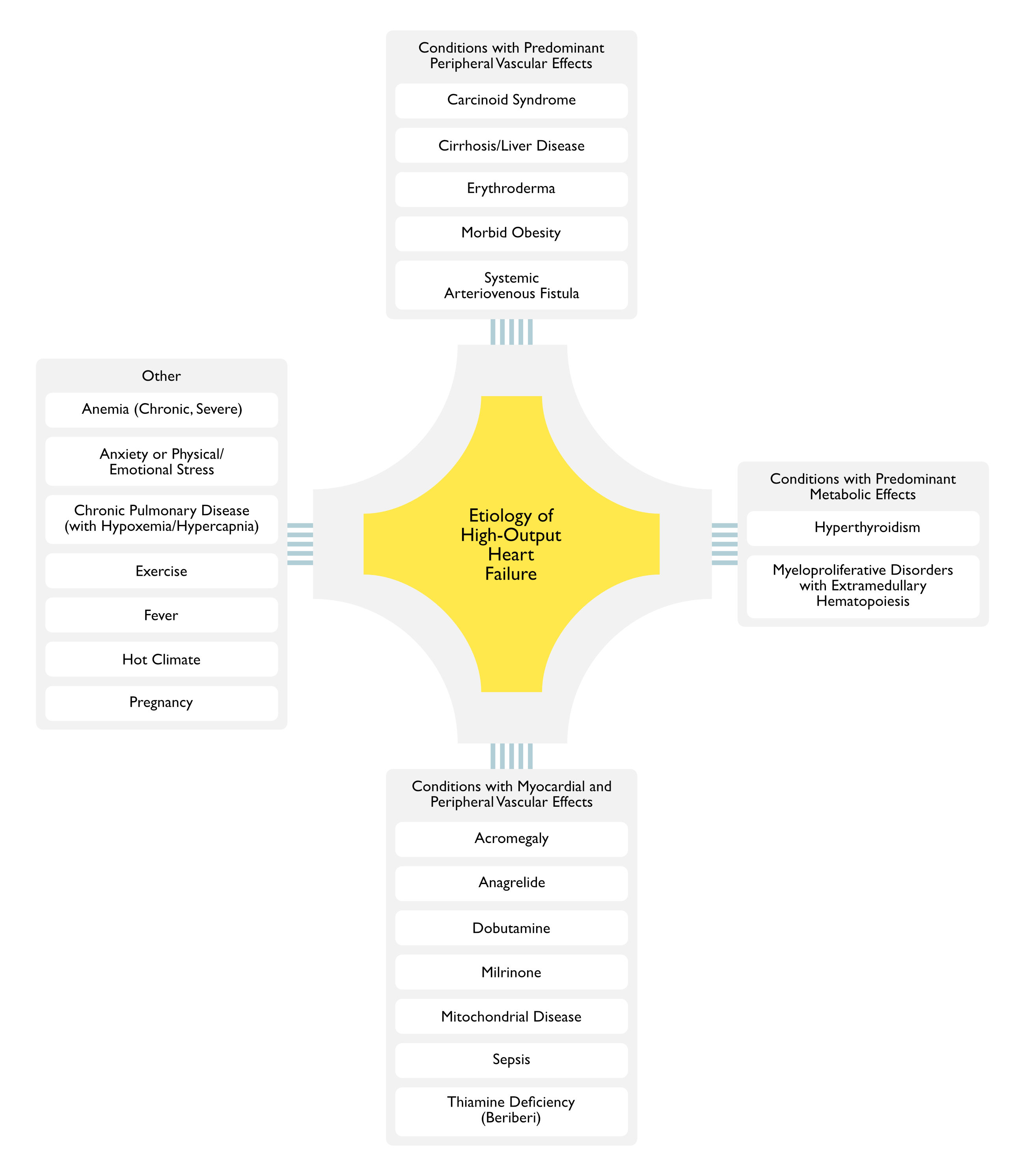
Etiologies of High-Output Heart Failure
Mayo Clinic Series of High-Output Heart Failure Patients (J Am Coll Cardiol, 2016) [MEDLINE]: n = 120
This Study Excluded a Number of Patient Groups with Other Etiologies of Heart Failure (Some of Which May Produce High-Output Heart Failure)
Many of the Following Conditions are Classified as Etiologies of “High Output Heart Failure”
However, this Term is a Misnomer, Since the Heart is Generally Normal (i.e. Capable of Generating a High Cardiac Output) and the Underlying Pathophysiology is Decreased Systemic Vascular Resistance, Resulting in Activation of Neurohormones Which Increase Renal Salt and Water Retention (and May Result in Hypotension)
Treatment with Vasodilators (Typically Used in Congestive Heart Failure) May Exacerbate the Heart Failure in These Conditions
Conditions with Predominant Peripheral Vascular Effects
Peripheral Vasodilation with Decreased Systemic Vascular Resistance
Clinical
High Cardiac Output/Low Systemic Vascular Resistance State Has Been Reported in Some Cases (Ann Intern Med, 1994) [MEDLINE] (Neth J Med, 2002) [MEDLINE]
However, Heart Failure with Right Heart Valvular Fibrosis is a More Common Cardiac Presentation
Progressive Systemic Vasodilation (Especially Splanchnic) with Development of Intrahepatic/Mesenteric Arteriovenous Shunts
Intrapulmonary Arteriovenous Shunts (i.e. Hepatopulmonary Syndrome) May Also Occur (Echocardiography, 2006) [MEDLINE] (see Hepatopulmonary Syndrome)
Clinical
Characteristically Produces a High Cardiac Output/Low Systemic Vascular Resistance State
High Output Heart Failure May Occur
Of All of the High Output Heart Failure Conditions, Cirrhosis Generally Produces the Lowest Arterial-Venous Oxygen Difference and the Lowest Systemic Vascular Resistance
Multiple Myeloma (see Multiple Myeloma): due to multiple minute arteriovenous fistulas in bony lesions
Paget Disease of the Bone (Osteitis Deformans) (see Paget Disease of Bone): due to multiple minute arteriovenous fistulas in bony lesions
Polyostotic Fibrous Dysplasia (McCune-Albright Syndrome): due to multiple minute arteriovenous fistulas in bony lesions
Trauma
Aortocaval Fistula
Bullet/Knife Wound (Particularly in the Thigh)
Physiology
High Pressure Arterial Blood is Shunted into a Low Pressure Vein, Shunting Past the Tissue Capillary Bed (and Decreasing the Systemic Vascular Resistance)
Subsequently, there is a Compensatory Increase in Stroke Volume, Cardiac Output, and Total Plasma Volume to Maintain Capillary Perfusion
High Cardiac Output/Low Systemic Vascular Resistance State May Occur (with High Output Heart Failure) (NEJM, 2001) [MEDLINE]
Sympatholytic Agents (β-Blockers) Can Partially Decrease Heart Rate and Cardiac Output, as Well as Partially Improve Pulse Pressure
Hyperthyroidism-Associated Hyperdynamic Right Ventricular Function (Which is Reversible with Treatment) Has Also Been Reported (Heart Lung Circ, 2017) [MEDLINE]
Hyperthyroidism-Associated Decreased Cardiac Output May Alternately Occur (Due to Tachycardia-Mediated Cardiomyopathy or Associated Cardiac Disease) (Heart, 2007) [MEDLINE]
Hyperthyroidism-Associated Reversible Right Ventricular Failure with Pulmonary Hypertension Has Also Been Reported (Am J Med Sci, 2018) [MEDLINE]
Myeloproliferative Disorders with Extramedullary Hematopoiesis
Due to Inflammatory Response (Involving TNF-α, IL-1β, IL-6, etc)
Clinical
Characteristically Produces a High Cardiac Output/Low Systemic Vascular Resistance State (Although Sepsis-Induced Myocardial Dysfunction May Alternately Occur)
High Output Heart Failure May Occur
Thiamine (Vitamin B1) Deficiency (Beriberi) (see Thiamine)
Epidemiology
Cases in Developed Countries are Generally Associated with One of the Following
Vasodilation May Occur Due to Direct Depression of Vasomotor Function (Am J Med, 1966) [MEDLINE]
Thiamine Deficiency Impairs Lactate and Pyruvate Utilization by the Myocardium (These Substrates are Important for Oxidation and Energy Production in the Myocardium)
Placental Blood Flow (Which May Function an Arteriovenous Shunt)
Physiology
High-Output Heart Failure is Characterized by Increased Cardiac Output and Decreased Systemic Vascular Resistance (Due to Peripheral Vasodilation or Arteriovenous Fistula/Shunt)
Increased Cardiac Output is Related to Both Lower Arterial Afterload (Decreased Systemic Vascular Resistance) and Higher Metabolic Rate (J Am Coll Cardiol, 2016) [MEDLINE]
The Observed Increased Cardiac Output is Higher than that Required to Meet Metabolic Demand
Ineffective Blood Volume and Blood Pressure Result in the Following
Neurohormonal Activation Results in the Following (J Am Coll Cardiol, 2016) [MEDLINE]
Increased Renovascular Resistance
Decreased Renal Blood Flow and Glomerular Filtration Rate
Retention of Salt and Water
Chronic Volume Overload May Result in Ventricular Enlargement, Remodeling, and Heart Failure
Activation of Neprilysin and the Sodium-Glucose Cotransporter 2 (SGLT2) Have Been Implicated in Interstitial Fibrosis and Subsequent Ventricular Remodeling in High-Output Heart Failure
Presence of Other Cardiovascular Disease
The Conditions Which Provoke High-Output Heart Failure are Rarely the Sole Etiology of Heart Failure
In Most Patients, the High Cardiac Output Provokes Heart Failure in the Setting of Decreased Ventricular Reserve (Systolic and/or Diastolic Dysfunction) from an Underlying Cardiac Problem
Therefore, the Presence of High-Output Heart Failure Should Prompt a Search for Another Underlying Cardiovascular Condition, Such as the Following
Failing Fontan Circulation (Extracardiac Conduit or Lateral Tunnel)
Of All Etiologies, Patients with Liver Disease Have the Lowest Arterial-Venous Oxygen Content Difference and the Lowest Systemic Vascular Resistance (SVR) (J Am Coll Cardiol, 2016) [MEDLINE]
Elevated Cardiac Filling Pressures (J Am Coll Cardiol, 2016) [MEDLINE]
Increased Oxygen Consumption (Due to Increased Metabolic Demand) with Increased Arterial-Venous Oxygen Difference is Present in Some Types of High-Output Heart Failure
Of All Etiologies, Patients with Liver Disease Have the Lowest Arterial-Venous Oxygen Content Difference and the Lowest Systemic Vascular Resistance (SVR) (J Am Coll Cardiol, 2016) [MEDLINE]
Of All Etiologies, Patients with Myeloproliferative Disorders Have the Highest Oxygen Consumption (Indexed to Weight) and Lowest Mixed Venous Oxygen Content (J Am Coll Cardiol, 2016) [MEDLINE]