Eliminate Source/Eliminate Contact with Antigen (If Known)
Source Elimitation is Crucial
There is No Evidence that Gastric Emptying of Food Allergens Has Any Clinical Benefit in the Management of Food-Associated Anaphylaxis
Monitoring
Continuous Blood Pressure (BP)
Heart Rate (HR)
Respiratory Rate (RR)
Pulse Oximetry Monitoring of Oxygen Saturations
Establish Intravenous (IV) Access
Intravenous (IV) Access is Necessary to Facilitate Intravenous Fluid Resuscitation
Place Patient in Supine Position
Supine Position Maximizes Perfusion of Vital Organs and Prevents Severe Hypotension, Inadequate Cardiac Filling, and Development of Pulseless Electrical Activity (PEA)/”Empty Ventricle Syndrome” (see Pulseless Electrical Activity)
Conscious Patients with Bronchospasm May Resist Being Placed Supine, as Supine Posture May Exacerbate Dyspnea
In This Setting, Providing Oxygen and Explaining the Reason for Lying Supine are Important (at Least Until the Cardiovascular Status Can Be Assessed and Optimized)
Patients Who are Vomiting and Also Hypotensive Should Be Placed on Their Side (Rather than Supine) to Avoid Aspiration
Adult Basic and Advanced Life Support: 2020 American Heart Association (AHA) Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (Circulation, 2020) [MEDLINE]
Recommendations for Anaphylaxis Without Cardiac Arrest (see Anaphylaxis)
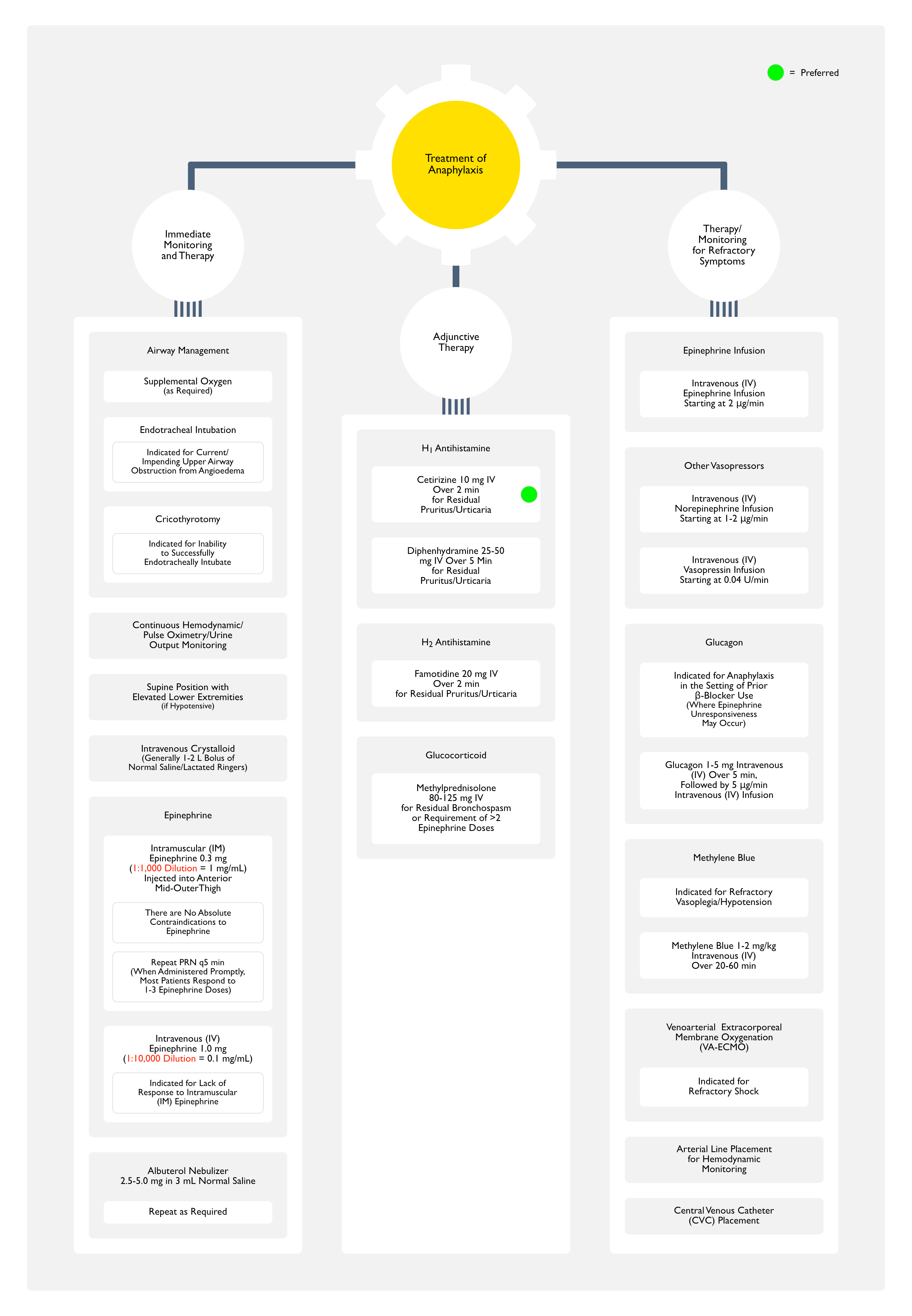
Epinephrine Should Be Administered Early by Intramuscular Injection (or Autoinjector) to All Patients with Signs of a Systemic Allergic Reaction (Especially Hypotension, Airway Swelling, or Difficulty Breathing) (Class of Recommendation: 1, Level of Evidence: C-LD)
Injection of Epinephrine into the Lateral Aspect of the Thigh Produces Rapid Peak Plasma Epinephrine Concentrations
The Recommended epinephrine Dose in Anaphylaxis is 0.2-00.5 mg (1:1,000) Intramuscularly, to Be Repeated q5-15 min as Required (Class of Recommendation: 1, Level of Evidence: C-LD)
In Patients with Anaphylactic Shock, Close Hemodynamic Monitoring is Recommended Class of Recommendation: 1, Level of Evidence: C-LD
Given the Potential for the Rapid Development of Oropharyngeal/Laryngeal Edema, Immediate Referral to a Health Professional with Expertise in Advanced Airway Placement (Including Surgical Airway Management) is Recommended (Class of Recommendation: 1, Level of Evidence: C-LD)
When Anaphylaxis Produces Obstructive Airway Edema, Rapid Advanced Airway management is Critical
In Some Cases, Emergency Cricothyrotomy/Tracheostomy May Be Required
When an Intravenous Line is in Place, it is Reasonable to Consider the Intravenous Route for Epinephrine in Anaphylactic Shock, at a Dose of 0.05-0.1 mg (0.1 mg/mL, aka 1:10 000) (Class of Recommendation: 2a, Level of Evidence: C-LD)
Intravenous Infusion of Epinephrine is a Reasonable Alternative to Intravenous Boluses for the Treatment of Anaphylaxis in Patients Not in Cardiac Arrest (Class of Recommendation: 2a, Level of Evidence: C-LD)
Intravenous Infusion of Epinephrine May Be Considered for Postarrest Shock in Patients with Anaphylaxis (Class of Recommendation: 2b, Level of Evidence: C-LD)
Recommendations for Cardiac Arrest From Anaphylaxis (see Anaphylaxis)
General Comments
There are No Randomized Controlled Trials (RCT’s) Evaluating Alternative Treatment Algorithms for Cardiac Arrest Due to Anaphylaxis
Evidence is Limited to Case Reports and Extrapolations from Non-Fatal Anaphylaxis Cases, Interpretation of Pathophysiology, and Consensus Opinion
Because of Limited Evidence, the Cornerstone of Management of Anaphylaxis-Associated Cardiac Arrest is Standard Basic Life Support/Advanced Cardiac Life Support, Including Airway Management and Early Epinephrine
There is No Proven Benefit from the Use of Antihistamines, Inhaled β2-Agonists, and Intravenous Corticosteroids During Anaphylaxis-Induced Cardiac Arrest
In Cardiac Arrest Secondary to Anaphylaxis, Standard Resuscitative Measures and Immediate Administration of Epinephrine Should Take Priority (Class of Recommendation: 1, Level of Evidence: C-LD)
Observation Period
General Comments
While There is No Consensus Regarding the Optimal Period of Observation for Anaphylaxis, the Following is Reasonable (Clin Med-Lond, 2022) [MEDLINE]
All Patients with Anaphylaxis Should Be Observed Until Symptoms Have Completely Resolved (Including ≥1 hr of Being Completely Symptom-Free
All Patients with Severe Anaphylaxis (Hypotension, Hypoxia, or >2 Epinephrine Doses), Risk Factors for Biphasic Reactions, or a History of Severe Asthma Should Be Observed for ≥12 hrs, Including ≥4 hrs Completely Symptom-Free in an Observation Unit/Inpatient Hospital Setting
Delayed Time to First Epinephrine Treatment (>60 min)
Need for >1 Dose of Epinephrine
Unclear Risk Factors
Unknown Trigger for Anaphylaxis
Possible Ongoing Exposure to Trigger for Anaphylaxis (Such as Sustained-Release/Depot Medication, Food, etc)
Prolonged Interval (i.e. Hours) Between COntact with Trigger and Onset of Anaphylaxis Symptoms
Treatment with Antihistamines/Glucocorticoids without Epinephrine
Observation Period Can Be Customized Based on Patient Characteristics, Reaction Severity, Patient Access to and Ability to Self-Administer Epinephrine, Patient Access to Emergency Medical Care, and Shared Decision-Making
Clinical Efficacy
Pediatric Retrospective Cohort Emergency Department Study of Anaphylaxis Observation Times (Lancet Child Adolesc Health, 2025) [MEDLINE]: n = 7,717
The Observation Period at Which the Increase in Cumulative Incidence of Repeat Epinephrine was <2% was 115 min (95% CI: 105-122) for All Patients, 105 min (54-135) for Patients without Respiratory/Cardiovascular Involvement (n = 1,070), 109 min (98-118) for Patients with Respiratory But No Cardiovascular Involvement (n = 4,076), and 161 min (125-249) for Patients with Cardiovascular Involvement (n = 495)
These Findings Suggest that 95.3% of Patients in the Cohort Would Have Been Safely Discharged 2 hrs After Receiving the First Epinephrine Dose and that 98.1% of Patients Would Have Been Safely Discharged 4 hrs After the First Epinephrine Dose
Conclusions
A 2 Hour Observation Period was Safe for Most Children Who Presented to the Emergency Department with an Acute Allergic Reaction Which Required Epinephrine
A 4 Hour Observation Period May Be Adequate for Patients with Cardiovascular Involvement
Indicated for Inability to Successfully Endotracheally Intubate (Due to Severe Upper Airway Edema Preventing Access to the Glottic Aperture)
Use of an Extraglottic Airway Device (Laryngeal Mask Airway) May Be Considered as a Rescue Maneuver or as a Bridge to Provide Oxygenation/Ventilation While Making Preparations for Cricothyrotomy, But These Devices are Dependent on Normal Upper Airway Anatomy, So They May Not Be Successful
Intravenous Fluids
Indications for Intravenous Fluids
Hypotension/Incomplete Response to Intramuscular (IM) Epinephrine (see Hypotension and Epinephrine)
Intravenous Fluids are Indicated Due to Massive Fluid Shifts Which Occur Associated with Increased Vascular Permeability (Med J Aust. 2006) [MEDLINE] (Allergy, 2007) [MEDLINE] (Resuscitation, 2008) [MEDLINE] (J Allergy Clin Immunol, 2020) [MEDLINE] (World Allergy Organ J, 2020) [MEDLINE]
Patients with Anaphylaxis Can Experience a Transfer of Up to 35% of the Their Intravascular Volume into the Extravascular Space within Minutes (Emerg Med J, 2004) [MEDLINE]
Epinephrine is the Most Important Treatment for Anaphylaxis
Epinephrine Should Be Administered as Soon as Anaphylaxis is Recognized to Prevent the Progression to Life-Threatening Symptoms
Epinephrine Should Also Be Administered to Patients Who Have Symptoms/Signs Consistent with Impending Anaphylaxis When the Clinical Suspicion for Anaphylaxis is High (Even if Formal Diagnostic Criteria or Anaphylaxis Have Not Been Met)
Timeliness of Epinephrine Administration
In the Setting of Anaphylaxis, Delayed Epinephrine Injection is Associated with an Increased Mortality Risk (BMJ, 2003) [MEDLINE] (Allergy, 2007) [MEDLINE] (BMJ, 2008) [MEDLINE] (Allergy, 2009) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2010) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2010) [MEDLINE]
The Pharmacologic Actions of Epinephrine Address the Pathophysiologic Changes Which Occur in Anaphylaxis Better Than Any Other Medication
Epinephrine Decreases Mediator Release from Mast Cells, Prevents/Reverses Obstruction to Airflow in the Upper and Lower Respiratory Tracts, and Prevents/Reverses Cardiovascular Collapse (J Allergy Clin Immunol, 2012) [MEDLINE]
Although epinephrine increases heart rate in healthy individuals, it often leads to a paradoxical decrease (to normal) in the reflex tachycardia characteristic of anaphylaxis
Canadian/Israeli Emergency Department Study (from Cross-Canada Anaphylaxis Registry of Predominantly Pediatric Patients) of Prehospital Anaphylaxis Treatments (Epinephrine, Antihistamines, and Corticosteroids) (Ann Allergy Asthma Immunol, 2023) [MEDLINE]: n = 5,364
Patients Treated with Prehospital Epinephrine were Less Likely to Have Uncontrolled Reactions (>2 Doses of Epinephrine in the Emergency Department) [Adjusted Odds Ratio 0.955 (95%CI 0.943, 0.967)], Receive Intravenous Fluids in Emergency Department [Adjusted Odds Ratio 0.976 (95% CI: 0.959-0.992)], and to Be Admitted Following the Reaction [Adjusted Odds Ratio 0.964 (95% CI: 0.949-0.980)]
Patients Treated with Prehospital Antihistamines were Less Likely to Have Uncontrolled Reactions (>2 Doses of Epinephrine in the Emergency Department) [Adjusted Odds Ratio 0.978 (95% CI: 0.967-0.989)] and to Be Admitted Following the Reaction [Adjusted Odds Ratio 0.963 (95% CI: 0.949-0.977)]
Patients Who Received Prehospital Corticosteroids were More Likely to Require Intravenous Fluids in the Emergency Department [Adjusted Odds Ratio 1.059 (95% CI: 1.013-1.107)] and Be Admitted [Adjusted Odds Ratio 1.232 (95% CI: 1.181-1.286)]
Preferred Route of Epinephrine Administration
Intramuscular (IM) Injection is the Preferred Route for Initial Epinephrine Administration for Anaphylaxis in Most Settings and in Patients of All Ages
Intramuscular (IM) Epinephrine Injection is Recommended Over Subcutaneous Injection Because it Consistently Provides a More Rapid Increase in the Plasma and Tissue Concentrations of Epinephrine (J Allergy Clin Immunol, 1998) [MEDLINE] (J Allergy Clin Immunol, 2001) [MEDLINE]
Intramuscular (IM) Epinephrine Injection is Also Preferred Over Intravenous (IV) Bolus Because it is Faster and is Safer (i.e. Lower Risk of Cardiovascular Complications, Such as Severe Hypertension and Ventricular Arrhythmias) (J Allergy Clin Immunol Pract, 2015) [MEDLINE] (Resuscitation, 2017) [MEDLINE]
Commercial Epinephrine Preparations
Epinephrine is Commercially Available in Different Concentrations
1 mg/mL = 1:1,000 Dilution (Preparation Commonly Used Intramuscularly in Anaphylaxis)
To Assist in Preventing Medication Errors, the “Ratio Expressions” (1:1,000 or 1:10,000) were Removed from Epinephrine Labels in the United States in 2016
0.3 mL Dose Contains 0.3 mg Epinephrine + 1.8 mg Sodium Chloride + 0.5 mg Sodium Metabisulfite + Hydrochloric Acid (to Adjust the pH from 2.2-5.0)
Compendial Limits for Epinephrine Content of Formulations are 90-115% of Labeled Strength (United States Pharmacopeia) (However, in Some Countries, the Stated Content of Epinephrine in Autoinjectors May Range from 0.23-0.37 mg)
Epinephrine Should Be Stored at Room Temperature (15-30°C) to Prevent Oxidation and Inactivation
An EpiPen Jr Contains Epinephrine 0.15 mg + Same Nonmedicinal Ingredients in the Same Amounts as in the EpiPen
0.1 mg/mL = 1:10,000 Dilution (Preparation Commonly Used Intravenous in Advanced Cardiac Life Support/ACLS Protocols)
Repeat Dosing: may repeat q5 min (or sooner, if clinically required)
Approximately 90% of Patients Respond to a Single Intramuscular (IM) Epinephrine Dose, Particularly if it is Given Promptly After the Onset of Anaphylaxis Symptoms (J Allergy Clin Immunol, 2021) [MEDLINE]
Patients with a History of Previous Anaphylaxis and Patients Presenting with Flushing/Diaphoresis/Dyspnea wereMore Likely to Require Multiple Epinephrine Doses to Control Symptoms in an Observational Study (J Allergy Clin Immunol Pract, 2015) [MEDLINE]
Maximum Single Dose: 0.5 mg
Maximum Total Dose: none
The Needle Used in Adults/Children Should Be Long Enough to Penetrate the Subcutaneous Adipose Tissue Over the Vastus Lateralis Muscle
However, Intramuscular (IM) Injection into the Thigh May Be Difficult or Impossible in Some Patients, Particularly Those Who are Overweight/Obese (Ann Allergy Asthma Immunol, 2005) [MEDLINE] (Pediatrics, 2009) [MEDLINE]
In Such Cases, the Best Attempt at Intramuscular (IM) Injection Should Be Achieved
Preloaded Epinephrine Injectable Devices
Advantages
Patient Can Keep Nearby at Home for Emergency Use: do not store in warm/hot places (such as a car), due to drug stability
Shelf-Life: 1 year (when stored properly)
Adult Dose: 0.3 mg IM (1:1000) for adults
Brands
Epipen
Hold Like a Pen, Not Like a Knife (to Avoid Inadvertent Injection into the User’s Thumb)
Remove Blue Safety Cap
Firmly Push Orange Tip Against the Lateral Thigh (Don’t Need to Remove Clothes to Use) Until it Clicks
Hold Device in Place for 5-10 sec
Auvi-Q
Provides Verbal Instructions
Adrenaclick
Pen-Like Device
Epinephrine Nasal Spray was Approved for the Treatment of Allergic Reactions (Including Anaphylaxis) by the US Food and Drug Administration (FDA) in 2024
Intravenous Epinephrine for Refractory Anaphylaxis (see Epinephrine)
Intravenous Epinephrine (Bolus Dosing)
For Anaphylaxis, Note that the Epinephrine Dose is Approximately 1/10th of the Intravenous Epinephrine Dose Used in Cardiac Arrest
Because Intravenous (IV) Bolus Epinephrine is Associated with Significantly More Dosing Errors and Cardiovascular Complications than Intramuscular (IM) Epinephrine, Intravenous (IV) Bolus Epinephrine Should Be Used Only in the Setting of Imminent Circulatory Arrest when an Intravenous Infusion is Not Yet Available
Epinephrine Intravenous (IV) Infusion
Epinephrine Intravenous (IV) Infusion May Be Used for Hypotension Refractory to Intramuscular (IM) Epinephrine and Aggressive Intravenous (IV) Fluids
Dose
Start Epinephrine Intravenous (IV) Infusion at 1-2 μg/min
Adverse Effects of Epinephrine
General Comments
In Patients of All Ages, Epinephrine by Any Route (and in Therapeutic Doses) Commonly Cases Mild Side Effects
Serious Adverse Effects of Epinephrine are More Common After Intravenous Bolus Injection, Particularly in an Inappropriately Large Dose is Administered (BMJ, 2003) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2010) [MEDLINE] (Ann Emerg Med, 2010) [MEDLINE] (J Allergy Clin Immunol Pract, 2015) [MEDLINE]
Patients with Anaphylaxis Who are Taking Monoamine Oxidase (MAO) Inhibitors (Which Inhibit Epinephrine Metabolism)/Tricyclic Antidepressants (TCA’s) (Which Prolong Epinephrine Duration of Action)/Stimulants (Amphetamines, Methylphenidate, Cocaine) or Patients with Preexisting Conditions (Such as Recent Intracranial Surgery, Aortic Aneurysm, or Uncontrolled Hyperthyroidism, Uncontrolled Hypertension) Should Receive Epinephrine (Preferably Intramuscularly) Even Though They Theoretically Might Be at Higher Risk for Adverse Effects
Generally, Glucocorticoids Should Not Be Routinely Used in Patients Who Respond Well to 1-2 Epinephrine Doses
In Anaphylaxis Patients Who Respond Promptly to Epinephrine, There is No Convincing Evidence that Glucocorticoids Provide Additional Clinical Benefits (J Allergy Clin Immunol Pract, 2019) [MEDLINE] (J Allergy Clin Immunol Pract, 2019) [MEDLINE]
In the Past, Glucocorticoids were Believed to Prevent Biphasic Reactions and Given Primarily for this Purpose
However, a 2020 Systematic Review Failed to Support this Practice (J Allergy Clin Immunol, 2020) [MEDLINE]
For Patients with Persistent Bronchospasm (Especially with Known Asthma) Despite an Adequate Response to Epinephrine, Glucocorticoids May Be Considered
It is Reasonable to Administer Glucocorticoids for Patients with Severe Symptoms Requiring >2 Doses of Intramuscular (IM) Epinephrine or in Patients Requiring Intravenous (IV) Epinephrine
Pharmacology
Clinical Efficacy
Canadian/Israeli Emergency Department Study (from Cross-Canada Anaphylaxis Registry of Predominantly Pediatric Patients) of Prehospital Anaphylaxis Treatments (Epinephrine, Antihistamines, and Corticosteroids) (Ann Allergy Asthma Immunol, 2023) [MEDLINE]: n = 5,364
Patients Treated with Prehospital Epinephrine were Less Likely to Have Uncontrolled Reactions (>2 Doses of Epinephrine in the Emergency Department) [Adjusted Odds Ratio 0.955 (95%CI 0.943, 0.967)], Receive Intravenous Fluids in Emergency Department [Adjusted Odds Ratio 0.976 (95% CI: 0.959-0.992)], and to Be Admitted Following the Reaction [Adjusted Odds Ratio 0.964 (95% CI: 0.949-0.980)]
Patients Treated with Prehospital Antihistamines were Less Likely to Have Uncontrolled Reactions (>2 Doses of Epinephrine in the Emergency Department) [Adjusted Odds Ratio 0.978 (95% CI: 0.967-0.989)] and to Be Admitted Following the Reaction [Adjusted Odds Ratio 0.963 (95% CI: 0.949-0.977)]
Patients Who Received Prehospital Corticosteroids were More Likely to Require Intravenous Fluids in the Emergency Department [Adjusted Odds Ratio 1.059 (95% CI: 1.013-1.107)] and Be Admitted [Adjusted Odds Ratio 1.232 (95% CI: 1.181-1.286)]
Residual Pruritus/Urticaria in the Setting of Anaphylaxis, in a Patient Who Has Already Responded Adequately to Epinephrine
Pharmacology
H1-Histamine Receptor Antagonist
Clinical Efficacy
Canadian/Israeli Emergency Department Study (from Cross-Canada Anaphylaxis Registry of Predominantly Pediatric Patients) of Prehospital Anaphylaxis Treatments (Epinephrine, Antihistamines, and Corticosteroids) (Ann Allergy Asthma Immunol, 2023) [MEDLINE]: n = 5,364
Patients Treated with Prehospital Epinephrine were Less Likely to Have Uncontrolled Reactions (>2 Doses of Epinephrine in the Emergency Department) [Adjusted Odds Ratio 0.955 (95%CI 0.943, 0.967)], Receive Intravenous Fluids in Emergency Department [Adjusted Odds Ratio 0.976 (95% CI: 0.959-0.992)], and to Be Admitted Following the Reaction [Adjusted Odds Ratio 0.964 (95% CI: 0.949-0.980)]
Patients Treated with Prehospital Antihistamines were Less Likely to Have Uncontrolled Reactions (>2 Doses of Epinephrine in the Emergency Department) [Adjusted Odds Ratio 0.978 (95% CI: 0.967-0.989)] and to Be Admitted Following the Reaction [Adjusted Odds Ratio 0.963 (95% CI: 0.949-0.977)]
Patients Who Received Prehospital Corticosteroids were More Likely to Require Intravenous Fluids in the Emergency Department [Adjusted Odds Ratio 1.059 (95% CI: 1.013-1.107)] and Be Admitted [Adjusted Odds Ratio 1.232 (95% CI: 1.181-1.286)]
Bronchodilators are Considered an Adjunctive Treatment to Epinephrine Because They Do Not Prevent or Relieve Upper Airway Mucosal Edema or Shock (for which the α1-Adrenergic Effects of Epinephrine are Required)
The Evidence for the Use of β2-Adrenergic Agonists in the Management of Anaphylaxis is Extrapolated from Their Use in the Management of Acute Asthma Exacerbation (see Asthma)
Considerations for Anaphylaxis Management During Pregnancy (see Pregnancy)
During Labor/Delivery, Patient Positioning on Their Left Side, Use of High-Flow Supplemental Oxygen, and Maintenance of a Systolic Blood Pressure ≥90 mm Hg, and Continuous Fetal Monitoring are Recommended (World Allergy Organ J, 2020) [MEDLINE]
Left Lateral Position Minimizes Compression of the Inferior Vena Cava by the Gravid Uterus
Considerations for Refractory Anaphylaxis Management
Other Vasopressors (Ann Allergy Asthma Immunol, 2014) [MEDLINE]
Adrenaline in the treatment of anaphylaxis: what is the evidence? BMJ. 2003;327(7427):1332 [MEDLINE]
Adrenaline in the treatment of anaphylaxis: what is the evidence? BMJ. 2003;327(7427):1332 [MEDLINE]
First-aid treatment of anaphylaxis to food: focus on epinephrine. J Allergy Clin Immunol. 2004;113(5):837 [MEDLINE]
Adequacy of the epinephrine autoinjector needle length in delivering epinephrine to the intramuscular tissues. Ann Allergy Asthma Immunol. 2005;94(5):539 [MEDLINE]
Anaphylaxis: diagnosis and management. Med J Aust. 2006;185(5):283 [MEDLINE]
The management of anaphylaxis in childhood: position paper of the European academy of allergology and clinical immunology. Allergy. 2007;62(8):857 [MEDLINE]
H1-antihistamines for the treatment of anaphylaxis: Cochrane systematic review. Allergy. 2007;62(8):830 [MEDLINE]
Emergency treatment of anaphylaxis. BMJ. 2008;336(7654):1141 [MEDLINE]
Epinephrine: the drug of choice for anaphylaxis. A statement of the World Allergy Organization. Allergy. 2008;63(8):1061 [MEDLINE]
Emergency treatment of anaphylactic reactions–guidelines for healthcare providers. Resuscitation. 2008;77(2):157 [MEDLINE]
Epinephrine auto-injectors: is needle length adequate for delivery of epinephrine intramuscularly? Pediatrics. 2009;124(1):65 [MEDLINE]
Adrenaline for the treatment of anaphylaxis: cochrane systematic review. Allergy. 2009;64(2):204 [MEDLINE]
Epinephrine and its use in anaphylaxis: current issues. Curr Opin Allergy Clin Immunol. 2010;10(4):354 [MEDLINE]
Pharmacologic treatment of anaphylaxis: can the evidence base be strengthened? Curr Opin Allergy Clin Immunol. 2010;10(4):384 [MEDLINE]
Epinephrine and its use in anaphylaxis: current issues. Curr Opin Allergy Clin Immunol. 2010;10(4):354 [MEDLINE]
Confusion about epinephrine dosing leading to iatrogenic overdose: a life-threatening problem with a potential solution. Ann Emerg Med. 2010;55(4):341 [MEDLINE]
Methylene blue and epinephrine: a synergetic association for anaphylactic shock treatment. Crit Care Med. 2013;41(1):195 [MEDLINE]
Methylene blue for the treatment of refractory anaphylaxis without hypotension. Am J Emerg Med. 2013 Jan;31(1):264.e3-5 [MEDLINE]
The level of evidence 5 blues: investigating medicine when experience trumps equipoise. Crit Care Med. 2013 Jan;41(1):359-61 [MEDLINE]
Emergency department diagnosis and treatment of anaphylaxis: a practice parameter. Ann Allergy Asthma Immunol. 2014 [MEDLINE]
Epinephrine in anaphylaxis: higher risk of cardiovascular complications and overdose after administration of intravenous bolus epinephrine compared with intramuscular epinephrine. J Allergy Clin Immunol Pract. 2015;3(1):76 [MEDLINE]
Predictors of Repeat Epinephrine Administration for Emergency Department Patients with Anaphylaxis. J Allergy Clin Immunol Pract. 2015 Jul-Aug;3(4):576-84 [MEDLINE]
Epinephrine use in older patients with anaphylaxis: Clinical outcomes and cardiovascular complications. Resuscitation. 2017;112:53 [MEDLINE]
Patients Taking β-Blockers Do Not Require Increased Doses of Epinephrine for Anaphylaxis. J Allergy Clin Immunol Pract. 2018;6(5):1553 [MEDLINE]
Anaphylaxis Management: Time to Re-Evaluate the Role of Corticosteroids. J Allergy Clin Immunol Pract. 2019;7(7):2239 [MEDLINE]
Evaluation of Prehospital Management in a Canadian Emergency Department Anaphylaxis Cohort. J Allergy Clin Immunol Pract. 2019;7(7):2232 [MEDLINE]
Extracorporeal membrane oxygenation support in refractory perioperative anaphylactic shock to rocuronium: a report of two cases. Perfusion. 2019;34(8):717 [MEDLINE]
Anaphylaxis-a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. J Allergy Clin Immunol. 2020;145(4):1082 [MEDLINE]
World allergy organization anaphylaxis guidance 2020. World Allergy Organ J. 2020;13(10):100472. [MEDLINE]
Use of multiple epinephrine doses in anaphylaxis: A systematic review and meta-analysis. J Allergy Clin Immunol. 2021;148(5):1307 [MEDLINE]
Emergency treatment of anaphylaxis: concise clinical guidance. Clin Med (Lond). 2022;22(4):332 [MEDLINE]
Multi-phasic life-threatening anaphylaxis refractory to epinephrine managed by extracorporeal membrane oxygenation (ECMO): A case report. Front Allergy. 2022;3:934436 [MEDLINE]
Extracorporeal membrane oxygenation support in refractory anaphylactic shock after bee stings: A case report. Perfusion. 2023;38(6):1308 [MEDLINE]
A case report of gadopentetate dimeglumine-induced cardiac arrest: Resuscitation using extracorporeal membrane oxygenation. Ann Noninvasive Electrocardiol. 2023;28(3):e13039 [MEDLINE]
Ann Allergy Asthma Immunol. Published online September 7, 2023. doi:10.1016/j.anai.2023.08.606 [MEDLINE]
Anaphylaxis: A 2023 practice parameter update. Ann Allergy Asthma Immunol. 2024;132(2):124 [MEDLINE]
Timing of repeat epinephrine to inform paediatric anaphylaxis observation periods: a retrospective cohort study. Lancet Child Adolesc Health 2025; 9:484 [MEDLINE]
Rescuing Protamine Anaphylaxis Refractory to Adrenaline Using Extracorporeal Membrane Oxygenation. JACC Case Rep. 2025;30(6 Pt 1):102966 [MEDLINE]