

Definitions
General Definitions
- Acute Coronary Syndrome (ACS): defined as presence of suspicion of myocardial ischemia
- ST Elevation Myocardial Infarction (STEMI): characterized by an increase in cardiac biomarkers, indicative of myocyte injury
- Non-ST Elevation Myocardial Infarction (NSTEMI): characterized by an increase in cardiac biomarkers, indicative of myocyte injury
- Unstable Angina: myocardial ischemic symptoms suggestive of an acute coronary symptom without elevation in cardiac biomarkers with or without ECG changes indicative of myocardial ischemia
- ST-Segment and/or T-Wave changes are Often Persistent in NSTEMI: if they occur in unstable angina, they are usually transient
- However, the Presence of ST-Segment Changes Defines a Higher Risk Group, Regardless of Whether They Occur in Unstable Angina or NSTEMI (J Am Coll Cardiol, 1997) [MEDLINE]
Epidemiology
- CAD is the #1 cause of death in the US -> approximately 1 million deaths per year
- CAD comprises approximately 33-50% of all cardiovascular disease
- Cardiovascular disease (all related to atherosclerotic disease) includes CAD (MI, angina, CHF, and sudden death), cerebrovascular disease (stroke and TIA), peripheral vascular disease, and aortic aneurysm
- Presence of atherosclerotic disease in one location confers a high risk for astherosclerotic disease in another location
- Framingham Data
- Without CAD at Age 40: lifetime risk of CAD is 49% for men, 32% for women
- Without CAD At Age 70: lifetime risk of CAD is 35% for men, 24% for women
- National Health and Nutrition Examination Survey (NHANES): from 1960 -> 2000
- Obesity has increased 15% -> 30%
- Total Cholesterol >240 mg/dL: decreased 34% -> 17% (due to medications for cholesterol)
- HTN: decreased 31% -> 15% (due to antihypertensives)
- Smoking: decreased from 39% -> 26% (due to smoking cessation efforts)
Myocardial Infarction Associated with Non-Cardiac Procedures
- Epidemiology
- Perioperative MI is the Most Common Perioperative Vascular Complication in Major Non-Cardiac Surgery
- Perioperative MI is Associated with a Poor Prognosis
- Physiology: studies suggest that most of the MI’s diagnosed in this setting are due to a prolonged imbalance between myocardial oxygen supply and demand, with a background of CAD
- Clinical Features
- Most Patients Do Not Have Symptoms of Ischemia (POISE Study; Ann Intern Med, 2011) [MEDLINE]: monitoring of troponin levels in at-risk patients is required postoperatively to detect most MI events
- Prognosis
- Perioperative MI (Whether Symptomatic or Asymptomatic) is Strongly Associated with an Increased 30-Day Mortality Rate (POISE Study; Ann Intern Med, 2011) [MEDLINE]
Myocardial Infarction in the Intensive Care Unit (ICU)
- Epidemiology
- Troponin Elevations are Common in the ICU (Crit Care Med, 2008) [MEDLINE]
- Prognosis
- Acute MI Occurring in the ICU is Associated with a Worse Short-Term and Long-Term Mortality Rate, Regardless of the Underlying Disease State (Crit Care Med, 2008) [MEDLINE]
Reinfarction and Recurrent Myocardial Infarction
- Incident Myocardial Infarction: patient’s first MI
- Reinfarction: repeat myocardial infarction occurring within 28 days of an incident or recurrent MI
- Reinfarction Can Manifest as Recurrent ST-Segment Elevation or New Pathologic Q-Waves in Two Contiguous Leads: particularly when associated with symptoms lasting ≥20 min
- Re-elevation of the ST-segment can be seen as well with pending myocardial rupture
- ST-Segment Depression or LBBB Alone are Non-Specific Findings: should not be used to diagnose reinfarction
- Reinfarction Can Manifest as Recurrent ST-Segment Elevation or New Pathologic Q-Waves in Two Contiguous Leads: particularly when associated with symptoms lasting ≥20 min
- Recurrent Infarction: repeat myocardial infarction occurring >28 days from an incident MI
CAD Risk Assessment
Historical Elements
- Chest Pain/Angina
- Dyspnea
- CHF Symptoms
- Syncope
- Sudden Cardiac Death
Non-Modifiable Risk Factors
- Sex
- Males have a 3-fold increased risk of CAD, as compared to females
- Males have a 5-fold increased risk of CAD mortality, as compared to females -> however, half of this is attributable to an increased incidence of other cardiovascular risk factors in men vs women
- Risk in females increases afte menopause
- Age: increases risk
- Family History: significant independent risk factor for CAD
- Parental Positive History of CAD Before Age 55 in 1st Degree Male Relative or Before Age 65 in 1st Degree Female Relative: 1.4-1.8-fold increased risk of CAD
Modifiable Risk Factors for CAD (Interheart Study from 9 countries): these 9 modifiable factors account for approximately 90% of the population-attributable risk for acute MI
- Smoking
- 20% of American adults smoke
- Rates are lower among those >60 y/o (only 10 smoke) and higher in yound adults, males, those living below the poverty line, and in those without a high school education
- Smoking is the leading cause of preventable death: accounts for over 5 million deaths per year worldwide and 400k deaths per year in the US -> via cardiovascular disease, lung cancer, and COPD
- Confers 3-fold increased risk for CAD in men, 6-fold increased risk for CAD in women
- 20% of American adults smoke
- Hyperipidemia
- Increased total cholesterol, increased LDL, increased total cholesterol/HDL ratio, and hypertriglyceridemia all confer increased risk of CAD
- HTN
- Increased Systolic and Diastolic BP: both confer increased risk of CAD: systolic BP confers a higher risk in older patients
- Increased Pulse Pressure (a proxy for arterial stiffness): confers increased risk of CAD
- Past hx of HTN probably also confers increased risk of CAD
- Diabetes Mellitus
- Hyperinsulinemia, hyperglycemia, and insulin resistance all act to promoter atherosclerosis
- 2002-National Cholesterol Education Project: defined presence of DM as equivalent to having known CAD
- Abdominal Obesity: obesity alone is an independent risk factor for CAD
- Metabolic Syndrome: substantially increased risk for CAD
- Mild-Moderate Chronic Kidney Disease (CKD with GFR <60 ml/min): considered a CAD-equivalent by the National Kidney Foundation and ACC/AHA
- Psychosocial Factors: high-stress, depression, anger
- High Consumption of Calories + Saturated Fat + Cholestrol/Low Consumption of Fruits and Vegetables + Fiber
- ETOH Consumption: moderate ETOH consumption confers protection against CAD
- Lack of Regular Exercise
- Exercise increases HDL, decreases insulin resistance, has beneficial effects on coagulation, decreases BP, increases weight loss -> all combine to decrease the risk for CAD
NCEP-ATIII Panel Recommendations
- NCEP-AT III panel recommends screening of patients with 2 or more major risk factors:
- Smoking
- HTN with BP 140/90 or greater
- Low HDL (<40 mg/dL)
- Positive Family History of Premature CAD (Before Age 55 in 1st Degree Male Relative or Before Age 65 in 1st Degree Female Relative)
- Male Age 45 or greater/Female Age 55 ot greater
Web-Based CAD Risk Calculation
(Using Equation Derived from Framingham Data)
- Online Risk Calculator (determines 10-year risk of CAD: MI, coronary death, and angina): http://hp2010.nhlbihin.net/atpiii/calculator.asp?usertype=prof
- If HDL is 60 mg/dl or greater, remove one other risk factor from calculation
- From the NHANES database, this risk calculator will place approximately 82% of all patients into the low-risk group (<10% risk), 16% into the medium-risk group (10-20% risk), and 3% into the high-risk group (>20% risk)
- Those with a current high risk level (known CAD, DM, CKD, or familial hyperlipidemias) do not require additional screening
Etiology of Myocardial Ischemia/Infarction
Hypercoagulable State (see Hypercoagulable States, [[Hypercoagulable States]]
- Heparin-Induced Thrombocytopenia (HIT) (see Heparin-Induced Thrombocytopenia, [[Heparin-Induced Thrombocytopenia]])
- Physiology:
- Leukostasis (see Leukostasis, [[Leukostasis]])
- Physiology:
Toxin
- Cocaine Intoxication (see Cocaine, [[Cocaine]])
- Physiology:
- Methamphetamine Intoxication (see Methamphetamine, [[Methamphetamine]])
- Physiology:
Other
- Behcet’s Disease (see Behcet’s Disease, [[Behcets Disease]])
- Physiology: coronary artery vasculitis
- Churg-Strauss Syndrome (see Churg-Strauss Syndrome, [[Churg-Strauss Syndrome]])
- Physiology: coronary artery vasculitis
- Coronary Artery Bypass Graft (CABG) (see Coronary Artery Bypass Graft, [[Coronary Artery Bypass Graft]])
- Epidemiology
- Diagnosis: MRI studies suggest that most myocardial necrosis in this setting is not focal but is diffuse and localized in the subendocardium (J Am Coll Cardiol, 2005) [MEDLINE]
- Physiologic Mechanisms
- Coronary Artery Dissection
- Failure to Reperfuse Areas of Myocardium Not Served by Graftable Vessels
- Global/Regional Myocardial Ischemia Due to Inadequate Intraoperative Cardiac Protection
- Manipulation of the Heart
- Microvascular Events Related to Myocardial Reperfusion
- Myocardial Injury Due to Generation of Oxygen Free Radicals
- Suture Placement
- Coronary Artery Stent Thrombosis
- Physiology:
- Percutaneous Coronary Intervention (PCI) (see Percutaneous Coronary Intervention, [[Percutaneous Coronary Intervention]])
- Physiology Mechanisms: myocardial ischemia/injury with necrosis can occur via various mechanisms
- Balloon Inflation During PCI: causes transient myocardial ischemia with or without chest pain or ST-segment/T-wave changes
- Coronary Artery Dissection
- Disruption of Collateral Coronary Blood Flow
- Distal Coronary Artery Embolization: embolization of intracoronary thrombus may be not be preventable, despite anticoagulation, anti-platelet agents, aspiration, and protection devices
- Microvascular Plugging
- Occlusion of Major Coronary Artery or Side Branch
- Slow Flow or No-Reflow
- Physiology Mechanisms: myocardial ischemia/injury with necrosis can occur via various mechanisms
- Sinus of Valsalva Aneurysm (see Sinus of Valsalva Aneurysm, [[Sinus of Valsalva Aneurysm]]): due to coronary ostial obstruction with thrombosis
- Transcatheter Aortic Valve Replacement (TAVR) (see Transcatheter Aortic Valve Replacement, [[Transcatheter Aortic Valve Replacement]])
- Physiology
- Direct Trauma to Myocardium
- Regional Ischemia Due to Coronary Artery Obstruction or Embolization
- Physiology
- Transcatheter Mitral Valve Repair (Mitral Valve Clip) (see Transcatheter Mitral Valve Repair, [[Transcatheter Mitral Valve Repair]])
- Physiology
- Direct Trauma to Myocardium
- Regional Ischemia Due to Coronary Artery Obstruction or Embolization
- Physiology
Physiology
Normal Coronary Artery Anatomy and Physiology
Coronary Blood Supply
- Left Anterior Descending (LAD): anterior wall, anterior 2/3 of septum
- Left Circumflex (LCX): posterolateral wall
- Gives Rise to AV Nodal Artery in 10-15% of Persons
- Right Coronary Artery (RCA): inferolateral wall, posterior wall, posterior 1/3 of septum
- Gives Rise to AV Nodal Artery in 85-90% of Persons
- Note: lateral wall is often partially supplied by the LCX and RCA
- Dominance
- Right-Dominant Coronary Circulation: acute marginal and RV branches originating from RCA supply the RV
- Left-Dominant Coronary Circulation: LCX supplies the RV
- Codominant Coronary Circulation: RCA and LCX supply the RV
- Occasionally, the LAD may supply parts of the RV
Blood Supply to Cardiac Conduction System
- Blood Supply to the Sinoatrial (SA) Node
- Right Coronary Artery: 60% of patients
- Left Circumflex Artery: 40% of patients
- Blood Supply to the Atrioventricular (AV) Node
- Right Coronary Artery: 90% of patients
- Left Circumflex Artery: 10% of patients
- Blood Supply to the His Bundle
- Right Coronary Artery: main blood supply
- Septal Perforators of the Left Anterior Descending Coronary Artery: minor contribution
- Main/Proximal Left Bundle Branch
- Left Anterior Descending Artery: main blood supply
- Right Coronary Artery: collateral flow
- Left Circumflex Artery: collateral flow
- Left Anterior Fascicle
- Septal Perforators of the Left Anterior Descending Coronary Artery: main blood supply
- AV Nodal Artery: 50% of patients
- Left Posterior Fascicle
- Proximal Left Posterior Fascicle
- AV Nodal Artery: main blood supply
- Septal Perforators of the Left Anterior Descending Coronary Artery: in some cases
- Distal Left Posterior Fascicle
- Anterior and Posterior Septal Perforating Arteries (Dual Blood Supply)
- Proximal Left Posterior Fascicle
- Right Bundle Branch
- Septal Perforators of the Left Anterior Descending Artery: main blood supply
- Right Coronary Artery: some collateral flow (depending on dominance of the system)
- Left Circumflex Artery: some collateral flow (depending on dominance of the system)
Drivers of Myocardial Oxygen Consumption
- Heart Rate
- Increased Heart Rate Decreases Diastolic Filling Time and Increases Oxygen Demand
- Myocardial Contractility
Compensatory Increases in the Contractility of Non-ischemic/Non-Infarcted Myocardial Segments Can also Increase the Myocardial Oxygen Consumption - Myocardial Wall Stress
- Varies Directly as a Function of Chamber Pressure and Radius and Inversely as a Function of Wall Thickness: wall stress increases as the LV dilates and chamber pressure rises
Coronary Artery Obstruction
Background
- Coronary Artery Obstruction in STEMI and NSTEMI
- STEMI is Associated with Coronary Artery Obstruction in Almost 90% of Cases (NEJM, 1980) [MEDLINE]: based on this, the “open artery” strategy is fundamental
- NSTEMI is Associated with Coronary Artery Obstruction in <33% of Cases: consequently, strategies focused on maintaining arterial patency were developed (NEJM, 1986) [MEDLINE]
- Importantly, Both of These Studies Cited Above Demonstrated Significant Coronary Artery Disease in >97% of the Studied MI Patients (Circulation, 2015) [MEDLINE]
- Time Course of Coronary Artery Obstruction and Infarction: variable and depends on myocardial oxygen supply and demand
- Generally, in the Absence of Collateral Flow, Complete Coronary Artery Occlusion Results in Myocardial Infarction (Myocyte Necrosis) After Approximately 20 min
Myocardial Infarction with Non-Obstructed Coronary Arteries
- Approximately 10% of Acute MI Patients Have No Evidence of Coronary Artery Obstruction
- Systematic Review of Suspected Myocardial Infarction with Non-Obstructed Coronary Arteries (Circulation, 2015) [MEDLINE]
- MI without Coronary Artery Obstruction Occurs in 6% of All MI Cases
- No Clinical Features Allow Differentiation from MI with Obstructed Coronary Arteries
- MI with Non-Obstructed Coronary Arteries Has a Better 1-Year All-Cause Mortality Rate than MI with Obstructed Coronary Arteries
- Causes Which Should Be Considered in MI with Non-Obstructed Coronary Arteries
- Coronary Artery Vasospasm
- Structural Myocardial Dysfunction
- Dilated Cardiomyopathy
- Hypertrophic Cardiomyopathy
- Myocarditis (see Myocarditis, [[Myocarditis]])
- Takotsubo Cardiomyopathy (see Takotsubo Cardiomyopathy, [[Takotsubo Cardiomyopathy]])
- Thrombotic Disorders
- Factor V Leiden (see Factor V Leiden, [[Factor V Leiden]]): found in 12% of MI with non-obstructed coronary arteries
- Protein C Deficiency
- Protein S Deficiency
- Systematic Review of Suspected Myocardial Infarction with Non-Obstructed Coronary Arteries (Circulation, 2015) [MEDLINE]
Diagnosis
Electrocardiogram (EKG) (see Electrocardiogram, [[Electrocardiogram]])
Technique
- Right-Sided EKG Leads
- Purpose: used when an RV infarct is suspected
- ST elevation in V1-V3 is suggestive of RV infarct
- RV infarct may occur due to proximal RCA occlusion (often in conjunction with inferior or posterior MI, as RCA supplies these territories)
- Technique: V1 and V2 in usual position, V3-V6 on the right anterior chest wall in a mirror position as the V3-V6 leads in a normal left-sided ECG
- Interpretation: ST-segment elevation ≥0.05 mV (≥0.1 mV in males <30 y/o) in V3R and V4R
- Purpose: used when an RV infarct is suspected
- Posterior Leads: useful to detect left circumflex occlusion (which may exhibit a non-diagnostic EKG or ST-segment depression in V1-V3)
- V7: located at posterior axillary line
- V8: located at the left mid-scapular line
- V9: located at left paraspinal border
General Comments
- Comparison with Prior EKG: required to detect the timing of new EKG changes
- Serial EKG Assessment: required to detect dynamic changes
- If the Initial EKG is Non-Diagnostic and Patient Remains Asymptomatic, Serial EKG’s Should Be Performed q15-30 min During the Fist Hour (Class of Recommendation: I, Level of Evidence: C) (2014 AHA/ACC NSTEMI Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- EKG Changes Suggestive of Myocardial Ischemia or Infarction May Occur in the PR-Segment, the QRS Complex, the ST-Segment, or the T-Wave
- ST-Segment and T-Wave Changes: generally the earliest changes which are observed
- Hyperacute T-Waves (Increased T-Wave Amplitude) with Prominent Symmetrical T-Waves in at Least Two Contiguous Leads May Occur and Precede ST-Segment Elevation
- Prolonged ST-Segment Elevation (>20 min) Associated with Reciprocal ST-Segment Depression Usually Indicates Acute Coronary Occlusion (Which Results in Myocardial Injury with Necrosis)
- Pseudonormalization of Previously Inverted T-Waves May Indicate Myocardial Ischemia
- Q-Waves: may occur transiently during myocardial ischemia or rarely during acute MI with successful reperfusion
- Presence of LBBB: although interpretation of myocardial ischemia may be more difficult, the presence of concordant ST-segment elevation may be indicative of ischemia
- Presence of RBBB: in these patients, ST-segment abnormalities in V1-V3 are common, making it difficult to detect ischemia in these leads (however, new ST-segment elevation or Q-waves may be indicative of ischemia)
- ST-Segment and T-Wave Changes: generally the earliest changes which are observed
Electrocardiographic Criteria for Acute Myocardial Ischemia (ESC/ACCF/AHA/WHF; Circulation, 2012) [MEDLINE]
- New ST Elevation at the J Point in Two Contiguous Leads with the Following Cut Points
- Cut Point: ≥0.1 mV in all leads other than V2-V3
- Cut Point: ≥0.05 mV in V7-V9
- Cut Point (Males <40 y/o): ≥0.1 mV in V7-V9
- Cut Point (Males ≥40 y/o): ≥0.20 mV in V2-V3
- Cut Point (Males <40 y/o): ≥0.25 mV in V2-V3
- Cut Point (Females): ≥0.15 mV in V2-V3
- Cut Point: ≥0.1 mV in all leads other than V2-V3
- ST-Segment Depression and T-Wave Changes: either or both
- New Horizontal or Downsloping ST-Segment Depression ≥0.05 mV in Two Contiguous Leads
- Contiguous Leads Refers to Lead Groupings: anterior (V1-V6), inferior (II, II, AVF), lateral (I, AVL), free wall of RV (V3R, V4R), and infero-basal wall (V7-V9)
- ST-Segment Depression in V1-V3 May Indicate Posterior (Infero-Basal) Myocardial Ischemia (Especially When the Terminal T-Wave is Positive): however, this is non-specific
- T-Wave Inversion ≥0.1 mV in Two Contiguous Leads with Prominent R-Wave or R/S Ratio >1
- New Horizontal or Downsloping ST-Segment Depression ≥0.05 mV in Two Contiguous Leads
Conditions Which May Confound the EKG Diagnosis of Myocardial Ischemia
- Conditions Which May Result in a False-Positive EKG
- Acute Cholecystitis (see Acute Cholecystitis, [[Acute Cholecystitis]])
- Acute Pericarditis (see Acute Pericarditis, [[Acute Pericarditis]])
- Acute Pulmonary Embolism (PE) (see Acute Pulmonary Embolism, [[Acute Pulmonary Embolism]])
- Cardiomyopathy (see Congestive Heart Failure, [[Congestive Heart Failure]])
- Early Repolarization
- Hyperkalemia (see Hyperkalemia, [[Hyperkalemia]])
- J-Point Elevation Syndromes: Brugada syndrome
- Lead Transposition/Malposition of Precordial Leads
- Left Bundle Branch Block (LBBB) (see Left Bundle Branch Block, [[Left Bundle Branch Block]])
- Myocarditis (see Myocarditis, [[Myocarditis]])
- Persistent Juvenile Pattern
- Phenothiazines (see Phenothiazines, [[Phenothiazines]])
- Pre-Excitation
- Subarachnoid Hemorrhage (SAH) (see Subarachnoid Hemorrhage, [[Subarachnoid Hemorrhage]])
- Tricyclic Antidepressants (see Tricyclic Antidepressants, [[Tricyclic Antidepressants]])
- Conditions Which May Result in False-Negative EKG
- Left Bundle Branch Block (LBBB) (see Left Bundle Branch Block, [[Left Bundle Branch Block]])
- Prior MI with Q-Waves and/or Persistent ST-Segment Elevation
- Right Ventricular Pacing
Electrocardiographic Criteria for Prior Myocardial Infarction (ESC/ACCF/AHA/WHF; Circulation, 2012) [MEDLINE]
- Any Q-Wave in Leads V2-V3 ≥0.02 sec or QS Complex in Leads V2 and V3
- Q-Wave ≥0.03 sec and ≥0.1 mV or QRS Complex in Leads I, II, AVL, AVF, or V4-V6 in Any Two Contiguous Leads
- R-Wave ≥0.04 sec in V1-V2 and R/S ≥1 with a Concordant Positive T-Wave in the Absence of a Conduction Defect
Serum Troponin (see Serum Troponin, [[Serum Troponin]])
- Serial Troponin I/T Assessment is Indicated
- Clinical Efficacy
- Presence and Magnitude of Troponin Elevation is Useful for Short-Term and Long-Term Prognosis (Class of Recommendation: I, Level of Evidence: B) (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- Assessment of Serum Troponin Once on Day 3-4 May Be Reasonable in Acute MI as an Index of Infarct Size and Dynamics of Myocardial Necrosis (Class of Recommendation: IIb, Level of Evidence: B) (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
Serum Brain Natriuretic Peptide (BNP) (see Brain Natriuretic Peptide, [[Brain Natriuretic Peptide]])
- Clinical Efficacy
- Measurement of BNP May Be Useful to Provide Additional Prognostic Information (Class of Recommendation: IIb, Level of Evidence: B) (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
Echocardiogram (see Echocardiogram, [[Echocardiogram]])
- xxxx
Radionuclide Imaging
- Rationale: radionuclides allow viable mysocytes ot be visualized directly
- Radionuclide Tracers
- Thallium-201: SPECT
- Technetium-99m MIBI: SPECT
- Tetrofosmin: SPECT
- F-2-fluorodeoxyglucose (FDG): PET
- Rubidium-82: PET
Cardiac Computed Tomography (CT) (see Cardiac Computed Tomography, [[Cardiac Computed Tomography]])
- Indications
- xxxx
Cardiac Magnetic Resonance Imaging (MRI) (see Cardiac Magnetic Resonance Imaging, [[Cardiac Magnetic Resonance Imaging]])
- Indications
- xxxx
Cardiac Catheterization with Coronary Angiogram (see Cardiac Catheterization, [[Cardiac Catheterization]])
- TIMI Coronary Flow
- TIMI 0 Flow: complete occlusion
- TIMI 1 Flow: artery is reopened and fills but does not empty
- TIMI 2 Flow: slow flow
- TIMI 3 Flow: normal brisk flow
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- Takotsubo Cardiomyopathy Should be Considered in Patients Who Present with Apparent ACS and Non-Obstructive CAD on Coronary Angiogram (Class of Recommendation: I, Level of Evidence: C)
Clinical-Third Universal Definition of Acute Myocardial Infarction (ESC/ACCF/AHA/WHF; Circulation, 2012) [MEDLINE]
General Criteria for Myocardial Infarction
- Cardiac Death with Symptoms Suggestive of Myocardial Ischemia and Presumed New Ischemic EKG Changes or New LBBB: however, death occurred before cardiac biomarkers were obtained or before cardiac biomarker values would have been expected to increase
- Detection in Rise/Fall in Cardiac Biomarker (Troponin) with At Least One Value >99% of Upper Reference Limit and At Least One of the Following
- Development of Pathologic Q-Waves on EKG
- Identification of Intracoronary Thrombus by Angiography or Autopsy
- Imaging Evidence of a New Loss of Viable Myocardium or a New Regional Wall Motion Abnormality
- New or Presumed New Significant ST-Segment or T-Wave Changes or New Left Bundle Branch Block (LBBB)
- Symptoms of Myocardial Ischemia
Criteria for Percutaneous Coronary Intervention (PCI)-Related Myocardial Infarction
- Elevation of Cardiac Biomarker Values (Troponin) >5 x 99th Percentile Upper Reference Limit in Patient with Normal Baseline Values (<99th percentile Upper Reference Limit) or a Rise of Values >20% if the Baseline Values are Elevated but Stable or Falling
- Other Requirements
- Angiographic Evidence of Loss of Patency of a Major Coronary Artery or a Side Branch or Persistent Slow- or No-Flow or Embolization
- New Ischemic ECG Changes or New Left Bundle Branch Block (LBBB)
- Imaging Evidence of New Loss of Viable Myocardium or New Regional Wall Motion Abnormality
- Symptoms of Myocardial Ischemia
- Other Requirements
Criteria for Stent Thrombosis-Associated Myocardial Infarction
- Stent Thrombosis Detected by Coronary Angiography or Autopsy in the Setting of Myocardial Ischemia and with a Rise and/or Fall of Cardiac Biomarkers with at Least One Value Above the 99th Percentile of Upper Reference Limit
Criteria for Coronary Artery Bypass Graft Surgery (CABG)-Associated Myocardial Infarction
- Elevation of Cardiac Biomarker Values (Troponin) >10 x 99th percentile of Upper Reference Limit in Patient with Normal Baseline Troponin Values
- Other Requirements
- Angiographic Evidence of New Graft or Native Coronary Artery Occlusion
- Imaging Evidence of New Loss of Viable Myocardium or New Regional Wall Motion Abnormality
- New Pathologic Q Waves or New New Left Bundle Branch Block (LBBB)
- Other Requirements
Clinical Manifestations
General Comments
- Natural History of Coronary Artery Disease
- Course of CAD is variable: some patients remain stable, some patients develop unstable angina, some patients develop acute MI, and some patients develop sudden cardiac death
- The natural history may be related to the propensity of the patient’s coronary artery plaque to rupture
- ACS Triggers: which may precipitate plaque rupture
- Strenuous Activity
- Emotional Upset: related to sympathetic activation with increased BP, HR, and contractility
- However, ACS can occur at rest
- MI’s most often occur early in the AM: due to increased BP, increased blood viscosity, and highest diurnal epinephrine levels at this time
Cardiovascular Manifestations
Acute Myocardial Infarction (MI)
- Epidemiology
- xxxxx
- Clinical Criteria for Prior Acute Myocardial Infarction ((Third Universal Definition; ESC/ACCF/AHA/WHF; Circulation, 2012) [MEDLINE]
- Pathologic Q-Waves with/without Symptoms in the Absence of Non-Ischemic Causes
- Imaging Evidence of New Loss of Viable Myocardium that is Thinned and Fails to Contract in the Absence of Non-Ischemic Causes
- Pathologic Finding of a Prior MI
- Clinical Classification of Myocardial Infarction ((Third Universal Definition; ESC/ACCF/AHA/WHF; Circulation, 2012) [MEDLINE]
- Type 1-Spontaneous Myocardial Infarction: spontaneous myocardial infarction related to atherosclerotic plaque rupture, ulceration, fissuring, erosion, or dissection with resulting intraluminal thrombus in one or more coronary arteries leading to decreased myocardial blood flow or distal platelet emboli with ensuing myocardial necrosis (the patient may have underlying severe CAD, but on occasion, non-obstructive or no CAD)
- Type 2-Myocardial Infarction Secondary to an Ischemic Imbalance: myocardial injury with necrosis where a condition other than CAD contributes to an imbalance between myocardial oxygen supply and/or demand
- Anemia (see Anemia, [[Anemia]])
- Bradyarrhythmia
- Coronary Artery Endothelial Dysfunction
- Coronary Artery Vasospasm
- Coronary Embolism
- Hypertension with or without Left Ventricular Hypertrophy (see Hypertension, [[Hypertension]])
- Hypotension (see Hypotension, [[Hypotension]])
- Respiratory Failure (see Respiratory Failure, [[Respiratory Failure]])
- Tachyarrhythmia
- Type 3-Myocardial Infarction Resulting in Death When Biomarkers are Unavailable: cardiac death with symptoms suggestive of myocardial ischemia and presumed new ischemic EKG changes or new LBBB, but death occurred before blood samples could be obtained, before cardiac biomarker could rise, or where cardiac biomarkers were not collected
- Type 4a-Myocardial Infarction Related to Percutaneous Coronary Intervention (PCI): elevation of cardiac biomarker values (troponin) >5 x 99th percentile upper reference limit in patient with normal baseline values (<99th percentile upper reference limit) or a rise of values >20% if the baseline values are elevated but stable or falling
- Other Requirements
- Angiographic Evidence of Loss of Patency of a Major Coronary Artery or a Side Branch or Persistent Slow- or No-Flow or Embolization
- New Ischemic ECG Changes or New Left Bundle Branch Block (LBBB)
- Imaging Evidence of New Loss of Viable Myocardium or New Regional Wall Motion Abnormality
- Symptoms of Myocardial Ischemia
- Other Requirements
- Type 4b-Myocardial Infarction Related to Stent Thrombosis: stent thrombosis detected by coronary angiography or autopsy in the setting of myocardial ischemia and with a rise and/or fall of cardiac biomarkers with at least one value above the 99th percentile of upper reference limit
- Type 5-Myocardial Infarction Related to Coronary Artery Bypass Grafting (CABG): elevation of cardiac biomarker values (troponin) >10 x 99th percentile of upper reference limit in patient with normal baseline troponin values
- Other Requirements
- Angiographic Evidence of New Graft or Native Coronary Artery Occlusion
- Imaging Evidence of New Loss of Viable Myocardium or New Regional Wall Motion Abnormality
- New Pathologic Q Waves or New New Left Bundle Branch Block (LBBB)
- Other Requirements
- Clinical Features
- Chest Pain (see Chest Pain, [[Chest Pain]])
Acute Pericarditis (see Acute Pericarditis, [[Acute Pericarditis]])
- Epidemiology
- May Complicate the Course of Acute MI (NSTEMI/STEMI)
- Diagnosis
- xxxx
- Clinical
- Chest Pain (see Chest Pain, [[Chest Pain]])
Arrhythmia
- Epidemiology
- Ventricular Arrhythmias are Common Early After the Onset of STEMI
- Types
- Atrial Fibrillation (AF) (see Atrial Fibrillation, [[Atrial Fibrillation]])
- Atrial Flutter (see Atrial Flutter, [[Atrial Flutter]])
- Supraventricular Tachycardia (SVT) (see Supraventricular Tachycardia, [[Supraventricular Tachycardia]])
- Ventricular Fibrillation (VF) (see Ventricular Fibrillation, [[Ventricular Fibrillation]])
- Ventricular Tachycardia (VT) (see Ventricular Tachycardia, [[Ventricular Tachycardia]])
Cardiac Arrest (see Cardiac Arrest, [[Cardiac Arrest]])
- Epidemiology
- Almost 70% of the Coronary Heart Disease Deaths Annually in the US Occur Out-of-Hospital: usually presenting as cardiac arrest with sudden death
- Only 23% of Out-of-Hospital Arrests Have a Shockable Initial Rhythm (Usually VF): most neurologically-intact survivors come this group
- Clinical
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- Therapeutic hypothermia should be started as soon as possible in comatose patients with STEMI and out-of-hospital cardiac arrest caused by VF or pulseless VT, including patients who undergo primary PCI (Class of Recommendation: I, Level of Evidence: B)
- Immediate Coronary Angiogram and PCI When Indicated Should Be Performed in Resuscitated Out-of-Hospital Cardiac Arrest Patients Whose Initial EKG Demonstrates STEMI (Class of Recommendation: I, Level of Evidence: B)
Cardiogenic Shock (see Cardiogenic Shock, [[Cardiogenic Shock]])
- Epidemiology
- Cardiogenic Shock Occurs in 5-10% of ACS Cases
- Physiology
- xxxx
- Clinical
- Acute Kidney Injury (AKI) (see Acute Kidney Injury, [[Acute Kidney Injury]])
- Hypotension (see Hypotension, [[Hypotension]])
- Pulmonary Edema (see Pulmonary Edema, [[Pulmonary Edema]])
Conduction Defects
- Epidemiology
- Early Revascularization Has Decreased Incidence of Atrioventricular Blocks from 5.3% -> 3.7%
- Clinical
- Occlusion of Right Coronary Artery is the Most Common Source of Atrioventricular Block: proximal RCA occlusion has a high incidence of AV block (24% of cases) because there is involvement of not only the AV nodal artery, but also of the right superior descending artery (which originates from the proximal portion of the right coronary artery)
- Anterior Wall Myocardial Infarction with His-Purkinje (Infranodal) Block
- Inferior Wall Myocardial Infarction with AV Nodal Block: complete heart block occurs in <10% of cases
- Approximately 20% of Patients with Acute MI Develop an Atrioventricular Block
- First Degree Atrioventricular Block (see First Degree Atrioventricular Block, [[First Degree Atrioventricular Block]]): accounts for 8% of cases
- Second Degree Atrioventricular Block: accounts for 5% of cases
- Second Degree Atrioventricular Block-Mobitz Type I (see Second Degree Atrioventricular Block-Mobitz Type I, [[Second Degree Atrioventricular Block-Mobitz Type I]])
- Second Degree Atrioventricular Block-Mobitz Type II (see Second Degree Atrioventricular Block-Mobitz Type II, [[Second Degree Atrioventricular Block-Mobitz Type II]])
- Third Degree Atrioventricular Block (see Third Degree Atrioventricular Block, [[Third Degree Atrioventricular Block]]): accounts for 6% of cases
- Approximately 10-20% of Patients with Acute MI Develop an Intraventricular Conduction Disturbance (IVCD): includes bundle and fascicular blocks
- Left Bundle Branch Block (LBBB): common (accounts for approximately 33% of IVCD’s)
- Right Bundle Branch Block (RBBB) with Left Anterior Fascicle Block (LAHB): common (accounts for approximately 33% of IVCD’s)
- RBBB With or Without Left Posterior Fascicular Block: less commonly seen
- RBBB Alternating with LBBB: less commonly seen
- Isolated Left Anterior or Posterior Fascicle Block: least common
Left Ventricular Aneurysm (see Left Ventricular Aneurysm, [[Left Ventricular Aneurysm]])
- Epidemiology
- May Complicate the Course of Acute MI (NSTEMI/STEMI)
Left Ventricular Free Wall Rupture (see Left Ventricular Free Wall Rupture, [[Left Ventricular Free Wall Rupture]])
- Epidemiology
- May Complicate the Course of Acute MI (NSTEMI/STEMI)
- Clinical
Mitral Regurgitation (MR) (see Mitral Regurgitation, [[Mitral Regurgitation]])
- Epidemiology
- May Complicate the Course of Acute MI (NSTEMI/STEMI)
- Physiologic Mechanism
- Papillary Muscle Rupture
- Acute papillary muscle rupture affects the posteromedial papillary muscle more often than anterolateral papillary muscle because of its singular blood supply
- Post-Infarction LV Remodeling with Displacement of the Papillary Muscles, Leaflet Tethering, and Annular Dilatation
- Papillary Muscle Rupture
- Clinical
- Acute Mitral Regurgitation: pulmonary edema, shock, systolic murmur (although may not always be apreciated)
Pericardial Effusion (see Pericardial Effusion, [[Pericardial Effusion]])
- Epidemiology
- May Complicate the Course of Acute MI (NSTEMI/STEMI)
- Clinical
- Asymptomatic
Right Ventricular (RV) Infarction
- Epidemiology
- RV Infarct Complicates the Course of Approximately 33% of Patients with Inferior Wall MI
- Physiology: most often due to proximal RCA occlusion
- Diagnosis
- ST-Segment Elevation (1 mm) in V1 and V4R is the Most Sensitive EKG Pattern of RV Injury (Am Heart J, 1989) [MEDLINE]
- Classical Clinical Triad
- Clear Lung Fields
- Elevated Jugular Venous Pressure
- Hypotension (see Hypotension, [[Hypotension]])
Silent Myocardial Infarction
- Definition: silent myocardial infarction is defined as the presence of a new pathologic Q-wave in an asymptomatic patient detected during a routine EKG or detection of evidence of prior MI by cardiac imaging, which cannot be attributed to a coronary revascularization procedure
- Epidemiology
- Silent Q-wave MI Accounts for 9-37% of All Non-Fatal MI Events
- Silent Q-Wave MI is Associated with a Significantly Increased Mortality Risk
Ventricular Septal Rupture (see Ventricular Septal Rupture, [[Ventricular Septal Rupture]])
- Epidemiology
- Occurs Most Commonly in the First 24 hrs in STEMI Patients Treated with Thrombolytics
- Clinical
- Loud Systolic Murmur
- Cardiogenic Shock (see Cardiogenic Shock, [[Cardiogenic Shock]])
- Congestive Heart Failure (CHF) (see Congestive Heart Failure, [[Congestive Heart Failure]])
Acute MI
- Presentation
- NSTEMI (vessel is not typically 100% occluded)
- STEMI (vessel is typically 100% occluded): ST elevation or new LBBB on EKG
- Chest Pain
- Dyspnea
- Complications
- Post-Cardiac Injury Syndrome (see [[Post-Cardiac Injury Syndrome]])
Stunned Myocardium
- Prolonged reversible systolic dysfunction after acute MI (due to transient ischemia, but not necrosis)
- May improve gradually over days-weeks: includes resolution of myocyte calcium overload and free radical accumulation
Pulmonary Manifestations
Dyspnea (see Dyspnea, [[Dyspnea]])
- xxxx
Pulmonary Edema (see Pulmonary Edema, [[Pulmonary Edema]])
- xxx
Other Manifestations
- xxx
Treatment
Anti-Platelet Therapy
- Pharmacology: prevents further propagation of partially occlusive intracoronary thrombus and facilitates dissolution by endogenous mechanisms
- Agents
- Aspirin (see Acetylsalicylic Acid, [[Acetylsalicylic Acid]]): irreversible COX-1 inhibitor, preventing collagen-induced platelet activation and synthesis of thromboxane A2 (a platelet activator)
- P2Y12 Platelet Receptor Antagonists
- Cangrelor (Kengreal) (see Cangrelor, [[Cangrelor]])
- Clopidogrel (Plavix) (see Clopidogrel, [[Clopidogrel]]): thienopyridine P2Y12 platelet receptor antagonist which prevents ADP-induced platelet aggregation
- Prasugrel (Effient) (see Prasugrel, [[Prasugrel]])
- Ticagrelor (Brilinta) (see Ticagrelor, [[Ticagrelor]])
- Clinical Efficacy
- xxx
- Recommendations
- Aspirin is Recommended in All Patients with Coronary Artery Disease
Exercise
- Indicated to Manage Risk Factors
- Diabetes Mellitus (see Diabetes Mellitus, [[Diabetes Mellitus]])
- Hyperlipidemia (see Hyperlipidemia, [[Hyperlipidemia]])
- Hypertension (see Hypertension, [[Hypertension]])
Influenza Vaccination (see Influenza Virus, [[Influenza Virus]])
- Indicated
Inhibitors of the Renin-Angiotensin-Aldosterone System
- Pharmacology
- Aldosterone Antagonists
- Spironolactone (Aldactone) (see Spironolactone, [[Spironolactone]])
- Angiotensin Converting Enzyme (ACE) Inhibitors (see Angiotensin Converting Enzyme Inhibitors, [[Angiotensin Converting Enzyme Inhibitors]])
- Angiotensin II Receptor Blockers (ARB’s) (see Angiotensin II Receptor Blockers, [[Angiotensin II Receptor Blockers]])
- Aldosterone Antagonists
- Clinical Efficacy
- Controversial if ACE Inhibitors Decrease Exercise-Induced Myocardial Ischemia
- Recommendations
- xxx
Management of Hyperlipidemia (see Hyperlipidemia, [[Hyperlipidemia]])
- Statins lower LDL, stablize plaques, reduce inflammation (evidenced by decreased CRP levels), reverse endothelial dysfunction, and decrease thrombogenesis
- Lipid lowering decreases monocyte adherence to endothelium, reduces oxidative modification of LDL, and increase mobilization and differentiation of endothelial progenitors (which aid in preserving endothelial function)
- NCEP ATP III Guidelines (2004 Revision)
- High-Risk Patient (>20% 10-year risk, includes hx of CAD or cardiovascular disease, DM, CKD): LDL recommended to be <70
- Medium-Risk Patient (10-19% 10-year risk, includes metabolic syndrome): LDL recommended to be <100
- Low-Risk Patient (<10% 10-year risk): LDL recommended to be <160
- Trial Data
- Post-ACS: data support aggressive treatment to achieve LDL <70
- Stable CAD: data probably support treating high-risk group aggressively to achieve LDL <70
Smoking Cessation (see Tobacco, [[Tobacco]])
- Indicated
Weight Reduction
- Indicated
Treatment of Non-ST Elevation Myocardial Infarction (NSTEMI)/Acute Coronary Syndrome (ACS)
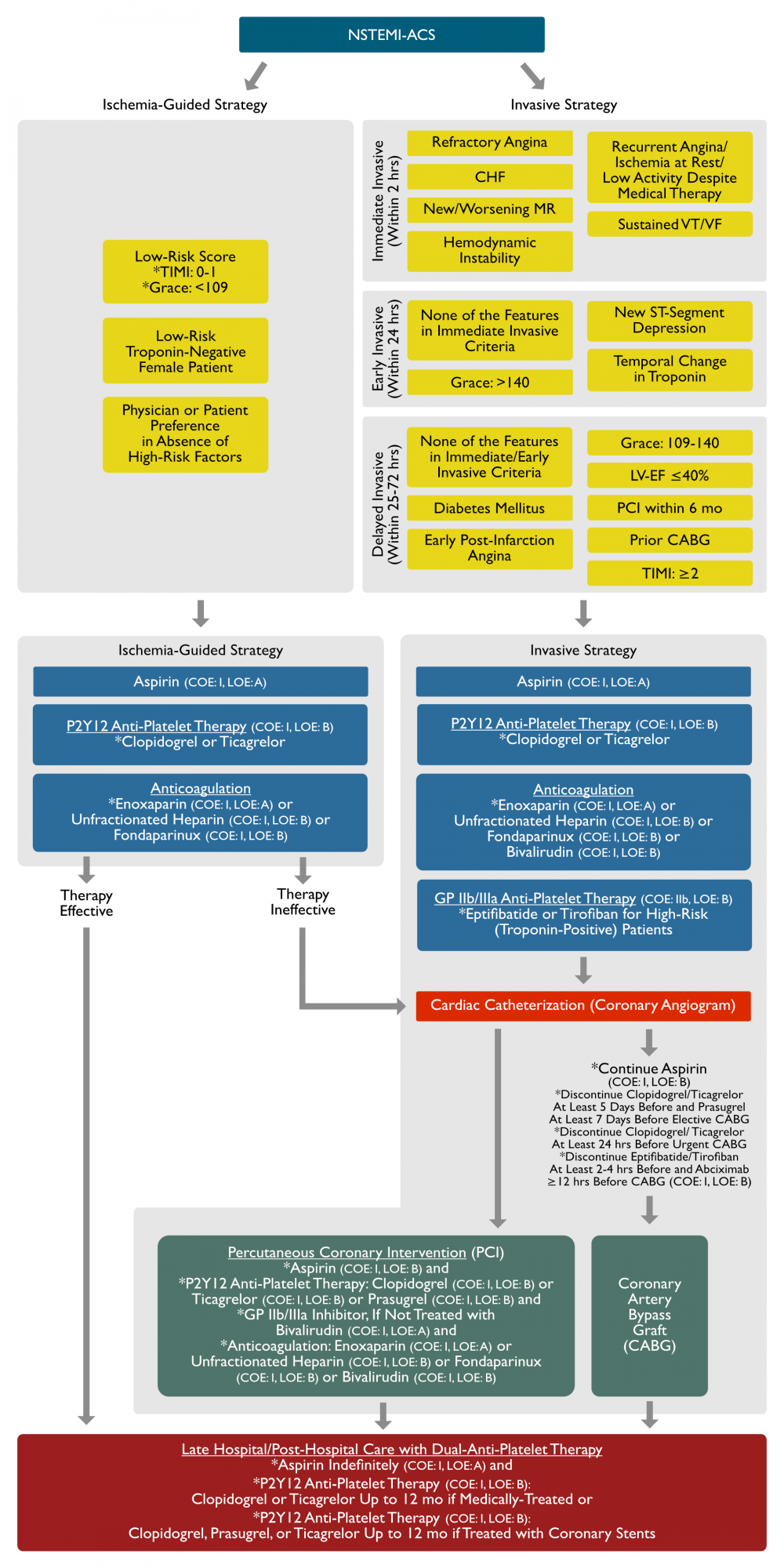
Flow Chart for NSTEMI-ACS Management (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
General Management Strategy
Risk Stratification Scoring Systems
- Thrombolysis in Myocardial Infarction (TIMI) Score: 7-Point scoring system which assesses risks of 30-day all-cause mortality, myocardial infarction, and recurrent myocardial ischemia -> patients with higher TIMI scores are more likely to benefit from an early invasive strategy
- Age ≥65 y/o
- Aspirin Use in the Last 7 Days
- At Least 3 Risk Factors for CAD: Hypertension, Hypercholesterolemia, Diabetes Mellitus, Family History of CAD, and Current Smoker
- Cardiac Biomarker Elevation
- History of Coronary Artery Disease (≥50% Stenosis)
- Severe Angina (≥2 Episodes in the Last 24 hrs)
- ST-Segment Changes (≥0.5 mm)
- Global Registry of Acute Cardiac Events (GRACE) Score
Clinical Features Determining the Management Strategy (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- Immediate Invasive Strategy (Within 2 hrs)
- Refractory Angina
- Congestive Heart Failure (CHF) (see Congestive Heart Failure, [[Congestive Heart Failure]])
- New/Worsening Mitral Regurgitation (see Mitral Regurgitation, [[Mitral Regurgitation]])
- Hemodynamic Instability
- Recurrent Angina or Ischemia at Rest or With Low-Level Activities Despite Intensive Medical Therapy
- Sustained Ventricular Tachycardia (VT)/Ventricular Fibrillation (VF) (see Ventricular Tachycardia, [[Ventricular Tachycardia]] or Ventricular Fibrillation, [[Ventricular Fibrillation]]))
- Early Invasive Strategy (Within 24 hrs)
- None of the Features in Immediate Invasive Strategy Criteria
- GRACE: >140
- New/Presumably New ST-Segment Depression
- Temporal Change in Troponin
- Delayed Invasive Strategy (Within 25-72 hrs)
- None of the Features in Immediate or Early Invasive Strategy Criteria
- Diabetes Mellitus (DM) (see Diabetes Mellitus, [[Diabetes Mellitus]])
- Early Post-Infarction Angina
- GRACE: 109-140
- Left Ventricular Dysfunction (LV EF ≤40%)
- Percutaneous Coronary Intervention (PCI) Within 6 mo (see Percutaneous Coronary Intervention, [[Percutaneous Coronary Intervention]])
- Prior Coronary Artery Bypass Graft (CABG) (see Coronary Artery Bypass Graft, [[Coronary Artery Bypass Graft]])
- TIMI: ≥2
- Ischemia-Guided Strategy
- Low-Risk Score
- TIMI: 0-1
- GRACE: <109
- Low-Risk Troponin-Negative Female Patient
- Patient or Physician Preference in the Absence of High Risk Features
- Low-Risk Score
Bed Rest
- Recommendations (ACCF/AHA Unstable Angina/NSTEMI Guidelines; Circulation, 2013) [MEDLINE]
- Bed/Chair Rest with Continuous EKG is Recommended During the Early Hospital Phase (Class of Recommendation: I, Level of Evidence: C)
Anticoagulation
- Pharmacology: prevents further propagation of partially occlusive intracoronary thrombus and facilitates dissolution by endogenous mechanisms
- Anticoagulation: in STEMI, heparin maintains coronary patency, once established
- Bivalirudin (Angiomax, Angiox) (see Bivalirudin , [[Bivalirudin ]])
- Enoxaparin (Lovenox) (see Enoxaparin, [[Enoxaparin]])
- Fondaparinux (Arixtra) (see Fondaparinux, [[Fondaparinux]])
- Unfractionated Heparin (see Heparin, [[Heparin]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Anticoagulation Should Be Added to Anti-Platelet Therapy for All Patients Irrespective of the Initial Management Strategy
- Enoxaparin (Lovenox) (Class of Evidence: I, Level of Evidence: A): for duration of hospitalization or until PCI is performed
- Unfractionated Heparin (Class of Evidence: I, Level of Evidence: B): for 48 hrs or until PCI is performed
- Bivalirudin (Class of Evidence: I, Level of Evidence: B)
- Fondaparinux (Class of Evidence: I, Level of Evidence: B)
- Anticoagulation Should Be Added to Anti-Platelet Therapy for All Patients Irrespective of the Initial Management Strategy
Anti-Platelet Therapy
- Pharmacology: prevents further propagation of partially occlusive intracoronary thrombus and facilitates dissolution by endogenous mechanisms
- Agents
- Aspirin (see Acetylsalicylic Acid, [[Acetylsalicylic Acid]]): irreversible COX-1 inhibitor, preventing collagen-induced platelet activation and synthesis of thromboxane A2 (a platelet activator)
- P2Y12 Platelet Receptor Antagonists
- Cangrelor (Kengreal) (see Cangrelor, [[Cangrelor]])
- Clopidogrel (Plavix) (see Clopidogrel, [[Clopidogrel]]): thienopyridine P2Y12 platelet receptor antagonist which prevents ADP-induced platelet aggregation
- Prasugrel (Effient) (see Prasugrel, [[Prasugrel]])
- Ticagrelor (Brilinta) (see Ticagrelor, [[Ticagrelor]])
- Platelet Glycoprotein IIb/IIIa Receptor Antagonists (see Platelet Glycoprotein IIb IIIa Receptor Antagonists, [[Platelet Glycoprotein IIb IIIa Receptor Antagonists]])
- Abciximab (ReoPro) (see Abciximab, [[Abciximab]])
- Eptifibatide (Integrilin) (see Eptifibatide, [[Eptifibatide]])
- Tirofiban (Aggrastat) (see Tirofiban, [[Tirofiban]])
- Clinical Efficacy
- Trial of Clopidogrel in Wide Range of Acute MI’s, NSTEMI and STEMI (Lancet, 2005) [MEDLINE]
- Clopidogrel Added to Aspirin and Other Standard Treatments Decreased Mortality and Other Vascular Events in the Hospital
- Trial of Clopidogrel in Wide Range of Acute MI’s, NSTEMI and STEMI (Lancet, 2005) [MEDLINE]
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Non-Enteric Coated Aspirin (162-325 mg) Should Be Administered as Soon as Possible After Presentation and Continued Indefinitely (Class of Evidence: I, Level of Evidence: A): with maintenance aspirin of 81-325 mg qday
- Clopidogrel Can Be Administered if Aspirin Cannot Be Tolerated (Class of Evidence: I, Level of Evidence: B)
- A P2Y12 Inhibitor (Clopidogrel or Ticagrelor) Should Be Administered in Addition to Aspirin for up to 12 mo to All Patients Who are Treated with Either an Early Invasive or Ischemia-Guided Strategy
- Clopidogrel (Plavix): 300-600-mg loading dose, then 75 mg qday (Class of Evidence: I, Level of Evidence: B)
- Ticagrelor (Brilinta): 180-mg loading dose, then 90 mg BID (Class of Evidence: I, Level of Evidence: B)
- It is Reasonable to Use Ticagrelor in Preference to Clopidogrel for P2Y12 Treatment in Patients with who Undergo an Early Invasive or Ischemia-Guided Strategy (Class of Evidence: IIa, Level of Evidence: B)
- In Patients Treated with an Early Invasive Strategy and Dual Anti-Platelet Therapy with Intermediate/High-Risk Fatures (Such as Positive Troponin), a Platelet llb/llla Inhibitor May Be Considered as Part of the Initial Anti-Platelet Therapy (Class of Evidence: IIb, Level of Evidence: B)
- Eptifibatide (Integrilin)
- Tirofiban (Aggrastat)
- In Patient with History of Stroke/TIA for Whom PCI is Planned, Prasugrel is Potentially Harmful (From 2013 Guidelines)
Beta Blockers (see β-Adrenergic Receptor Antagonists, [[β-Adrenergic Receptor Antagonists]])
- Pharmacology: mediated mostly via the blockade of the cardiac β1 adrenergic receptor
- Decease Sympathetic Drive to Myocardium
- Decrease Heart Rate
- Decrease Myocardial Contractility and Myocardial O2 Consumption
- Increase Rhythm Stability
- Decrease Progression from Unstable Angina to Acute MI
- Decrease the Mortality Rate in Acute MI
- Decease Sympathetic Drive to Myocardium
- Contraindications
- Bradycardia (see Sinus Bradycardia, [[Sinus Bradycardia]])
- Bronchospasm (see Obstructive Lung Disease, [[Obstructive Lung Disease]])
- Decompensated Congestive Heart Failure (CHF) (see Congestive Heart Failure, [[Congestive Heart Failure]])
- Hypotension (see Hypotension, [[Hypotension]])
- RV Infarction/Right Ventricular Dysfunction (see Congestive Heart Failure, [[Congestive Heart Failure]]): these patients are exquisitely preload-dependent
- Agents
- Bisoprolol (Concor, Zebeta) (see Bisoprolol, [[Bisoprolol]])
- Carvedilol (Coreg) (see Carvedilol, [[Carvedilol]])
- Metoprolol (Toprol) (see Metoprolol, [[Metoprolol]])
- Clinical Efficacy
- Meta-Analysis of Beta Blocker Use in Acute MI (NEJM, 1992) [MEDLINE]
- Beta Blockers Decreased the Mortality Rate by 28% at 1 week in ACS, with Most of the Benefit Occurring in the First 48 hrs
- Beta Blockers Demonstrated an 18% Reduction in Cumulative Rate of Reinfarction
- Beta Blockers Demonstrated an 15% Reduction in Cumulative Rate of Cardiac Arrest
- Systematic Review and Meta-Analysis of Beta Blockers in Acute MI (BMJ, 1999) [MEDLINE]
- Beta Blockers Decreased Long-Term Mortality Rate in Acute MI
- Meta-Analysis of Beta Blocker Use in Acute MI (NEJM, 1992) [MEDLINE]
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Oral Beta Blockers Should Be Used within the First 24 hrs in the Absence of Congestive Heart Failure, Low Cardiac Output State, Increased Risk for Cardiogenic Shock, or Other Contraindications to Beta Blocker Therapy (PR-Interval >0.24 sec, Second or Third-Degree Heart Block, or Active Asthma/Reactive Airway Disease) (Class of Recommendation: I, Level of Evidence: B)
- In Patients with Contraindications to Beta Blockers in the First 24 hrs, Eligibility Should Be Reassessed to Determine Their Subsequent Eligibility (Class of Recommendation: I, Level of Evidence: C)*
- In Patients with with Stabilized Heart Failure and Systolic Dysfunction, Beta Blocker Therapy Should Be Continued with One of the Drugs Proven to Decrease Mortality (Carvedilol, Metoprolol Succinate, Bisoprolol) (Class of Recommendation: I, Level of Evidence: C)
- It May Be Reasonable to Continue Beta Blocker Therapy in Patients with Normal LV Function (Class of Recommendation: IIa, Level of Evidence: C)
- Intravenous Beta Blockers are Reasonable in the Absence of Congestive Heart Failure, Low Cardiac Output State, Increased Risk for Cardiogenic Shock, or Other Contraindications to Beta Blocker Therapy (PR-Interval >0.24 sec, Second or Third-Degree Heart Block without a Pacemaker, or Active Asthma/Reactive Airway Disease) (From 2013 Guidelines)
- It May Be Harmful to Administer Intravenous Beta Blockers in Patients with Contraindications to Beta Blockade to Patients with Congestive Heart Failure, Low Cardiac Output State, Increased Risk for Cardiogenic Shock, or Other Contraindications to Beta Blocker Therapy (PR-Interval >0.24 sec, Second or Third-Degree Heart Block, or Active Asthma/Reactive Airway Disease) (Class of Recommendation: III, Level of Evidence: B)
- Oral Beta Blockers Should Be Used within the First 24 hrs in the Absence of Congestive Heart Failure, Low Cardiac Output State, Increased Risk for Cardiogenic Shock, or Other Contraindications to Beta Blocker Therapy (PR-Interval >0.24 sec, Second or Third-Degree Heart Block, or Active Asthma/Reactive Airway Disease) (Class of Recommendation: I, Level of Evidence: B)
Calcium Channel Blockers (see Calcium Channel Blockers, [[Calcium Channel Blockers]])
- Contraindicaions
- Pulmonary Edema/Severe Congestive Heart Failure (CHF) (see Congestive Heart Failure, [[Congestive Heart Failure]]): for non-dihydropyridine calcium channel blockers (which have negative inotropic effects)
- Pharmacology
- Decreased Heart Rate
- Decreased Myocardial Contractility
- Vasodilation
- Agents
- Dihydropyridine Calcium Channel Blockers (Amlodipine, Nifedipine): predominately produce vasodilation, resulting in a decrease in blood pressure and reflex tachycardia
- Non-Sustained Release Nifedipine Should Be Avoided in ACS (in the Absence of Beta Blockers) for this Reason
- Non-Dihydropyridine Calcium Channel Blockers (Diltiazem, Verapamil): predominately decrease heart rate, the rate of atrioventricular conduction, blood pressure, and myocardial contractility
- Dihydropyridine Calcium Channel Blockers (Amlodipine, Nifedipine): predominately produce vasodilation, resulting in a decrease in blood pressure and reflex tachycardia
- Clinical Efficacy
- Review of Calcium Channel Blockers in Acute MI (BMJ, 1989) [MEDLINE]
- Calcium Channel Blockers Did Not Impact Infarct Size, Rate of Reinfarction, or Mortality Rate
- Review of Calcium Channel Blockers in Acute MI (BMJ, 1989) [MEDLINE]
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Non-Dihydropyridine Calcium Channel Blockers (Diltiazem, Verapamil) Can Be Used for Ongoing Myocardial Ischemia, if Beta Blockers are Contraindicated and in the Absence of LV Dysfunction, Increased Risk for Cardiogenic Shock, PR-Interval >0.24 sec, or Second/Third-Degree Atrioventricular Block without a Pacemaker (Class of Recommendation: I, Level of Evidence: B)
- Oral Non-Dihydropyridine Calcium Channel Blockers (Diltiazem, Verapamil) Can Be Used in Addition to Beta Blockers and Nitrates for Recurrent Myocardial Ischemia (Class of Recommendation: I, Level of Evidence: C)
- Extended Release Non-Dihydropyridine Calcium Channel Blockers (Diltiazem, Verapamil) are Recommended for Ischemic Symptoms When Beta Blockers are Unsuccessful, Contraindicated, or Cause Unacceptable Side Effects (Class of Recommendation: I, Level of Evidence: C)
- Long-Acting Calcium Channel Blockers and Nitrates are Recommended in Patients with Coronary Artery Vasospasm (Class of Recommendation: I, Level of Evidence: C)
- Immediate Release Dihydropyridine (Nifedipine) Calcium Channel Blockers Should Not Be Used in Unstable Angina/NSTEMI in the Absence of a Beta Blocker (Class of Recommendation: III, Level of Evidence: B)
Cardiac Catheterization with Coronary Angiography (see Cardiac Catheterization, [[Cardiac Catheterization]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- Takotsubo Cardiomyopathy Should be Considered in Patients Who Present with Apparent ACS and Non-Obstructive CAD on Coronary Angiogram (Class of Recommendation: I, Level of Evidence: C)
Coronary Artery Bypass Graft (CABG) (see Coronary Artery Bypass Graft, [[Coronary Artery Bypass Graft]])
- Indications
- Significant Left Main Disease (>50%) (Class of Recommendation: I)
- Three-Vessel CAD, Especially in Patients with LV-EF <50%) (Class of Recommendation: I)
- Two-Vessel CAD with Significant Proximal LAD Stenosis and Either LV-EF <50% or Ischemia on Stress Testing (Class of Recommendation: I)
- Poor or No Options for PCI in Patient with Ongoing Ischemia Refractory to Medical Therapy (Class of Recommendation: I)
Inhibitors of the Renin-Angiotensin-Aldosterone System
- Rationale: activation of the renin-angiotensin-aldosterone system by a number of factors is known to occur in the setting of ACS -> results in increased production of angiotensin II with increased systematic vascular resistance, myocardial workload, and myocardial oxygen consumption
- Inhibitors of the Renin-Angiotensin-Aldosterone System Also Function to Inhibit the Downstream Detrimental Pathways Which Lead to Long-Term Fibrosis and Myocardial/Vascular Remodeling
- Pharmacology
- Aldosterone Antagonists
- Spironolactone (Aldactone) (see Spironolactone, [[Spironolactone]])
- Angiotensin Converting Enzyme (ACE) Inhibitors (see Angiotensin Converting Enzyme Inhibitors, [[Angiotensin Converting Enzyme Inhibitors]]): prevent adverse ventricular remodeling (ie: detrimental increase in ventricular size, which increases ventricular wall stress, impairs systolic contractile function, and increases likelihood of aneurysm formation, CHF, and ventricular arrhythmias)
- Remodeling is Reduced by Decreasing Infarct Size (by Repercussion) and Afterload Reduction (Due to Inhibition of the Renin-Angiotensin System)
- Angiotensin II Receptor Blockers (ARB’s) (see Angiotensin II Receptor Blockers, [[Angiotensin II Receptor Blockers]])
- Aldosterone Antagonists
- Clinical Efficacy
- GISSI-3 Trial of Transdermal Glyceryl Trinitrate and Lisinopril in Acute MI (Lancet, 1994) [MEDLINE]
- Lisinopril Decreased the 6-Week Mortality Rate and the Composite Endpoint of Mortality and Severe LV Dysfunction
- GISSI-3 Trial of Transdermal Glyceryl Trinitrate and Lisinopril in Acute MI (Lancet, 1994) [MEDLINE]
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- Aldosterone Antagonists Should Be Administered In Addition to Beta Blocker and ACE Inhibitor with an LV EF ≤40%, Heart Failure, or Diabetes Mellitus, in the Absence of Significant Renal Dysfunction (Cr >2.5 mg/dL in males, Cr >2.0 mg/dL in females) or Hyperkalemia (Class of Evidence: I, Level of Evidence: A)
- Oral ACE Inhibitors Should Be Started and Continued Indefinitely in Patients with LV EF ≤40%, Hypertension, Diabetes Mellitus, or Stable Chronic Kidney Disease, in the Absence of Hypotension (SBP <100 mm Hg or <30 mm Hg Below Baseline SBP) (Class of Evidence: I, Level of Evidence: A)
- Oral ACE Inhibitors May Be Reasonable in All Other Patients with Cardiac or Other Vascular Disease (Class of Evidence: IIb, Level of Evidence: B)
- Intravenous ACE Inhibitors Should Not Be Used in the First 24 hrs, Due the Risk of Hypotension (From 2013 Guidelines)
- ARB’s Should Be Administered to Patients Who are Intolerant of ACE Inhibitors with Heart Failure or LV EF ≤40%, in the Absence of Hypotension (SBP <100 mm Hg or <30 mm Hg Below Baseline SBP) (Class of Evidence: I, Level of Evidence: A)
- ARB’s are Reasonable in Patients with Cardiac or Other Vascular Disease Who are Intolerant of ACE Inhibitors (Class of Evidence: IIa, Level of Evidence: B)
Intra-Aortic Balloon Pump (IABP (see Intra-Aortic Balloon Pump, [[Intra-Aortic Balloon Pump]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- IABP is Reasonable for Severe Ongoing Myocardial Ischemia Despite Intensive Medical Therapy, for Hemodynamic Instability Before/After Coronary Angiography, or for Mechanical Complications of MI (From 2013 Guidelines)
Management of Anemia (see Anemia, [[Anemia]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- A Strategy of Routine Blood Transfusion in Hemodynamically Stable Patients with NSTEMI-ACS and Hemoglobin Levels Greater than 8 g/dL is Not Recommended (Class of Recommendation: III, Level of Evidence: B)
Management of Blood Glucose
- xxxx
Morphine Sulfate (see Morphine, [[Morphine]])
- Pharmacology
- Anxiolytic
- Decreases Work of Breathing
- Favorable Effect on Ventricular Loading
- Clinical Efficacy
- CRUSADE Trial in Acute Coronary Syndrome (Am Heart J, 2005) [MEDLINE]
- Use of Morphine (Alone or with Nitroglycerin) in NSTEMI/ACS was Associated with a Higher Mortality Rate
- CRUSADE Trial in Acute Coronary Syndrome (Am Heart J, 2005) [MEDLINE]
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014) [MEDLINE]
- Intravenous Morphine is Reasonable for for Uncontrolled Ischemic Chest Discomfort Which Occurs Despite Maximal Anti-Ischemic Medications (Class of Recommendation: IIb, Level of Evidence: B)
Nitrates (see Nitrites and Nitrates, [[Nitrites and Nitrates]])
- Indications
- Chest Pain (see Chest Pain, [[Chest Pain]])
- Hypertension (see Hypertension, [[Hypertension]])
- Congestive Heart Failure (CHF) (see Congestive Heart Failure, [[Congestive Heart Failure]])
- Contraindications
- RV Infarction/Right Ventricular Dysfunction (see Congestive Heart Failure, [[Congestive Heart Failure]]): these patients are exquisitely preload-dependent
- Use of Phosphodiesterase Type 5 Inhibitors (PDE5 Inhibitors) (see Phosphodiesterase Type 5 Inhibitors, [[Phosphodiesterase Type 5 Inhibitors]]): may result in profound hypotension
- Sildenafil (Viagra) (see Sildenafil, [[Sildenafil]])
- Pharmacology
- Normal and Diseased Coronary Artery Vasodilation: improves anterograde and collateral coronary blood flow
- Prevention of Coronary Artery Vasospasm: improves coronary blood flow
- Provides Symptomatic Relief of Chest Pain
- Systemic Vasodilation, Resulting in Decreased Blood Pressure and Decreased Afterload
- Venodilation with Decreased Preload and Decreased LV End-Diastolic Volume, Resulting in Decreased Myocardial Oxygen Consumption
- No Impact on Myocardial Infarction Rate or Mortality Rate
- Administration
- PO: nitro-BID (see Nitroglycerin, [[Nitroglycerin]])
- SL: nitroglycerin sublingual (see Nitroglycerin, [[Nitroglycerin]])
- IV: nitroglycerin drip (see Nitroglycerin, [[Nitroglycerin]])
- Transdermal: nitro-paste, nitro-patch (see Nitroglycerin, [[Nitroglycerin]])
- Adverse Effects
- Headache (se Headache, [[Headache]])
- Hypotension (see Hypotension, [[Hypotension]])
- Clinical Efficacy
- GISSI-3 Trial of Transdermal Glyceryl Trinitrate and Lisinopril in Acute MI (Lancet, 1994) [MEDLINE]
- Nitrates Had No Impact on 6-Week Mortality or Mortality and LV Dysfunction
- GISSI-3 Trial of Transdermal Glyceryl Trinitrate and Lisinopril in Acute MI (Lancet, 1994) [MEDLINE]
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Sublingual Nitroglycerin (0.4 mg) Should Be Administered q5min x3 for Ongoing Ischemic Discomfort (Class of Recommendation: I, Level of Evidence: C): after this, decision should be made regarding intravenous nitroglycerin
- Nitrates are Recommended in Unstable Angina/NSTEMI with Ongoing Angina (Class of Recommendation I, Level of Evidence C), Ischemic EKG Changes, and for Chest Pain After Cocaine Use (Class of Recommendation I, Level of Evidence C)
- Intravenous Nitroglycerin is Indicated for Persistent Ischemia, Hypertension, and/or Congestive Heart Failure (Class of Recommendation: I, Level of Evidence: B)
- Use of Intravenous Nitroglycerin Should Not Preclude the Use of Beta Blockers or ACE Inhibitors (Class of Recommendation: I, Level of Evidence: B)
- Nitrates Should Not Be Used with SBP <90 mm Hg or >30 mm Hg Below Baseline SBP, Severe Bradycardia (HR <50 bpm), or Tachycardia (HR >100 bpm) Occurring in the Absence of Symptomatic Congestive Heart Failure or RV Infarction (From 2013 Guidelines)
- Nitrates are Contraindicated in Patients Who Had Received a Phosphodiesterase Inhibitor for Erectile Dysfunction Within 24 hrs of Sildenafil/Vardenafil or 48 hrs of Tadalafil Use (Class of Recommendation: III, Level of Evidence: B)
Non-Steroidal Anti-Inflammatory Drugs (NSAID) (see Non-Steroidal Anti-Inflammatory Drug, [[Non-Steroidal Anti-Inflammatory Drug]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Non-Aspirin NSAID’s (Non-Selective or COX-2 Selective) Should Be Discontinued at Time of Unstable Angina/NSTEMI Presentation and Should Not Be Used During Hospitalization for NSTEMI-ACS (Class of Recommendation: III, Level of Evidence: B): due to risk of mortality, reinfarction, hypertension, congestive heart failure, and myocardial rupture
Oxygen (see Oxygen, [[Oxygen]])
- Pharmacology: improves coronary oxygenation
- Studies
- Study of Supplemental Oxygen in STEMI (Circulation, 2015) [MEDLINE]: supplemental oxygen in patients with STEMI, but without hypoxia, may increase early myocardial injury and is associated with larger myocardial infarct size assessed at 6 mo
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Supplemental Oxygen Should Be Administered for SaO2 <90%, Respiratory Distress, or High Risk Features for Hypoxemia (Class of Recommendation: I, Level of Evidence: C)
- Supplemental Oxygen May Be Administered to All Patients with Unstable Angina/NSTEMI (Class of Recommendation: IIa, Level of Evidence: C)
Percutaneous Coronary Intervention (PCI) (see Percutaneous Coronary Intervention, [[Percutaneous Coronary Intervention]])
- Indications
- STEMI
- Background
- Only 25% of US Hospitals Have PCI Capability
- Clinical Efficacy
- Primary PCI is More Effective in Restoring Coronary Blood Flow than Thrombolytics
- Decreases Mortality Rate, Rate of Recurrent MI, and Rate of Stroke, as Compared to Thrombolytics
- Decreases Bleeding Rate, as Compared to Thrombolytics
- The Incremental Benefit of Primary PCI Over Thrombolytics Disappears When PCI-Related Delay (Door-toBalloon Minus Door-to-Needle Time) Exceeds 60 min: based on this, ons-ire thrombolysis is preferred in STEMI if Transfer to a PCI-Capable Center Cannot Be Achieved Within 90 min on Patient Arrival
- Primary PCI is More Effective in Restoring Coronary Blood Flow than Thrombolytics
- Technique: best outcome is when TIMI-3 flow is restored
- Balloon Angioplasty: higher rate of acute thrombosis and long-term thrombosis (within months), as compared to coronary artery stent
- Coronary Artery Stent
- Bare Metal Stent: preferred when the risk of subsequent bleeding with prolonged anti-platelet therapy is high
- Drug-Eluting Stent: coated with sirolimus, these stents retard the development of intimal hyperplasia (neointima), which could potentially restenosis the stent
- However, this also delays the endothelialization of the stent itself, making ASA+clopidogrel necessary for at least 12 mo to decrease the risk of stent thrombosis
- Rate of in-stent thrombosis on patients with dual ASA+clopidogrel therapy: 1-2% in the first year
Proton Pump Inhibitors (see Proton Pump Inhibitors, [[Proton Pump Inhibitors]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Proton Pump Inhibitors Should Be Used in Patients with a History of GI Bleeding Who Require Triple Anti-Thrombotic Therapy (Coumadin + Aspirin + P2Y12 Receptor Inhibitor) (Class of Recommendation: I, Level of Evidence: C)
- Proton Pump Inhibitors are Reasonable in Patients Without a Known History of GI Bleeding Who Require Triple Anti-Thrombotic Therapy (Coumadin + Aspirin + P2Y12 Receptor Inhibitor) (Class of Recommendation: IIa, Level of Evidence: C)
Ranolazine (see Ranolazine, [[Ranolazine]])
- Pharmacology: late sodium channel blocker
- Recommendations (ACCF/AHA Unstable Angina/NSTEMI Guidelines; Circulation, 2013) [MEDLINE]
- No Formal Recommendation for Ranolazine Use
Statins (see HMG-CoA Reductase Inhibitors, [[HMG-CoA Reductase Inhibitors]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- High-Intensity Statins Should be Initiated or Continued in All Patients, if There are No Contraindications (Class of Recommendation: I, Level of Evidence: A)
- It is Reasonable to Obtain a fasting Lipid Profile within 24 hrs of Presentation (Class of Recommendation: IIa, Level of Evidence: C)
Stress Test
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Non-Invasive Stress Testing is Recommended in Low and Intermediate-Risk Patients Who Have Been Free of Ischemia at Rest or with Low-Level Activity for a Minimum of 12-24 hrs (Class of Recommendation: I, Level of Evidence: B)
- Non-Invasive Imaging Testing is Recommended to Evaluate LV Function in Patients with a Definite ACS (Class of Recommendation: I, Level of Evidence: C)
Treatments Which Do Not Have Clinical Benefit in NSTEMI/ACS
- Thrombolytics (see Thrombolytics, [[Thrombolytics]])
- xxxx
Management of Special Clinical Subsets of Patients with NSTEMI/ACS
Cocaine/Methamphetamine Abuse (see Cocaine, [[Cocaine]] and Methamphetamine, [[Methamphetamine]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Patients with NSTEMI-ACS and a Recent History of Cocaine/Methamphetamine Use Should Be Treated in the Standard Manner (Class of Recommendation: I, Level of Evidence: C)
- Exception: Beta Blockers Should Not Be Used in Acute Cocaine/Methamphetamine Intoxication (with Euphoria, Tachycardia, and/or Hypertension) Due to the Risk of Potentiating Coronary Artery Vasospasm (Class of Recommendation: III, Level of Evidence: C)
- Benzodiazepines Alone or in Combination with Nitroglycerin are Reasonable for the Management of Hypertension/Tachycardia in NSTEMI-ACS During Acute Cocaine/Methamphetamine Intoxication (Class of Recommendation: IIa, Level of Evidence: C)
- Patients with NSTEMI-ACS and a Recent History of Cocaine/Methamphetamine Use Should Be Treated in the Standard Manner (Class of Recommendation: I, Level of Evidence: C)
Treatment of ST Elevation Myocardial Infarction (STEMI)
Bed Rest
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- xxxx
Anticoagulation
- Pharmacology: prevents further propagation of partially occlusive intracoronary thrombus and facilitates dissolution by endogenous mechanisms
- Anticoagulation: in STEMI, heparin maintains coronary patency, once established
- Unfractionated Heparin (see Heparin, [[Heparin]])
- Enoxaparin (Lovenox) (see Enoxaparin, [[Enoxaparin]])
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- For Patients with STEMI Undergoing Primary PCI, Anticoagulation is Recommended with Unfractionated Heparin (with Additional Boluses Administered as Required to Maintain Therapeutic Activated Clotting Time Levels, Taking into Account Whether a Platelet IIb/ IIIa Receptor Antagonist Has Been Also Administered) (Class of Evidence: I, Level of Evidence: C)
- Bivalirudin (Angiomax, Angiox) Can Be Alternately Used (see Bivalirudin, [[Bivalirudin]])
- For Patients with STEMI Undergoing Primary PCI, Anticoagulation is Recommended with Unfractionated Heparin (with Additional Boluses Administered as Required to Maintain Therapeutic Activated Clotting Time Levels, Taking into Account Whether a Platelet IIb/ IIIa Receptor Antagonist Has Been Also Administered) (Class of Evidence: I, Level of Evidence: C)
Anti-Platelet Therapy
- Pharmacology: prevents further propagation of partially occlusive intracoronary thrombus and facilitates dissolution by endogenous mechanisms
- Agents
- Aspirin (see Acetylsalicylic Acid, [[Acetylsalicylic Acid]]): irreversible COX-1 inhibitor, preventing collagen-induced platelet activation and synthesis of thromboxane A2 (a platelet activator)
- Cangrelor (Kengreal) (see Cangrelor, [[Cangrelor]])
- Clopidogrel (Plavix) (see Clopidogrel, [[Clopidogrel]]): thienopyridine P2Y12 platelet receptor antagonist which prevents ADP-induced platelet aggregation
- Prasugrel (Effient) (see Prasugrel, [[Prasugrel]])
- Ticagrelor (Brilinta) (see Ticagrelor, [[Ticagrelor]])
- Clinical Efficacy
- ISIS-2 Trial in Acute MI (BMJ, 1998) [MEDLINE]
- Aspirin Decreased 35-Day Mortality by 23% in STEMI
- Trial of Clopidogrel in Wide Range of Acute MI’s, NSTEMI and STEMI (Lancet, 2005) [MEDLINE]
- Clopidogrel Added to Aspirin and Other Standard Treatments Decreased Mortality and Other Vascular Events in the Hospital
- ISIS-2 Trial in Acute MI (BMJ, 1998) [MEDLINE]
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Aspirin (162-325 mg) Should Be Given Before Primary PCI (Class of Evidence: I, Level of Evidence: B)
- After PCI, Aspirin Should Be Continued Indefinitely (Class of Evidence: I, Level of Evidence: A)
- A Loading Dose of a P2Y12 Receptor Inhibitor Should Be Given as Early as Possible or at Time of Primary PCI to Patients (Class of Evidence: I, Level of Evidence: B): clopidogrel, ticagrelor, or prasugrel
- Prasugrel Should Not Be Administered to Patients with a History of Prior Stroke/TIA (Class of Evidence: I, Level of Evidence: B)
Beta Blockers (see β-Adrenergic Receptor Antagonists, [[β-Adrenergic Receptor Antagonists]])
- Pharmacology: mediated mostly via the blockade of the cardiac β1 adrenergic receptor
- Decease Sympathetic Drive to Myocardium
- Decrease Heart Rate
- Decrease Myocardial Contractility and Myocardial O2 Consumption
- Increase Rhythm Stability
- Decrease Progression from Unstable Angina to Acute MI
- Decrease the Mortality Rate in Acute MI
- Decease Sympathetic Drive to Myocardium
- Contraindications
- Bradycardia (see Sinus Bradycardia, [[Sinus Bradycardia]])
- Bronchospasm (see Obstructive Lung Disease, [[Obstructive Lung Disease]])
- Decompensated Congestive Heart Failure (CHF) (see Congestive Heart Failure, [[Congestive Heart Failure]])
- Hypotension (see Hypotension, [[Hypotension]])
- RV Infarction/Right Ventricular Dysfunction (see Congestive Heart Failure, [[Congestive Heart Failure]]): these patients are exquisitely preload-dependent
- Agents
- Bisoprolol (Concor, Zebeta) (see Bisoprolol, [[Bisoprolol]])
- Carvedilol (Coreg) (see Carvedilol, [[Carvedilol]])
- Metoprolol (Toprol) (see Metoprolol, [[Metoprolol]])
- Clinical Efficacy
- Meta-Analysis of Beta Blocker Use in Acute MI (NEJM, 1992) [MEDLINE]
- Beta Blockers Decreased the Mortality Rate by 28% at 1 week in ACS, with Most of the Benefit Occurring in the First 48 hrs
- Beta Blockers Demonstrated an 18% Reduction in Cumulative Rate of Reinfarction
- Beta Blockers Demonstrated an 15% Reduction in Cumulative Rate of Cardiac Arrest
- Systematic Review and Meta-Analysis of Beta Blockers in Acute MI (BMJ, 1999) [MEDLINE]
- Beta Blockers Decreased Long-Term Mortality Rate in Acute MI
- Meta-Analysis of Beta Blocker Use in Acute MI (NEJM, 1992) [MEDLINE]
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Beta Blockers Should Be Used within the First 24 hrs in Patients Without Signs of Congestive Heart Failure, Low Cardiac Output State, Increased Risk for Cardiogenic Shock, or Other Contraindications to Beta Blocker Therapy (PR-Interval >0.24 sec, Second or Third-Degree Heart Block, or Active Asthma/Reactive Airway Disease) (Class of Recommendation: I, Level of Evidence: B)
- Patients Who are Initially Ineligible for Beta Blockers Should Be Subsequently Reevaluated for Later Beta Blocker Use (Class of Recommendation: I, Level of Evidence: C)
- Beta Blockers Should Be Continued During and After Hospitalization (Class of Recommendation: I, Level of Evidence: B)
- Intravenous Beta Blockers are Suggested for Patients with STEMI (and Unstable Angina/NSTEMI) with Hypertension or Ongoing Myocardial Ischemia (Class of Recommendation: IIa, Level of Evidence: B)
- Beta Blockers Should Be Continued for 3 Years After Acute MI in the Absence of LV Dysfunction (Class of Recommendation I, Level of Evidence A) (AHA/ACCF Secondary Prevention and Risk Reduction Guidelines; Circulation, 2011) [MEDLINE]
- Beta Blockers May Be Considered Beyond 3 Years (Class of Recommendation: IIa, Level of Evidence: B) (AHA/ACCF Secondary Prevention and Risk Reduction Guidelines; Circulation, 2011) [MEDLINE]
- Beta Blockers Should Be Used within the First 24 hrs in Patients Without Signs of Congestive Heart Failure, Low Cardiac Output State, Increased Risk for Cardiogenic Shock, or Other Contraindications to Beta Blocker Therapy (PR-Interval >0.24 sec, Second or Third-Degree Heart Block, or Active Asthma/Reactive Airway Disease) (Class of Recommendation: I, Level of Evidence: B)
Calcium Channel Blockers (see Calcium Channel Blockers, [[Calcium Channel Blockers]])
- Indications
- Atrial Fibrillation with Rapid Ventricular Response (see Atrial Fibrillation, [[Atrial Fibrillation]])
- Chest Pain (see Chest Pain, [[Chest Pain]])
- Hypertension (see Hypertension, [[Hypertension]])
- Contraindicaions
- Pulmonary Edema/Severe Congestive Heart Failure (CHF) (see Congestive Heart Failure, [[Congestive Heart Failure]]): for non-dihydropyridine calcium channel blockers (which have negative inotropic effects)
- Pharmacology
- Decreased Heart Rate
- Decreased Myocardial Contractility: caution is advised when using calcium channel blockers in the setting of LV dysfunction
- Vasodilation
- Agents
- Dihydropyridine Calcium Channel Blockers (Amlodipine, Nifedipine): predominately produce vasodilation, resulting in a decrease in blood pressure and reflex tachycardia
- Non-Sustained Release Nifedipine Should Be Avoided in ACS (in the Absence of Beta Blockers) for this Reason
- Non-Dihydropyridine Calcium Channel Blockers (Diltiazem, Verapamil): predominately decrease heart rate, the rate of atrioventricular conduction, blood pressure, and myocardial contractility
- Dihydropyridine Calcium Channel Blockers (Amlodipine, Nifedipine): predominately produce vasodilation, resulting in a decrease in blood pressure and reflex tachycardia
- Clinical Efficacy
- Review of Calcium Channel Blockers in Acute MI (BMJ, 1989) [MEDLINE]
- Calcium Channel Blockers Did Not Impact Infarct Size, Rate of Reinfarction, or Mortality Rate
- Review of Calcium Channel Blockers in Acute MI (BMJ, 1989) [MEDLINE]
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- No Formal Recommendations About Calcium Channel Blocker Use
Cardiac Catheterization with Coronary Angiography (see Cardiac Catheterization, [[Cardiac Catheterization]])
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Immediate Coronary Angiogram (and PCI When Indicated) Should Be Performed in Resuscitated Out-of-Hospital Cardiac Arrest Patients Whose Initial EKG Demonstrates STEMI (Class of Recommendation: I, Level of Evidence: B)
Coronary Artery Bypass Graft (CABG) (see Coronary Artery Bypass Graft, [[Coronary Artery Bypass Graft]])
- Indications
- Significant Left Main Disease (>50%) (Class of Recommendation: I)
- Three-Vessel CAD, Especially in Patients with LV-EF <50%) (Class of Recommendation: I)
- Two-Vessel CAD with Significant Proximal LAD Stenosis and Either LV-EF <50% or Ischemia on Stress Testing (Class of Recommendation: I)
- Poor or No Options for PCI in Patient with Ongoing Ischemia Refractory to Medical Therapy (Class of Recommendation: I)
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Urgent CABG is indicated in patients with STEMI and coronary anatomy not amenable to PCI who have ongoing or recurrent ischemia, cardiogenic shock, severe heart failure, or other high-risk features (Class of Recommendation: I, Level of Evidence: B)
- CABG is Recommended in Patients at Time of Operative Repair of Mechanical Defects (Class of Recommendation: I, Level of Evidence: B)
Inhibitors of the Renin-Angiotensin-Aldosterone System
- Rationale: activation of the renin-angiotensin-aldosterone system by a number of factors is known to occur in the setting of ACS -> results in increased production of angiotensin II with increased systematic vascular resistance, myocardial workload, and myocardial oxygen consumption
- Inhibitors of the Renin-Angiotensin-Aldosterone System Also Function to Inhibit the Downstream Detrimental Pathways Which Lead to Long-Term Fibrosis and Myocardial/Vascular Remodeling
- Pharmacology
- Aldosterone Antagonists
- Spironolactone (Aldactone) (see Spironolactone, [[Spironolactone]])
- Angiotensin Converting Enzyme (ACE) Inhibitors (see Angiotensin Converting Enzyme Inhibitors, [[Angiotensin Converting Enzyme Inhibitors]]): prevent adverse ventricular remodeling (ie: detrimental increase in ventricular size, which increases ventricular wall stress, impairs systolic contractile function, and increases likelihood of aneurysm formation, CHF, and ventricular arrhythmias)
- Remodeling is Reduced by Decreasing Infarct Size (by Repercussion) and Afterload Reduction (Due to Inhibition of the Renin-Angiotensin System)
- Angiotensin II Receptor Blockers (ARB’s) (see Angiotensin II Receptor Blockers, [[Angiotensin II Receptor Blockers]])
- Aldosterone Antagonists
- Clinical Efficacy
- GISSI-3 Trial of Transdermal Glyceryl Trinitrate and Lisinopril in Acute MI (Lancet, 1994) [MEDLINE]
- Lisinopril Decreased the 6-Week Mortality Rate and the Composite Endpoint of Mortality and Severe LV Dysfunction
- GISSI-3 Trial of Transdermal Glyceryl Trinitrate and Lisinopril in Acute MI (Lancet, 1994) [MEDLINE]
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Aldosterone Antagonists Should Be Administered In Addition to Beta Blocker and ACE Inhibitor with an LV EF ≤40% and Either Congestive Heart Failure or Diabetes Mellitus (Class of Evidence: I, Level of Evidence: B)
- ACE Inhibitors Should Be Administered within the First 24 hrs to Patients with Anterior STEMI, Congestive Heart Failure, LV EF ≤40% (Class of Evidence: I, Level of Evidence: A)
- ACE Inhibitors May Be Reasonable for Other STEMI Patients, As Well (Class of Evidence: IIa, Level of Evidence: A)
- ARB Should Be Administered to Patients Who are Intolerant of ACE Inhibitors (Class of Evidence: I, Level of Evidence: B)
Intra-Aortic Balloon Pump (IABP (see Intra-Aortic Balloon Pump, [[Intra-Aortic Balloon Pump]])
- Physiology
- xxxx
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- The Use of Intra-Aortic Balloon Pump (IABP) Can Be Useful for Patients with Cardiogenic Shock after STEMI Who Do Not Quickly Stabilize with Pharmacological Therapy (Class of Recommendation: IIa, Level of Evidence: B)
Morphine Sulfate (see Morphine, [[Morphine]])
- Pharmacology
- Anxiolytic
- Decreases Work of Breathing
- Favorable Effect on Ventricular Loading
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Morphine is Useful to Relieve Ischemic Pain and Treat Pulmonary Edema
Nitrates (see Nitrites and Nitrates, [[Nitrites and Nitrates]])
- Indications
- Chest Pain (see Chest Pain, [[Chest Pain]])
- Hypertension (see Hypertension, [[Hypertension]])
- Congestive Heart Failure (CHF) (see Congestive Heart Failure, [[Congestive Heart Failure]])
- Contraindications
- Hypotension (see Hypotension, [[Hypotension]])
- RV Infarction/Right Ventricular Dysfunction (see Congestive Heart Failure, [[Congestive Heart Failure]]): these patients are exquisitely preload-dependent
- Significant Bradycardia (see Sinus Bradycardia, [[Sinus Bradycardia]])
- Significant Tachycardia (see Sinus Tachycardia, [[Sinus Tachycardia]])
- Use of Phosphodiesterase Type 5 Inhibitors (PDE5 Inhibitors) (see Phosphodiesterase Type 5 Inhibitors, [[Phosphodiesterase Type 5 Inhibitors]]): may result in profound hypotension
- Sildenafil (Viagra) (see Sildenafil, [[Sildenafil]])
- Pharmacology
- Normal and Diseased Coronary Artery Vasodilation: improves anterograde and collateral coronary blood flow
- Prevention of Coronary Artery Vasospasm: improves coronary blood flow
- Provides Symptomatic Relief of Chest Pain
- Systemic Vasodilation, Resulting in Decreased Blood Pressure and Decreased Afterload
- Venodilation with Decreased Preload and Decreased LV End-Diastolic Volume, Resulting in Decreased Myocardial Oxygen Consumption
- No Impact on Myocardial Infarction Rate or Mortality Rate
- Administration
- PO: nitro-BID (see Nitroglycerin, [[Nitroglycerin]])
- SL: nitroglycerin sublingual (see Nitroglycerin, [[Nitroglycerin]])
- IV: nitroglycerin drip (see Nitroglycerin, [[Nitroglycerin]])
- Transdermal: nitro-paste, nitro-patch (see Nitroglycerin, [[Nitroglycerin]])
- Adverse Effects
- Headache (se Headache, [[Headache]])
- Hypotension (see Hypotension, [[Hypotension]])
- Clinical Efficacy
- GISSI-3 Trial of Transdermal Glyceryl Trinitrate and Lisinopril in Acute MI (Lancet, 1994) [MEDLINE]
- Nitrates Had No Impact on 6-Week Mortality or Mortality and LV Dysfunction
- GISSI-3 Trial of Transdermal Glyceryl Trinitrate and Lisinopril in Acute MI (Lancet, 1994) [MEDLINE]
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- No Formal Recommendations for the Use of Nitrates in STEMI
Non-Steroidal Anti-Inflammatory Drugs (NSAID) (see Non-Steroidal Anti-Inflammatory Drug, [[Non-Steroidal Anti-Inflammatory Drug]])
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Non-Aspirin NSAID’s (Non-Selective or COX-2 Selective) Should Be Discontinued at Time of STEMI Presentation and Should Not Be Used During Hospitalization for STEMI: due to risk of mortality, reinfarction, hypertension, congestive heart failure, and myocardial rupture
Oxygen (see Oxygen, [[Oxygen]])
- Pharmacology
- Improves Coronary Oxygenation
- May Increase Coronary Vascular Resistance
- Studies
- Study of Supplemental Oxygen in STEMI (Circulation, 2015) [MEDLINE]: supplemental oxygen in patients with STEMI, but without hypoxia, may increase early myocardial injury and is associated with larger myocardial infarct size assessed at 6 mo
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- No Formal Recommendations, But May Be Used for Patients with SaO2 >90%
Percutaneous Coronary Intervention (PCI) (see Percutaneous Coronary Intervention, [[Percutaneous Coronary Intervention]])
- Indications
- STEMI
- Background
- Only 25% of US Hospitals Have PCI Capability
- Clinical Efficacy
- Primary PCI is More Effective in Restoring Coronary Blood Flow than Thrombolytics
- Decreases Mortality Rate, Rate of Recurrent MI, and Rate of Stroke, as Compared to Thrombolytics
- Decreases Bleeding Rate, as Compared to Thrombolytics
- The Incremental Benefit of Primary PCI Over Thrombolytics Disappears When PCI-Related Delay (Door-toBalloon Minus Door-to-Needle Time) Exceeds 60 min: based on this, ons-ire thrombolysis is preferred in STEMI if Transfer to a PCI-Capable Center Cannot Be Achieved Within 90 min on Patient Arrival
- Primary PCI is More Effective in Restoring Coronary Blood Flow than Thrombolytics
- Technique: best outcome is when TIMI-3 flow is restored
- Balloon Angioplasty: higher rate of acute thrombosis and long-term thrombosis (within months), as compared to coronary artery stent
- Coronary Artery Stent
- Bare Metal Stent: preferred when the risk of subsequent bleeding with prolonged anti-platelet therapy is high
- Drug-Eluting Stent: coated with sirolimus, these stents retard the development of intimal hyperplasia (neointima), which could potentially restenosis the stent
- However, this also delays the endothelialization of the stent itself, making ASA+clopidogrel necessary for at least 12 mo to decrease the risk of stent thrombosis
- Rate of in-stent thrombosis on patients with dual ASA+clopidogrel therapy: 1-2% in the first year
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Immediate Coronary Angiogram (and PCI When Indicated) Should Be Performed in Resuscitated Out-of-Hospital Cardiac Arrest Patients Whose Initial EKG Demonstrates STEMI (Class of Recommendation: I, Level of Evidence: B)
- Primary PCI should be performed in patients with STEMI and ischemic symptoms of <12 hrs duration (Class of Recommendation: I, Level of Evidence: A)
- Primary PCI should be performed in patients with STEMI and ischemic symptoms of <12 hrs duration who have contraindications to fibrinolytic therapy, irrespective of the time delay
from First Medical Contact (Class of Recommendation: I, Level of Evidence: B) - Primary PCI should be performed in patients with STEMI and cardiogenic shock or acute severe HF, irrespective of time delay from MI onset (Class of Recommendation: I, Level of Evidence: B)
- Primary PCI is reasonable in patients with STEMI if there is clinical and/or ECG evidence of ongoing ischemia between 12-24 hrs after symptom onset (Class of Recommendation: IIa, Level of Evidence: B)
- PCI Should Not Be Performed in a Non-Infarct Artery at the Time of Primary PCI in Patients with STEMI Who are Hemodynamically Stable (Class of Recommendation: III, Level of Evidence: B)
- Placement of a Stent (Bare Metal or Drug-Eluting) is Useful in Primary PCI (Class of Recommendation: I, Level of Evidence: A)
- Bare Metal Stents Should be Used in Patients with High Bleeding Risk, Inability to Comply with 1 year of Dual Anti-Platelet Therapy, or Anticipated Invasive or Surgical Procedures in the Next 1 yr (Class of Recommendation: I, Level of Evidence: C)
- Drug-Eluting Stents Should Not Be Used in Primary PCI for Patients with STEMI Who are Unable to Tolerate or Comply with a Prolonged Course of Dual Anti-Platelet Therapy Because of the Increased Risk of Stent Thrombosis with Premature Discontinuation of One or Both Agents (Class of Recommendation: I, Level of Evidence: B)
Ranolazine (see Ranolazine, [[Ranolazine]])
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- No Formal Recommendation for Ranolazine Use
Statins (see HMG-CoA Reductase Inhibitors, [[HMG-CoA Reductase Inhibitors]])
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- High-Intensity Statin Therapy Should Be Initiated or Continued in All Patients with STEMI, Assuming No Contraindications (Class of Recommendation: I, Level of Evidence: B)
Thrombolytic Therapy (see Thrombolytics, [[Thrombolytics]])
- Indications
- STEMI
- Contraindications in the Setting of STEMI (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Absolute
- Any prior ICH
- Known structural cerebral vascular lesion (eg, arteriovenous malformation)
- Known malignant intracranial neoplasm (primary or metastatic)
- Ischemic stroke within 3 mo
- EXCEPT acute ischemic stroke within 4.5 h
- Suspected aortic dissection
- Active bleeding or bleeding diathesis (excluding menses)
- Signicant closed-head or facial trauma within 3 mo
- Intracranial or intraspinal surgery within 2 mo
- Severe uncontrolled hypertension (unresponsive to emergency therapy)
- For streptokinase, prior treatment within the previous 6 mo
- Relative
- History of Chronic, Severe, Poorly-Controlled Hypertension (see Hypertension, [[Hypertension]])
- Signicant Hypertension on Presentation (SBP >180 mm Hg or DBP >110 mm Hg) (see Hypertension, [[Hypertension]])
- History of Prior Ischemic Stroke >3 mo (see Ischemic Cerebrovascular Accident, [[Ischemic Cerebrovascular Accident]])
- Dementia (see Dementia, [[Dementia]])
- Known intracranial pathology not covered in absolute contraindications Traumatic or prolonged (>10 min) CPR
- Major Surgery (<3 wks)
- Recent Internal Bleeding (Within 2-4 wks)
- Noncompressible Vascular Punctures
- Pregnancy (see Pregnancy, [[Pregnancy]])
- Active Peptic Ulcer Disease (PUD) (see Peptic Ulcer Disease, [[Peptic Ulcer Disease]])
- Oral anticoagulant therapy
- Absolute
- Pharmacology
- Decreases myocardial necrosis and improves survival
- Earlier intervention -> greater myocardial salvage
- Optimal flow in STEMI patients is achieved in only 70% of patients
- Agents
- Alteplase (see Alteplase, [[Alteplase]])
- Recommendations (2014 AHA/ACC NSTEMI-ACS Guidelines; J Am Coll Cardiol, 2014)* [MEDLINE]
- Intravenous Thrombolytics are Not Recommended without ST-Segment Elevation, True Posterior MI, or Presumed New LBBB (Class of Recommendation: III, Level of Evidence: A)
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Indicated When PCI is Not Available
Other Therapies with No Defined Clinical Benefit
- Pexelizumab (see Pexelizumab, [[Pexelizumab]]):
- Systematic Review of Pexelizumab (J Thorac Cardiovasc Surg, 2008) [MEDLINE]: no clinical benefit in STEMI, but may decrease mortality rate in patients undergoing coronary artery bypass grafting
Management of Special Clinical Subsets of Patients with STEMI
Ventricular Arrhythmias
- Automatic Implantable Cardioverter-Defibrillator (AICD) (see Automatic Implantable Cardioverter-Defibrillator, [[Automatic Implantable Cardioverter-Defibrillator]])
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- AICD is Indicated Before Discharge in Patients Who Develop Sustained VT/VF >48 hrs After STEMI, Provided the Arrhythmia is Not Due to Transient or Reversible Ischemia, Reinfarction, or Metabolic Abnormalities (Class of Recommendation: I, Level of Evidence: B)
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
Cardiogenic Shock (see Cardiogenic Shock, [[Cardiogenic Shock]])
- Recommendations (ACCF/AHA STEMI Guidelines; Circulation, 2013) [MEDLINE]
- Emergency Revascularization with Either PCI or CABG is Recommended in Suitable Patients with Cardiogenic Shock Due to Pump Failure after STEMI, Irrespective of the Time Delay from MI Onset (Class of Recommendation: I, Level of Evidence: B)
- Alternative LV Assist Devices for Circulatory Support May Be Considered in Patients with Refractory Cardiogenic Shock (Class of Recommendation: IIb, Level of Evidence: C)
Left Ventricular Aneurysm (see Left Ventricular Aneurysm, [[Left Ventricular Aneurysm]])
- xxx
Left Ventricular Free Wall Rupture (see xxxx, [[xxxx]])
- xxx
Mitral Regurgitation (see xxxx, [[xxxx]])
- xxxx
Right Ventricular Infarction
- Recommendations
- Maintain RV Preload
- Decrease RV Afterload
- Inotropic Support (As Required)
- Immediate Reperfusion
- Coronary Artery Bypass Graft (CABG) (see Coronary Artery Bypass Graft, [[Coronary Artery Bypass Graft]])
- Percutaneous Coronary Intervention (PCI) (see Percutaneous Coronary Intervention, [[Percutaneous Coronary Intervention]])
- Avoidance of Nitrates and Diuretics: these can precipitate hypotension
Ventricular Septal Rupture (see Ventricular Septal Rupture, [[Ventricular Septal Rupture]])
- xxx
Prognosis
- Poor Prognostic Factors for CAD
- Increased with greater number of affected vessels
- Poor LV-EF
- Poor exercise capacity
- Magnitude of anginal symptoms
- Mortality rates have decreased 50% in recent decades: due to risk factor modifications, as well as better pharmacologic and mechanical management of ACS
References
General
- Prevalence of total coronary occlusion during the early hours of 16. transmural myocardial infarction. N Engl J Med. 1980;303:897–902. doi: 10.1056/NEJM198010163031601 [MEDLINE]
- Coronary arteriographic findings soon after non-Q-wave myocardial infarction. N Engl J Med. 1986;315:417–423. doi: 10.1056/ NEJM198608143150703 [MEDLINE]
- Electrocardiographic manifestations of right ventricular infarction. Am Heart J. 1989; 118:138–44 [MEDLINE]
- The electrocardiogram predicts one-year outcome of patients with unstable angina and non-Q wave myocardial infarction: results of the TIMI III Registry ECG Ancillary Study. Thrombolysis in Myocardial Ischemia. J Am Coll Cardiol. 1997;30(1):133 [MEDLINE]
- Elevated cardiac troponin is an independent risk factor for short- and long-term mortality in medical intensive care unit patients. Crit Care Med. 2008;36:759–765 [MEDLINE]
- POISE (PeriOperative ISchemic Evaluation) Investigators. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med. 2011;154:523–528 [MEDLINE]
- Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020 [MEDLINE]
- Mechanisms of acute coronary syndromes and their implications for therapy. N Engl J Med. 2013;368:2004–2013 [MEDLINE]
- Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015 Mar 10;131(10):861-70. doi: 10.1161/CIRCULATIONAHA.114.011201. Epub 2015 Jan 13 [MEDLINE]
Treatment
General
- Cumulative meta-analysis of therapeutic trials for myocardial infarction. N Engl J Med. 1992; 327:248–254 [MEDLINE]
- AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and other Atherosclerotic Vascular Disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation. 2011; 124:2458–2473 [MEDLINE]
- 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Jun 11;127(23):e663-828. doi: 10.1161/CIR.0b013e31828478ac. Epub 2013 Apr 29 [MEDLINE]
- American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013; 127:e362–425 [MEDLINE]
- Nonantithrombotic medical options in acute coronary syndromes: old agents and new lines on the horizon. Circ Res. 2014;114:1944–1958 [MEDLINE]
- 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014 Dec 23;64(24):e139-228. doi: 10.1016/j.jacc.2014.09.017. Epub 2014 Sep 23 [MEDLINE]
- 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Dec 23;130(25):2354-94. doi: 10.1161/CIR.0000000000000133. Epub 2014 Sep 23 [MEDLINE]
Angiotensin Converting Enzyme (ACE) Inhibitors
- GISSI-3: effects of lisinopril and transdermal glyceryl trinitrate singly and together on 6-week mortality and ventricular function after acute myocardial infarction. Gruppo Italiano per lo Studio della Sopravvivenza nell’infarto Miocardico. Lancet. 1994; 343:1115–1122 [MEDLINE]
Anti-Platelet Agents
- ISIS-2: 10 year survival among patients with suspected acute myocardial infarction in randomised comparison of intravenous streptokinase, oral aspirin, both, or neither. the ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. BMJ. 1998;316(7141):1337-1343 [MEDLINE]
- Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: rando- mised placebo-controlled trial. Lancet. 2005;366(9497):1607-1621 [MEDLINE]
Beta Blockers
- Cumulative meta-analysis of therapeutic trials for myocardial infarction. N Engl J Med. 1992; 327:248–254 [MEDLINE]
- Blockade after myocardial infarction: systematic review and meta regression analysis. BMJ. 1999; 318:1730–1737 [MEDLINE]
Calcium Channel Blockers
- Calcium channel blockers in acute myocardial infarction and unstable angina: an overview. BMJ. 1989; 299:1187–1192 [MEDLINE]
Coronary Artery Bypass Graft (CABG)
- Effects of off-pump versus on-pump coronary surgery on reversible and irreversible myocardial injury: a randomized trial using cardiovascular magnetic resonance imaging and biochemical markers. Circulation. 2004;109:345–350 [MEDLINE]
- Relationship of irreversible myocardial injury to troponin I and creatine kinase-MB elevation after coronary artery bypass surgery: insights from cardiovascular magnetic resonance imaging. J Am Coll Cardiol. 2005;45:629–631 [MEDLINE]
Morphine
- Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart J. 2005 Jun;149(6):1043-9 [MEDLINE]
Nitrates
- GISSI-3: effects of lisinopril and transdermal glyceryl trinitrate singly and together on 6-week mortality and ventricular function after acute myocardial infarction. Gruppo Italiano per lo Studio della Sopravvivenza nell’infarto Miocardico. Lancet. 1994; 343:1115–1122 [MEDLINE]