Anaphylaxis is an Acute (and Potentially Fatal) Systemic Hypersensitivity Reaction Caused by the Sudden Release of Mast Cell Inflammatory Mediators (see Immune Hypersensitivity) (World Allergy Organ J, 2020) [MEDLINE]
Anaphylaxis Most Commonly Results from Immunoglobulin E (IgE)-Mediated Reactions to Foods, Medications, and Insect Stings
However, Any Agent Capable of Inciting a Sudden, Systemic Mast Cell Degranulation Can Induce Anaphylaxis (Clin Rev Allergy Immunol, 2018) [MEDLINE]
Basophils May Play a Role in Human Anaphylaxis, Although Their Clinical Significance is Not Well-Differentiated from that of Mast Cells (Which are Activated Concomitantly in Most Cases of Anaphylaxis)
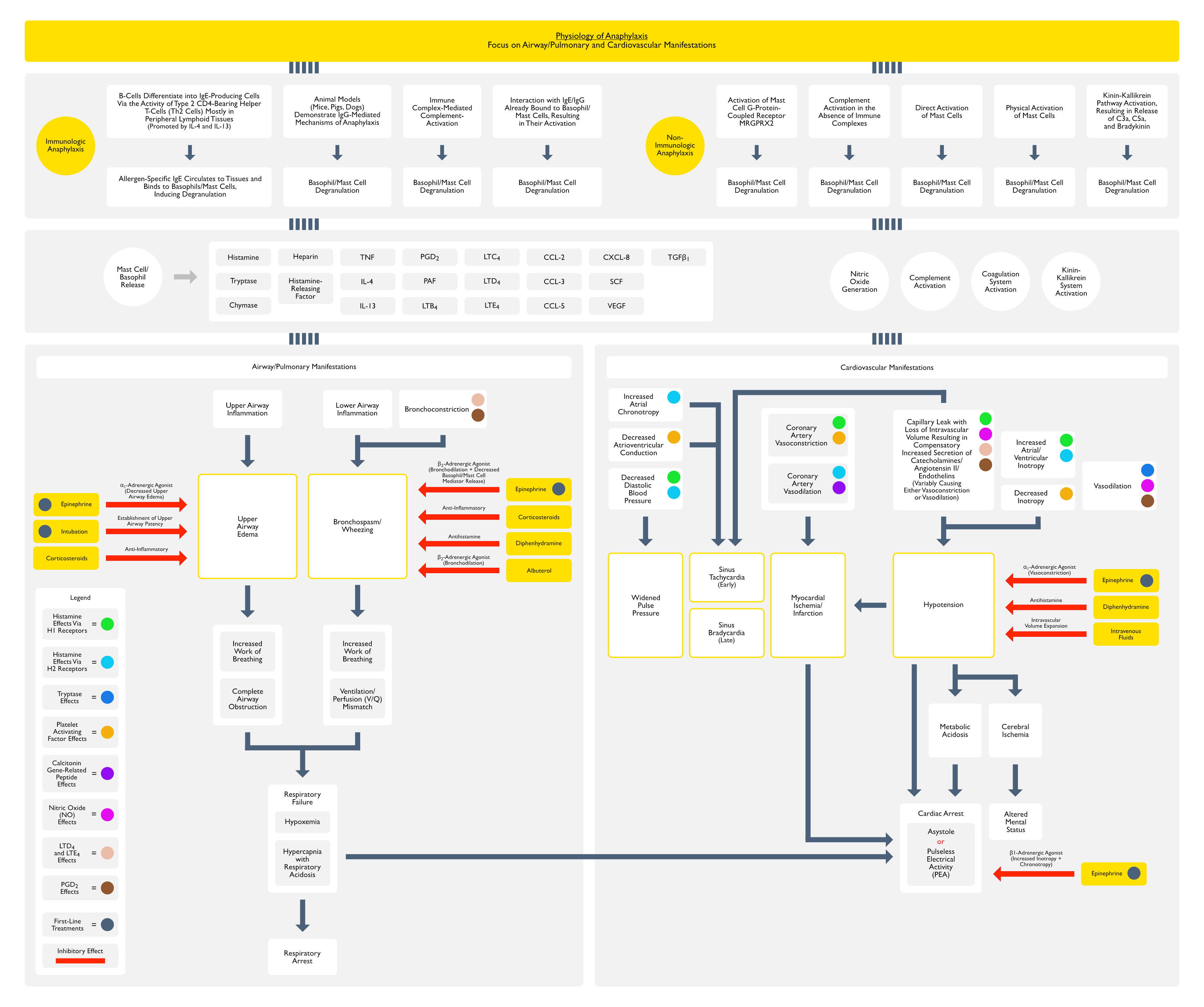
Inflammatory Mediators
Preformed Substances in Mast Cell/Basophil Intracellular Granules
Chymase
Heparin
Histamine
Tryptase
Tryptase is a Protease Which is Abundant in Human Mast Cells (Basophils and Myeloid Precursors Also Contain a Small Amount of Tryptase)
Causes Blood Clotting and Clot Lysis, Possibly Contributing to the Development of Disseminated Intravascular Coagulation (DIC) in Severe Anaphylaxis
Kallikrein-Kinin Contact System
Possibly Contributing to the Development of Disseminated Intravascular Coagulation (DIC) in Severe Anaphylaxis
Physiologic Effects of Platelet Activating Factor (PAF) (Novartis Found Symp, 2004) [MEDLINE]
Decreased Coronary Blood Flow
Delayed Atrioventricular Conduction
Negative Inotropy
Physiologic Effects of Nitric Oxide (NO)
Vasodilation (Potent)
Nitric Oxide (NO) Has Been Implicated in Hypotension in the Setting of Anaphylaxis and Sepsis (see Sepsis)
Increased Vascular Permeability
Protective Responses
Bronchodilation
Coronary Artery Vasodilation
Decreased Histamine Release
Physiologic Effects of Arachidonic Acid Metabolites
PGD2 Causes Vasodilation, Increased Vascular Permeability, and Bronchoconstriction
Leukotriene B4 is a Chemotactic Agent
Leukotriene C4 Enhances Mast Cell Degranulation
Leukotrienes D4 and E4 Increase Microvascular Permeability and are Potent Bronchoconstrictors
Physiologic Effects of Calcitonin Gene-Related Peptide (CGRP)
Calcitonin Gene-Related Peptide (CGRP) is a Sensory Neurotransmitter Widely Distributed in Cardiovascular Tissues and Released During Anaphylaxis
Calcitonin Gene-Related Peptide (CGRP) May Function May Help to Counteract Coronary Artery Vasoconstriction During Anaphylaxis (Naunyn Schmiedebergs Arch Pharmacol, 1997) [MEDLINE]
Calcitonin Gene-Related Peptide (CGRP) Relaxes Vascular Smooth Muscle and Has Cardioprotective Effects in Animal Models of Anaphylaxis (Naunyn Schmiedebergs Arch Pharmacol, 2003) [MEDLINE]
Physiologic Mechanisms of Anaphylaxis
Factors Which Amplify Anaphylaxis
Acute Infection
Disruption of Routine
Travel
Emotional Stress
Exercise
Exercise is the Best Characterized Amplifying Factor
Exercise is Commonly Associated with Anaphylaxis Due to Concomitant Ingestion of a Specific Food Trigger
Celery
Omega-5 Gliadin
Shellfish
Wheat
Exercise is Less Commonly Associated with Anaphylaxis Due to Concomitant Ingestion of Ethanol or Nonsteroidal Anti-Inflammatory Drug (NSAID)
These Agents Enhance Intestinal Permeability and Allergen Absorption
Premenstrual Status
Anaerobic Metabolism Occurs in the Setting of Anaphylaxis
During Anaphylaxis, Blood Flow to the Periphery is Decreased to Preserve Perfusion of the Central Organs (Brain, Heart, and Kidneys), Resulting in Anaerobic Metabolism within Peripheral Tissues
This is Similar to Other Types of Distributive Shock, Although the Mechanism May Be Different
In Septic Shock, Decreased Systemic Vascular Resistance (SVR) Results in Hypotension
Impaired Skeletal Muscle Oxygen Consumption (Despite an Increased Partial Pressure of Oxygen), Resulting in Anaerobic Metabolism and “Cytopathic Hypoxia” (Crit Care, 2002) [MEDLINE]
Study of a Rat Model of Ovalbumin-Induced Anaphylaxis vs Nicardipine-Induced Hypotension (Anesthesiology, 2005) [MEDLINE]
The Time Course and Magnitude to Hypotension were Similar and Both Groups Manifested Decreased Skeletal Muscle Perfusion
However, Anaphylactic Rats Manifested Greater Sympathetic Nervous System Activation (with Higher Plasma Catecholamine Levels at 20 min, Which were Maintained Throughout the 60 min Protocol)
Plasma Epinephrine Levels Increased 15-Fold and Norepinephrine Levels Increased 10-Fold Over Baseline Values in the Anaphylactic Rats
Skeletal Muscle Blood Flow was Decreased in Both the Anaphylaxis-Induced Hypotension and Nicardipine-Induced Hypotension Rats Initially, Which was Then Followed by a Further Decrease in the Anaphylaxis Group Beginning at 20 min and Persisting for the Duration of the Protocol
In the Anaphylactic Rats, a Higher Gradient Between Plasma and Interstitial Epinephrine Indicated More Impaired Skeletal Muscle Blood Flow (Possibly Due to Greater Skeletal Muscle Vasoconstriction)
Anaphylactic Rats Manifested a More Rapid Increase in Interstitial Lactate Levels and a Corresponding Decrease in Interstitial Pyruvate Levels, Indicating Depletion of Cellular Energy Stores (This Finding was Not Observed in the NIcardipine-Induced Hypotension Rats)
These Findings Suggest that Skeletal Muscle Maintains High Rates of Oxygen Utilization During Anaphylaxis (as Compared to Other Types of Distributive Shock) and This Combined with Decreased Perfusion Leads to Rapid Development of Anaerobic Metabolism (Possibly Explaining Why End-Organ Injury and Irreversible Shock Develop So Rapidly in the Setting of Anaphylaxis)
Anaphylaxis Has Historically Been Considered a Type of Distributive Shock Characterized by Profound Venodilation (Similar to Septic Shock and Toxic Shock Syndrome)
However, an Emerging View is that Anaphylaxis Has Clinical Features of Hypovolemic Shock Also (i.e. Fluid Extravasation Causing Decreased Venous Return Combined with Myocardial Depression) (Immunol Allergy Clin North Am, 2007) [MEDLINE]
Physiologic/Clinical Features
Anaphylaxis Causes Increased Vascular Permeability, Resulting in Massive Fluid Shifts and Hypovolemia
As Much as 35% of Intravascular Volume Can Shift to the Extravascular Space within 10 min During Anaphylaxis (Anaesth Intensive Care, 1986) [MEDLINE]
Compensatory Responses Resulting in Vasoconstriction
Release of Endogenous Catecholamines
Release of Angiotensin II
Release of Endothelins
However, Despite These Compensatory Responses, Some Patients Experience Persistent Shock (Due to Hypovolemia) and/or Persistent Shock Due to Vasodilation/Decreased Systemic Vascular Resistance (for Unclear Reasons)
Serum Tryptase Level Should Be Drawn within 3 hrs of the Event to Diagnose Anaphylaxis
Although Tryptase Levels Do Not Guide Acute Anaphylaxis Management, Their Assessment During Follow-Up May Be Useful (Ann Allergy Asthma Immunol, 2024) [MEDLINE]
Serum Tryptase Level May Not Be Elevated in Some Cases
RAST Testing
Useful for Allergy Testing: detects allergen-specific IgE
National Institute of Allergy and Infectious Disease (NIAID) and Food Allergy and Anaphylaxis Network (FAAN) Diagnostic Criteria (One of Three Following Criteria) (J Allergy Clin Immunol, 2006) [MEDLINE]
Criterion 1: Acute Onset of Illness (Within Min-Several Hours) with Skin/Mucosal Tissue Involvement (Flushing/Generalized Erythema, Hives, Pruritus, Swollen Lips/Tongue/Uvula) and At Least One of the Following
Criterion 3: Hypotension After Exposure to a Known Allergen for a Specific Patient Within Min-Several Hours (see Hypotension)
Adult
Systolic Blood Pressure 90 mm Hg or >30% in systolic blood pressure from patient’s baseline
Infant/Children
Age-Specific Hypotension or >30% Decrease in Systolic Blood Pressure
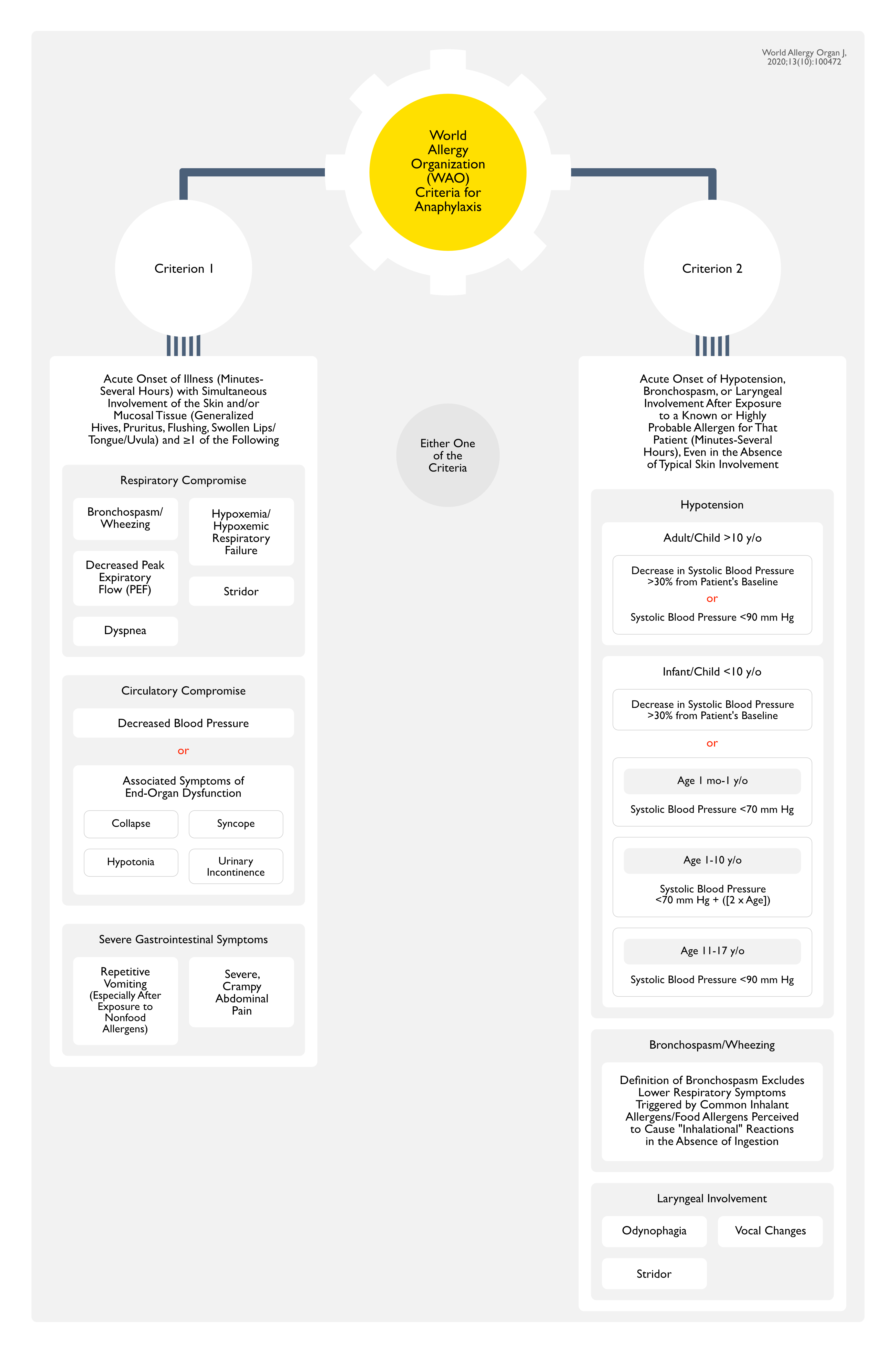
World Allergy Organization (WAO) Criteria for Anaphylaxis (World Allergy Organ J, 2020) [MEDLINE]
General Comments
Anaphylaxis is Highly Likely When Either One of the Following Two Criteria is Fulfilled
Criterion 1: Acute Onset of Illness (Minutes-Several Hours) with Simultaneous Involvement of the Skin and/or Mucosal Tissue (Generalized Hives, Pruritus, Flushing, Swollen Lips/Tongue/Uvula) and ≥1 of the Following
Criterion 2: Acute Onset of Hypotension, Bronchospasm, or Laryngeal Involvement After Exposure to a Known or Highly Probable Allergen for That Patient (Minutes-Several Hours), Even in the Absence of Typical Skin Involvement
Hypotension
Adult/Child >10 y/o
Decrease in Systolic Blood Pressure >30% from Patient’s Baseline or Systolic Blood Pressure <90 mm Hg
Infant/Child <10 y/o
Decrease in Systolic Blood Pressure >30% from from Patient’s Baseline or
Definition of Bronchospasm Excludes Lower Respiratory Symptoms Triggered by Common Inhalant Allergens/Food Allergens Perceived to Cause “Inhalational” Reactions in the Absence of Ingestion
IgE-Mediated Anaphylaxis Generally Develops Between Minutes-1 Hour of Exposure to the Trigger
However, Rarely, IgE-Mediated Anaphylactic Reactions Can Occur with a Longer Latency
For Example, IgE-Mediated Anaphylactic Reactions to the Carbohydrate Galactose α-1,3-Galactose (Alpha-Gal) in Red Meat Develop 4-6 hrs After Ingestion (J Allergy Clin Immunol, 2009) [MEDLINE]
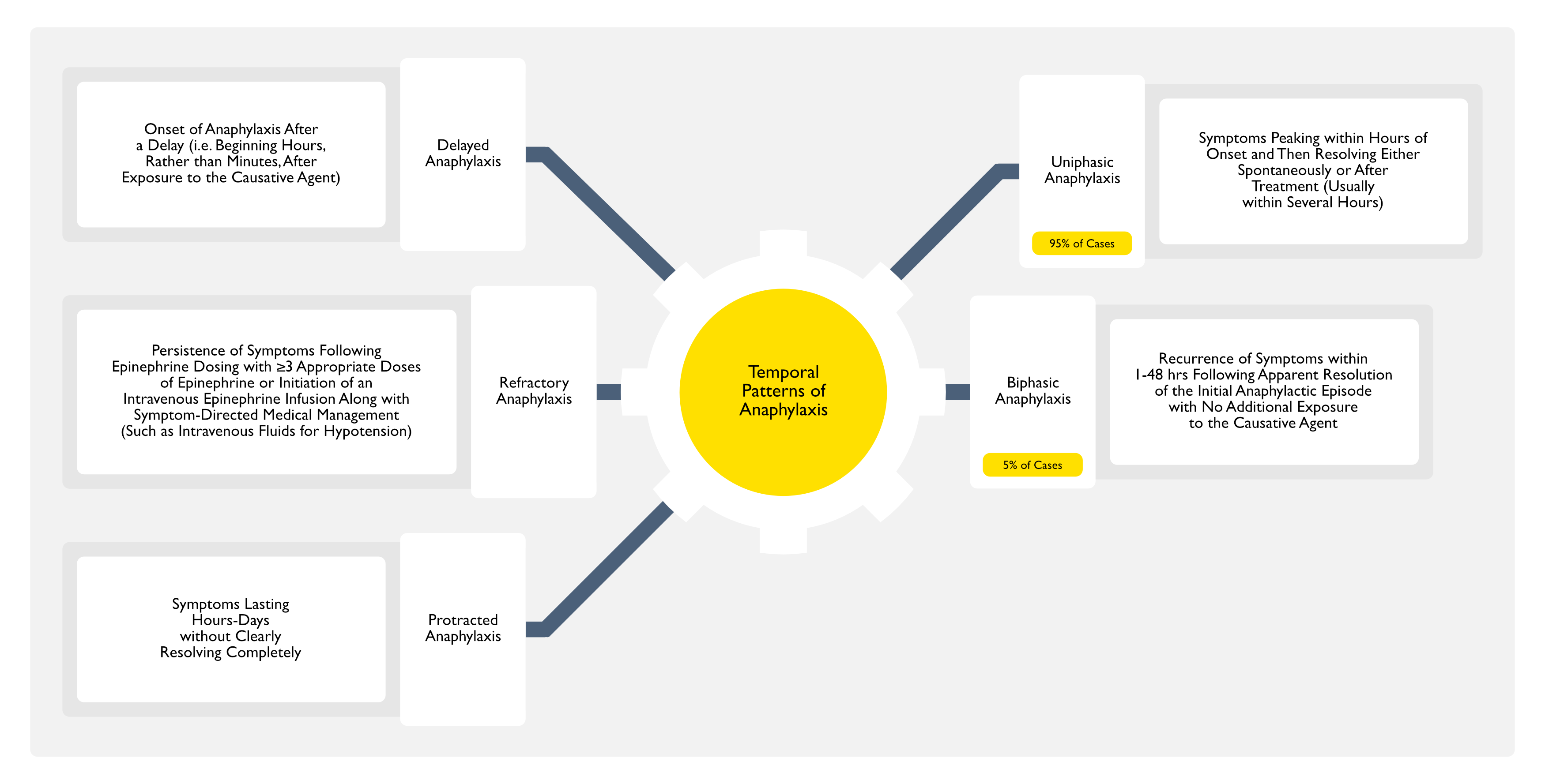
Anaphylaxis is Usually Characterized by a Defined Exposure to a Potential Etiology, Followed Usually within Seconds-Minutes (But Rarely Up to Hours Later) by Rapid Onset, Evolution, and Ultimate Resolution of Symptoms/Signs
Uniphasic Anaphylaxis
Most Common Type (95% of Anaphylaxis Cases)
Uniphasic Anaphylaxis Typically Peaks within Hours After Symptom Onset and Then Either Resolves Spontaneously or After Treatment, Usually within Several Hours (J Allergy Clin Immunol Pract, 2015) [MEDLINE] (J Allergy Clin Immunol Pract, 2020) [MEDLINE]
Biphasic Anaphylaxis
Biphasic Reactions Occur in Approximately 5% of Anaphylaxis Cases
Biphasic Anaphylaxis is Defined as a Recurrence of Anaphylaxis Symptoms within 1-48 hrs Following the Apparent Resolution of the Initial Anaphylactic Episode with No Additional Exposure to the Causative Agent (J Allergy Clin Immunol, 2020) [MEDLINE]
Recurrent Symptoms Typically Occur within 12 hrs After Resolution of the Initial Symptoms
Delayed Time to First Epinephrine Treatment (>60 min)
Need for >1 Dose of Epinephrine
Unclear Risk Factors
Unknown Trigger for Anaphylaxis
Possible Ongoing Exposure to Trigger for Anaphylaxis (Such as Sustained-Release/Depot Medication, Food, etc)
Prolonged Interval (i.e. Hours) Between COntact with Trigger and Onset of Anaphylaxis Symptoms
Treatment with Antihistamines/Glucocorticoids without Epinephrine
In Patients with Risk Factors for Biphasic Anaphylaxis, a Prolonged Observation May Be Required (and Corticosteroids are Often Useful to Blunt the Development of the Second Phase)
Protracted Anaphylaxis
Protracted/Persistent Anaphylaxis is Defined as Anaphylaxis Lasting Hours-Days without Clearly Resolving Completely
Refractory Anaphylaxis
Refractory Anaphylaxis is Defined as the Persistence of Anaphylaxis Following Appropriate Epinephrine Dosing with ≥3 Appropriate Doses of Epinephrine or Initiation of an Intravenous Epinephrine Infusion along with Symptom-Directed Medical Management (Such as Intravenous Fluids for Hypotension) (J Allergy Clin Immunol, 2020) [MEDLINE]
Delayed Anaphylaxis
Delayed Anaphylaxis is Defined as the Onset of Anaphylaxis After a Delay (i.e. Beginning Hours Rather than Minutes After Exposure to the Causative Agent) (Allergol Int, 2016) [MEDLINE]
Example: Alpha-Gal Syndrome
Range of Anaphylaxis Severity
Anaphylaxis is Highly Unpredictable
Anaphylaxis May Resolve Spontaneously (Due to Production of Compensatory Mediators, Sich as Epinephrine, Angiotensin II, Endothelins) or May Progress within Minutes to Respiratory Failure/Cardiovascular Collapse/Death (J Allergy Clin Immunol, 2006) [MEDLINE]
Because the Prediction of Anaphylaxis Course is Not Possible, Early Epinephrine Administration is Critical to Prevent Life-Threatening Manifestations
Latency Between Onset of Symptoms and Respiratory Arrest/Cardiac Arrest (Clin Exp Allergy, 2000) [MEDLINE]: n = 164
Medication/Radiographic Contrast-Induced Anaphylaxis: latency = 5 min
Insect Venom-Induced Anaphylaxis: latency = 15 min
Food-Induced Anaphylaxis: latency = 30 min
Nocturnal Anaphylaxis
A Small Number of Allergens Can Cause Primarily Nocturnal Anaphylaxis (Awakening a Patient from Sleep)
Anaphylactic Reactions to the Carbohydrate Galactose α-1,3-Galactose (Alpha-Gal) in Red Meat (Beef, Pork, Lamb) Develop 4-6 hrs After Ingestion (J Allergy Clin Immunol, 2009) [MEDLINE]
Allergens in the Saliva of Kissing Bugs Which Typically Bite During the Night
Allergens in the Bites of Pigeon Ticks (Argas Reflexus), Which Feed at Night (Eur Ann Allergy Clin Immunol, 2005) [MEDLINE] (Ann Agric Environ Med, 2006) [MEDLINE] (Eur J Dermatol, 2010) [MEDLINE] (Allergy, 2018) [MEDLINE]
Mostly Encountered in Middle/Southern European Cities Where Pigeons are Prevalent
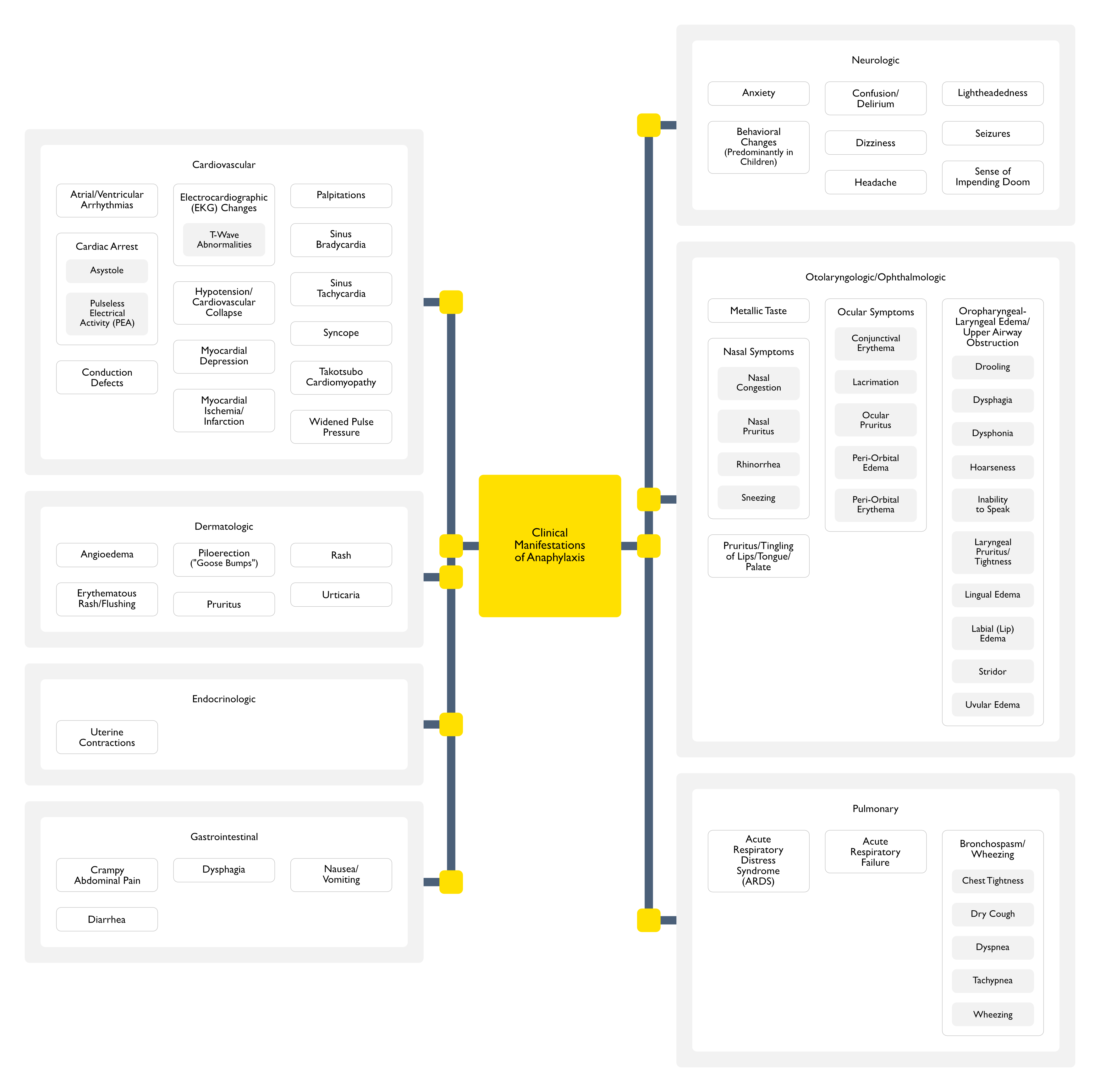
Cardiovascular Manifestations
General Comments
Cardiovascular Manifestations Occur in 45% of Anaphylaxis Cases
Arrhythmias
Epidemiology
Atrial/Ventricular Arrhythmias Have Been Reported in the Setting of Anaphylaxis (Novartis Found Symp, 2004) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2014) [MEDLINE]
Conduction Defects Have Been Reported in the Setting of Anaphylaxis (Novartis Found Symp, 2004) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2014) [MEDLINE]
As Much as 35% of Intravascular Volume Can Shift to the Extravascular Space within 10 min During Anaphylaxis (Anaesth Intensive Care, 1986) [MEDLINE]
In a Retrospective Series Examining the Contribution of Body Posture to Prehospital Fatality in the Setting of Anaphylaxis, 4/10 Patients were Associated with Upright/Sitting Posture (Autopsy Findings Confirmed Pulseless Electrical Activity and an “Empty Ventricle” Attributed to Inadequate Venous Return Secondary to Vasodilation and Decreased Intravascular Volume) (J Allergy Clin Immunol, 2003) [MEDLINE]
Venodilation
Anaphylaxis Has Historically Been Considered a Type of Distributive Shock Characterized by Profound Venodilation (Similar to Septic Shock and Toxic Shock Syndrome)
However, an Emerging View is that Anaphylaxis Also Has Clinical Features of Hypovolemic Shock (i.e. Fluid Extravasation Causing Decreased Venous Return Combined with Myocardial Depression) (Immunol Allergy Clin North Am, 2007) [MEDLINE]
Variable Systemic Vascular Resistance (SVR)
In Response to Loss of Intravascular Volume, Catecholamines/Angiotensin II/Endothelins are Released in a Compensatory Manner to Facilitate Vasoconstriction
Despite the Compensatory Release of Endogenous Catecholamines/Angiotensin II/Endothelins, Some Patients Experience Persistent Shock (Due to Hypovolemia) and/or Persistent Shock Due to Vasodilation/Decreased Systemic Vascular Resistance (for Unclear Reasons)
Myocardial Depression
Myocardial Depression
Epidemiology
Anaphylaxis Has Been Reported to Cause Myocardial Depression (Lancet, 1988) [MEDLINE]
Reported Cases were Severe Enough to Require Inotropic/Mechanical Support
Physiology
Histamine Acting at the H2 Histamine Receptor Causes Increased Atrial and Ventricular Inotropy
In Animal Models, Histamine Acting at the H3 Receptor Appears to Mediate Myocardial Depression (Am J Respir Crit Care Med, 1999) [MEDLINE]
Platelet-Activating Factor (PAF) Has Negative Inotropic Effects (Novartis Found Symp, 2004) [MEDLINE]
Coronary Artery Vasospasm, Severe Enough to Cause Myocardial Infarction (i.e. Kounis Syndrome) Has Been Reported in the Setting of Anaphylaxis (Int J Cardiol, 2006) [MEDLINE] (Clin Ther, 2013) [MEDLINE] (Rev Port Cardiol, 2016) [MEDLINE]
Platelet-Activating Factor (PAF) Induces Platelet Aggregation and Coagulation Pathway Activation (Which Might Predispose to Coronary Artery Thrombosis)
Calcitonin Gene-Related Peptide (CGRP, Which is a Sensory Neurotransmitter Widely Distributed in Cardiovascular Tissues, is Released During Anaphylaxis, and Causes Coronary Vasodilation (Naunyn Schmiedebergs Arch Pharmacol, 1997) [MEDLINE] (Naunyn Schmiedebergs Arch Pharmacol, 2003) [MEDLINE]
Mast Cells Accumulate at Sites of Coronary Atherosclerotic Plaques, and Mast Cell Degranulation May Promote Plaque Rupture During Both Acute myocardial Events and During Anaphylaxis
Some Anaphylaxis Patients Present with Bradycardia/Relative Bradycardia (i.e. Initial Tachycardia, Followed by a Decrease in Heart Rate, Despite Worsening Hypotension)
This Observation Has Been Reported in the Setting of Experimentally-Induced Insect Sting Anaphylaxis, as Well as in Trauma Patients (J Clin Invest, 1980) [MEDLINE] (Ann Intern Med, 1993) [MEDLINE] (J Trauma, 1998) [MEDLINE] (Emerg Med J, 2004) [MEDLINE]
Physiology
Phasic Response of Heart Rate in the Setting of Anaphylaxis (Data from Animal Models) (Am J Physiol, 1991) [MEDLINE]
Initial Response to Hypovolemia is a Baroreceptor-Mediated Increase in Cardiac Sympathetic Drive and Concomitant Withdrawal of Resting Vagal Drive, Which Together Produce Sinus Tachycardia and Peripheral Vasoconstriction
When the Effective Arterial Blood Volume Falls by 20-30%, a Second Phase Occurs with Withdrawal of the Vasoconstrictor Drive, Absolute/Relative Bradycardia, Increased Vasopressin, Further Catecholamine Release (Due to Increased Adrenal Axis Output), and Hypotension
Hypotension in this Setting is Independent of the Bradycardia Since it Persists Even if the Bradycardia is Reversed with Atropine
Bradycardia Has Also Been Observed in Porcine Anaphylaxis Models (Am J Physiol Heart Circ Physiol, 2006) [MEDLINE]
In this Model, Release of the Anaphylatoxin C5a and Adenosine Acting Via A1 Adenosine Receptors are Believed to Play a Role
Excessive Venous Pooling with Decreased Venous Return (Also Seen in Vasodepressor Reactions) May Activate Tension-Sensitive Sensory Receptors in the Inferoposterior Portions of the Left Ventricle
This Results in a Cardioinhibitory (Bezold-Jarisch) Reflex Which Stimulates the Vagus Nerve and Causes Bradycardia
Although the Clinical Implications of Anaphylaxis-Associated Bradycardia Have Not Been Studied, Trauma-Associated Bradycardia is Associated with a Decreased Mortality Rate (After Adjustment for Other Risk Factors) (J Trauma, 1998) [MEDLINE]
However, some Anaphylaxis Patients Present with Bradycardia/Relative Bradycardia (i.e. Initial Tachycardia, Followed by a Decrease in Heart Rate, Despite Worsening Hypotension)
This Observation Has Been Reported in the Setting of Experimentally-Induced Insect Sting Anaphylaxis, as Well as in Trauma Patients (J Clin Invest, 1980) [MEDLINE] (Ann Intern Med, 1993) [MEDLINE] (J Trauma, 1998) [MEDLINE] (Emerg Med J, 2004) [MEDLINE]
Physiology
Mechanisms
Mechanisms
Chronotropic Effects of Endogenous Catecholamines
Intravascular Volume Depletion
Phasic Response of Heart Rate in the Setting of Anaphylaxis (Data from Animal Models) (Am J Physiol, 1991) [MEDLINE]
Initial Response to Hypovolemia is a Baroreceptor-Mediated Increase in Cardiac Sympathetic Drive and Concomitant Withdrawal of Resting Vagal Drive, Which Together Produce Sinus Tachycardia and Peripheral Vasoconstriction
When the Effective Arterial Blood Volume Falls by 20-30%, a Second Phase Occurs with Withdrawal of the Vasoconstrictor Drive, Absolute/Relative Bradycardia, Increased Vasopressin, Further Catecholamine Release (Due to Increased Adrenal Axis Output), and Hypotension
Hypotension in this Setting is Independent of the Bradycardia Since it Persists Even if the Bradycardia is Reversed with Atropine
Histamine Acting at Both H1 and H2 Histamine Receptors Results in Decreased Diastolic Pressure and Increased Pulse Pressure
Dermatologic Manifestations
General Comments
Dermatologic and Mucosal Manifestations Occur in 90% of Anaphylaxis Cases
Dermatologic Symptoms/Signs May Be Missed in Patients Who Has Taken an H1 Antihistamine, if the Patient Cannot Describe Pruritus, or if the Patient is Not Undressed and Fully Examined During the Episode (or in Patients Who are Draped During Surgery)
Study of Activity of Enzymes Involved in Bradykinin Catabolism in Predicting Anaphylaxis to Peanuts/Tree Nuts from a Regional Allergy Center (J Allergy Clin Immunol, 2008) [MEDLINE]: n = 122 (46 patients had moderate-to-severe pharyngeal edema, 36 patients had moderate-severe bronchospasm, and the remainder lacked these symptoms)
Patients with Severe Pharyngeal Edema Had Significantly Low Serum Angiotensin Converting Enzyme (ACE) Levels than Those with No Pharyngeal Edema
In Multivariate Analysis, Patients with Serum Angiotensin Converting Enzyme (ACE) Levels in the Lowest Quartile Had a 9.6-Fold Increased Risk of Severe Pharyngeal Edema, as Compared to Those Patients with Higher Serum Angiotensin Converting Enzyme (ACE) Levels
However, Patients with Serum Angiotensin Converting Enzyme (ACE) Levels in the Lowest Quartile were No More Likely than Others to Have Decreased Consciousness, Bronchospasm, or Urticaria
Serum Aminopeptidase P Levels Did Not Correlate with Clinical Severity or Demonstrate Any Statistical Trends
These Findings Suggest that Patients Who Experience Angioedema During Anaphylaxis Might Be More Resistant to Treatment with Epinephrine and Second-Line Therapies (Atihistamines, Glucocorticoids)
Study of Anaphylaxis Fatalities (Curr Opin Allergy Clin Immunol, 2004) [MEDLINE]: n = 196
Asphyxia was the Cause of Death in Approximately 50% of the Cases (Of These, Lower Airways/Bronchospasm) Accounted for 50%, Upper Airway Angioedema Accounted for 24%, and Both Upper and Lower Airway Involvement Accounted for 26%)
The Fatalities from Acute Bronchospasm During Anaphylaxis Occurred Almost Exclusively in Those with Preexisting Asthma
Case Series of Anaphylaxis Fatalities (Ann Allergy Asthma Immunol, 2007) [MEDLINE]: n = 23
16 of 20 Immediate Deaths (within 1 hr of Symptom Onset) were Due to Upper Airway Edema
Pruritus/Tingling of Lips/Tongue/Palate
Epidemiology
XXX
Pulmonary Manifestations
General Comments
Pulmonary Manifestations Occur in 85% of Anaphylaxis Cases
In Retrospective Series of Acute Nonfatal Anaphylaxis
Respiratory Symptoms/Signs Occur in 40-60% of Patients
Study of Anaphylaxis Fatalities (Curr Opin Allergy Clin Immunol, 2004) [MEDLINE]: n = 196
Asphyxia was the Cause of Death in Approximately 50% of the Cases (Of These, Lower Airways/Bronchospasm) Accounted for 50%, Upper Airway Angioedema Accounted for 24%, and Both Upper and Lower Airway Involvement Accounted for 26%)
The Fatalities from Acute Bronchospasm During Anaphylaxis Occurred Almost Exclusively in Those with Preexisting Asthma
Nearly All Patients with Fatal Anaphylaxis are Known to Have ≥1 Allergic Conditions or were Clearly Atopic by Retrospectively-Gathered Medical History (Novartis Found Symp, 2004) [MEDLINE]
However, Drug/Venom Associated Anaphylaxis Typically Affects Non-Atopic Patients
Asthma is Probably the Single Most Important Risk Factor for Fatal Food-Associated Anaphylaxis
In a 10 Year Series of Patients in the United Kingdom, All Fatal Food-Related Anaphylaxis Cases Occurred in Patients Taking Daily Medications for Asthma (Novartis Found Symp, 2004) [MEDLINE]
In Another Series of 32 Food-Related Anaphylaxis Cases, All But One Patient Had Asthma (J Allergy Clin Immunol, 2001) [MEDLINE]
Drug/Venom-Associated Anaphylaxis
Asthma is Also Common Among Victims of Drug/Venom-Induced Anaphylaxis, Although the Correlation is Not as Strong as that for Food (Novartis Found Symp, 2004) [MEDLINE] (J Investig Allergol Clin Immunol, 2021) [MEDLINE]
It is Unclear if Asthma Control Decreases the Risk of Fatal Anaphylaxis
Most Anaphylaxis Series Have Not Reported the Status of Asthma Control at the Time of Fatal Anaphylaxis, But This Series Implies that at Least Some Patients Have Poor Asthma Control (Novartis Found Symp, 2004) [MEDLINE]
In Contrast, One Study of 13 Near-Fatal/Fatal Food-Associated Anaphylaxis Cases Reported that 12 Patients Had Asthma that was Well-Controlled (NEJM, 1992) [MEDLINE]
Mediators Released from Immunologically Activated Human Heart Mast Cells Strongly Influence Ventricular Function, Cardiac Rhythm and Coronary Artery Tone
Histamine, Cysteinyl Leukotrienes and Platelet-Activating Factor (PAF) Exert Negative Inotropic Effects and Induce Myocardial Depression Which Contribute Significantly to the Pathogenesis of Anaphylactic Shock
Moreover, Cardiac Mast Cells Release Chymase and Renin Which Activates the Angiotensin System Locally (Resulting in Further induces Arteriolar Vasoconstriction)
The Number and Density of Cardiac Mast Cells is Increased in Patients with Ischemic Heart Disease and Dilated Cardiomyopathies
This Observation May Help Explain Why These Conditions are Major Risk Factors for Fatal Anaphylaxis
Antidepressants Can Impair the Ability to Recognize Anaphylaxis Triggers and Symptoms
Tricyclic Antidepressants (TCA’s) May Increase the Adverse Effects of Epinephrine Due to Inhibition of Epinephrine Uptake at Adrenergic Receptors (see Tricyclic Antidepressants)
Monoamine Oxidase (MAO) Inhibitors Potentiate Epinephrine Effects by Inhibiting its Metabolism by Monoamine Oxidase (see Monoamine Oxidase Inhibitors)
α-Blockers May Decrease the Effects of Endogenous or Exogenous Epinephrine at α-Adrenergic Receptors, Potentially Making Anaphylaxis Less Responsive to the α-Adrenergic Effects of Epinephrine (Aust Fam Physician, 1998) [MEDLINE]
Angiotensin Converting Enzyme (ACE) Inhibitors Impair the Ability to Degrade Tryptase, Histamine, and Bradykinin
Angiotensin Converting Enzyme (ACE) Inhibitors Block the Effect of Angiotensin, Potentially Interfering with Endogenous Compensatory Mechanisms, Resulting in More Severe or Prolonged Anaphylaxis Symptoms (J Allergy Clin Immunol, 2009) [MEDLINE]
Concomitant β-Blocker and ACE Inhibitor Use May Synergistically Increase the Risk of Severe Anaphylaxis (J Allergy Clin Immunol, 2015) [MEDLINE]
Angiotensin II Receptor Blockers (ARB’s) are Less Likely to Have This Effect (J Allergy Clin Immunol, 2010) [MEDLINE]
Angiotensin Receptor Blockers (ARB’s) May Interfere with Endogenous Compensatory Responses
Antidepressants
Antidepressant Use May Impair the Ability to Recognize Anaphylaxis Triggers and Symptoms
Tricyclic Antidepressants (TCA’s) May Increase the Adverse Effects of Epinephrine Due to Inhibition of Epinephrine Uptake at Adrenergic Receptors (see Tricyclic Antidepressants)
Monoamine Oxidase (MAO) Inhibitors Potentiate Epinephrine Effects by Inhibiting its Metabolism by Monoamine Oxidase (see Monoamine Oxidase Inhibitors)
Antihypertensives
Use of Antihypertensives in Aggregate (β-Blockers, ACE Inhibitors, Calcium Channel Blockers, Angiotensin Receptor Blockers, and/or Diuretics) Has Been Associated with Increased Anaphylaxis-Associated Organ System Involvement and Increased Risk of Hospital Admission (Independent of Age, Sex, Suspected Etiology, or Presence of Preexisting Lung Disease) (J Allergy Clin Immunol, 2013) [MEDLINE]
Oral/Ophthalmologic β-Blocker Use May Potentially Make Anaphylaxis More Difficult to Treat by Causing Unopposed α-Adrenergic Effects (with Hypertension) and Decreased Bronchodilator Responsiveness to the β-Adrenergic Effects of Endogenous/Exogenous Epinephrine (J Allergy Clin Immunol, 2004) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2007) [MEDLINE]
Concomitant β-Blocker and Angiotensin Converting Enzyme (ACE) Inhibitor Use May Synergistically Increase the Risk of Severe Anaphylaxis (J Allergy Clin Immunol, 2015) [MEDLINE]
However, in a Retrospective Emergency Department Study (n = 789 Patients), Patients Taking β-Blockers were No More Likely to Require Epinephrine or to Require Additional Epinephrine Doses than Patients Not Taking β-Blockers, So the Clinical Impact May Be Relatively Small (J Allergy Clin Immunol Pract, 2018) [MEDLINE]
Due to Impaired Ability to Degrade Tryptase, Histamine, and Bradykinin
Study of Activity of Enzymes Involved in Bradykinin Catabolism in Predicting Anaphylaxis to Peanuts/Tree Nuts from a Regional Allergy Center (J Allergy Clin Immunol, 2008) [MEDLINE]: n = 122 (46 patients had moderate-to-severe pharyngeal edema, 36 patients had moderate-severe bronchospasm, and the remainder lacked these symptoms)
Patients with Severe Pharyngeal Edema Had Significantly Low Serum Angiotensin Converting Enzyme (ACE) Levels than Those with No Pharyngeal Edema
In Multivariate Analysis, Patients with Serum Angiotensin Converting Enzyme (ACE) Levels in the Lowest Quartile Had a 9.6-Fold Increased Risk of Severe Pharyngeal Edema, as Compared to Those Patients with Higher Serum Angiotensin Converting Enzyme (ACE) Levels
However, Patients with Serum Angiotensin Converting Enzyme (ACE) Levels in the Lowest Quartile were No More Likely than Others to Have Decreased Consciousness, Bronchospasm, or Urticaria
Serum Aminopeptidase P Levels Did Not Correlate with Clinical Severity or Demonstrate Any Statistical Trends
These Findings Suggest that Patients Who Experience Angioedema During Anaphylaxis Might Be More Resistant to Treatment with Epinephrine and Second-Line Therapies (Atihistamines, Glucocorticoids)
Due to Impaired Ability to Degrade Platelet-Activating Factor (PAF)
Factors Related to Ineffective Epinephrine Management of Anaphylaxis (J Allergy Clin Immunol, 2004) [MEDLINE]
Delayed/No Epinephrine Administration
The Number of Food and Venom-Allergic Patients Who Do Not Carry Their Prescribed Self-Injectable Epinephrine is Significant
Furthermore, Many of Those Patients Who Do Carry Their Epinephrine are Unable to Self-Administer it Promptly and Correctly in a Panic Situation Because They Have Not Been Instructed in the Proper Use of the Device or Have Not Practiced with a Trainer Device
Early Administration of Epinephrine Appears to Be Critical for Survival After Severe Anaphylaxis
A Series of 13 Near-Fatal/Fatal Food-Induced Anaphylactic Reactions in Children/Adolescents Suggested that Epinephrine is Most Effective When Given in the Initial 30 min of the Reaction (NEJM, 1992) [MEDLINE]
Epinephrine was Administered within this Time Period in 6/7 Children Who Survived, Whereas Only 2/6 Patients Who Died Received Epinephrine within the First 60 min
In the Setting of Anaphylaxis, Delayed Epinephrine Injection is Associated with Increased Risk of Death (BMJ, 2003) [MEDLINE] (Allergy, 2007) [MEDLINE] (BMJ, 2008) [MEDLINE] (Allergy, 2009) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2010) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2010) [MEDLINE]
Several Series Have Demonstrated that Only a Minority of Patients with Fatal Anaphylaxis Receive Epinephrine Promptly or at All (NEJM, 1992) [MEDLINE] (Clin Exp Allergy, 2000) [MEDLINE] (Ann Allergy Asthma Immunol, 2007) [MEDLINE]
A United Kingdom Series of Anaphylaxis-Associated Deaths Occurring from 1992-1998 Found that Only 20% of Patients were Given Epinephrine at Any Point in Their Treatment (Clin Exp Allergy, 2000) [MEDLINE]
Epinephrine Unresponsiveness
Potential Mechanisms of Epinephrine Unresponsiveness
Rapid Anaphylaxis Progression
From Case Reports/Autopsy Data, Epinephrine Does Not Work in Approximately 10% of Anaphylaxis Episodes (Even if Administered Promptly)
Epinephrine Given Late in Course of Anaphylaxis
From Case Reports/Autopsy Data, Role of Late Epinephrine Administration is Difficult to Prove
Inadequate Epinephrine Dose Administered
From Dose-Response Studies
Optimal Epinephrine Dose is Unknown
Based on Tradition, 0.3 mg is Used for Adults in Many Countries (Dose of 0.5 mg is Used in Some Countries)
In Infants/Children, Appropriate Dosing May be Difficult
Suboptimal Route/Site of Epinephrine Administration
Non-Medical Personnel May Lack Speed/Accuracy of Epinephrine Injection
In Obese Patients, Intramuscular Injection of Epinephrine May Inadvertently End Up Being a Subcutaneous Injection Unless a Needle ≥2.5 cm (1 in) is Used to Penetrate the Fat Pad Over the Vastus Lateralis Muscle
Use of an Expired Epinephrine Injector Device
Epinephrine Content is Inversely Related to the Number of Months Past the Expiration Date of an Epinephrine Injector Device
Use of Medications Which Might Interfere with Physiologic Effect of Epinephrine (Although There is More Clinical Data Available Regarding the Lack of Epinephrine Effect in Asthma than in Anaphylaxis)
Patient Not in Supine Position (See Discussion Regarding “Upright Posture During Anaphylaxis” Below)
From Autopsy Report Data
Presence of Sodium Metabisulfite Antioxidant in Epinephrine
From Case Report Data
However, Refuting its Role is the Observation that Sulfite-Sensitive Asthmatics Tolerate Epinephrine
Other Factors Related to the Management of Anaphylaxis
Initial Misdiagnosis
Anaphylaxis Can Be Mistaken for a Variety of Other Conditions (Such as Asthma Exacerbation, Panic Attack, Myocardial Infarction, and Choking
In Some Cases, Valuable time is Lost or Inappropriate Medications are Given Before the Correct Diagnosis is Recognized (Clin Exp Allergy, 2000) [MEDLINE] (Novartis Found Symp, 2004) [MEDLINE]
Unsuccessful Avoidance of Known Anaphylaxis Triggers
Iatrogenic Medication Errors
Lack of Patient Attention to Food Labelling
Upright Posture During Anaphylaxis
Pulseless Electrical Activity (PEA) Has Been Identified at the Time of Death in Some Patients with Anaphylaxis, Which is Believed to Result from Inadequate Cardiac Filling During Severe Hypotension and Subsequent Cardiac Arrest (So Called “Empty Ventricle Syndrome”) (J Allergy Clin Immunol, 2003)[MEDLINE] (Curr Opin Allergy Clin Immunol, 2005) [MEDLINE] (Masui, 2006) [MEDLINE] (Clin Exp Allergy, 2016) [MEDLINE]
This May Occur Despite Appropriate Epinephrine Administration
Conscious Patients with Bronchospasm May Resist Being Placed Supine, as Supine Posture May Exacerbate Dyspnea
In This Setting, Providing Oxygen and Explaining the Reason for Lying Supine are Important (at Least Until the Cardiovascular Status Can Be Assessed and Optimized)
Patients Who are Vomiting and Also Hypotensive Should Be Placed on Their Side (Rather than Supine) to Avoid Aspiration
History of Previous Anaphylaxis Episodes
Victims of Fatal Anaphylaxis May Not Be Aware that They are Allergic to the Implicated Allergen (Mayo Clin Proc, 1994) [MEDLINE]
In One Series of 25 Anaphylaxis Fatalities, the History of a Previous Reaction Could Be Elicited from the Patient’s Relatives or Medical Records in Only 33% of Cases (Ann Allergy Asthma Immunol, 2007) [MEDLINE]
Even in Patients with Known Past Anaphylaxis Reactions, the Severity of Previous Reactions Cannot Be Relied Upon to Predict the Severity of Future Reactions (NEJM, 1992) [MEDLINE] (Clin Exp Allergy, 1996) [MEDLINE] (Clin Exp Allergy, 2000) [MEDLINE] (J Allergy Clin Immunol, 2001) [MEDLINE] (Clin Exp Allergy, 2003) [MEDLINE] (Allergy Asthma Proc, 2003) [MEDLINE] (J Allergy Clin Immunol, 2007) [MEDLINE] (Forensic Sci Med Pathol, 2019) [MEDLINE]
In Fatal Food-Associated Anaphylaxis, Most Patients Have Had Previous Previous Reactions to the Culprit Food Allergen and were Supposed to Be Avoiding the Food Allergen
However, in Many Cases, These Reactions were So Mild that it is Unlikely that Most Clinicians Would Have Advised the Patient to Carry an Epinephrine Autoinjector
It is Possible that the Patients Experiencing Fatal Food-Associated Anaphylaxis Represent a Subset in Which the Initial Severe Reaction Proved Fatal
Perhaps, Other Patients’ Symptoms Escalated Gradually, Prompting Them to Seek Medical Attention and Thus Be Better Prepared for Reexposure
In Contrast, Venom and Medication-Associated Anaphylaxis Cases Often Had No Known History of a Previous Anaphylactic Reaction
In Many Cases of Venom-Associated Anaphylaxis, the Patient was Stung in the Past and Did Not Manifest Systemic Symptoms (Novartis Found Symp, 2004) [MEDLINE]
Similarly, No History of Previous Anaphylactic Reactions to the Causative Medication Can Be Elicited in Some Drug-Induced Anaphylaxis Fatalities (Clin Exp Allergy, 2000) [MEDLINE] (Novartis Found Symp, 2004) [MEDLINE]
Timing
Latency
Less than 60 min Elapses Between Allergen Exposure and Death in Most Cases of Fatal Anaphylaxis (NEJM, 1992) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2004) [MEDLINE]
Respiratory/Cardiac Arrest and Death Can Occur within Minutes of Onset of Anaphylaxis (NEJM, 1992) [MEDLINE] (Clin Exp Allergy, 2000) [MEDLINE] (J Allergy Clin Immunol, 2001) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2004) [MEDLINE] (J Allergy Clin Immunol, 2007) [MEDLINE] (J Allergy Clin Immunol, 2007) [MEDLINE] (Ann Allergy Asthma Immunol, 2007) [MEDLINE] (Forensic Sci Int, 2009) [MEDLINE] (Am J Forensic Med Pathol, 2009) [MEDLINE]
UK Study of Fatal Anaphylaxis (n = 202) Over 10-Year Period (Clin Exp Allergy, 2000) [MEDLINE]
Interval Between Allergen Exposure and the Onset of Symptoms Varied with the Allergen Type and Route of Exposure
Following Medications, Anaphylaxis Symptoms Appeared After a Mean of 5 min in Hospitalized Patients and After a Mean of 10-20 min in Ambulatory Patients
Following Insect Stings, Anaphylaxis Symptoms Appeared After a Mean of 10-15 min
Following Foods, Anaphylaxis Symptoms Appeared After a Mean of 25-35 min
Phasic Nature and Progression of Anaphylaxis
Most Fatal Anaphylaxis Reactions are Uniphasic, Present Fulminantly, and Progress Rapidly (Although Some Few Follow a More Protracted or Biphasic Course, Typically Over Several Hours) (J Allergy Clin Immunol, 1986) [MEDLINE] (NEJM, 1992) [MEDLINE] (Pediatrics, 2000) [MEDLINE]
Allergen Dose
In General, Higher Allergen Doses are Associated with More Rapid and Severe Anaphylaxis
However, Patients May Have Different Threshold Levels of an Allergen Beyond Which They Will Experience Anaphylaxis
Fatal Food Anaphylaxis Has Been Reported in Response to a Wide Range of Allergen Doses (Ranging from Trace Amounts to Doses >100 g
As Nuts are Considered Especially Potent Allergens, One Review Found that the Dose of Nuts Which was Most Frequently Implicated in Fatalities was Approximately 1 g, While the Dose Most Often Reported in Fatal Anaphylaxis from Other Foods was Approximately 10 g (Curr Opin Allergy Clin Immunol, 2004) [MEDLINE]
Most Insect Sting Anaphylaxis Fatalities Result from a Single Sting (Novartis Found Symp, 2004) [MEDLINE]
Most Drug-Induced Anaphylaxis Fatalities Occur in Response to Normal Doses of the Culprit Medication (Novartis Found Symp, 2004) [MEDLINE]
Mechanism of Death in Fatal Anaphylaxis
Immediate Cause of Death in Fatal Anaphylaxis is Usually Either Asphyxiation Due to Upper/Lower Airway Obstruction or Cardiovascular Collapse (NEJM, 1992) [MEDLINE] (Clin Exp Allergy, 2000) [MEDLINE] (J Allergy Clin Immunol, 2001) [MEDLINE] (Curr Opin Allergy Clin Immunol, 2004) [MEDLINE] (J Allergy Clin Immunol, 2007) [MEDLINE] (J Allergy Clin Immunol, 2007) [MEDLINE] (Ann Allergy Asthma Immunol, 2007) [MEDLINE] (Forensic Sci Int, 2009) [MEDLINE] (Am J Forensic Med Pathol, 2009) [MEDLINE]
Mechanism of Death Appears to Be Related to the Specific Allergen
In an Autopsy Review of Anaphylaxis Fatalities (n = 56), All Food-Associated Anaphylaxis Cases Involved Difficulty Breathing, and Respiratory Arrest was the Mechanism of Death in 13/16 Cases (J Clin Pathol, 2000) [MEDLINE]
In Contrast, in Most Venom/Medication-Associated Anaphylaxis Cases, Shock without Respiratory Compromise was the Mechanism (J Allergy Clin Immunol, 2007) [MEDLINE]
In a Very Small Number of Cases, Massive Epinephrine Overdose or Disseminated Intravascular Coagulation Appeared to Be the Immediate Cause of Death (Novartis Found Symp, 2004) [MEDLINE]
Clinical Manifestations-Refractory Anaphylaxis
Refractory Anaphylaxis is Highly Likely When Both of the Following Clinical Criteria are Present (Joint Task Force on Practice Parameters) (J Allergy Clin Immunol, 2020) [MEDLINE] (Clin Exp Allergy, 2024) [MEDLINE]
Anaphylaxis is Present Following Appropriate Epinephrine Dosing and Symptom-Directed Medical Management (Intravenous Fluid Bolus for Hypotension)
The Initial Anaphylaxis Reaction Has Been Treated with ≥3 Appropriate Doses of Epinephrine (or Initiation of an Intravenous Epinephrine Infusion)
References
Physiology
Profound reversible myocardial depression after anaphylaxis. Lancet. 1988;1(8582):386 [MEDLINE]
Release of calcitonin gene-related peptide in cardiac anaphylaxis. Naunyn Schmiedebergs Arch Pharmacol. 1997;355(2):224 [MEDLINE]
Triggering of plaque disruption and arterial thrombosis in an atherosclerotic rabbit model. Circulation. 1995;91(3):776 [MEDLINE]
Insect sting anaphylaxis; prospective evaluation of treatment with intravenous adrenaline and volume resuscitation. Emerg Med J. 2004;21(2):149 [MEDLINE]
The human heart as a shock organ in anaphylaxis. Novartis Found Symp. 2004;257:133 [MEDLINE]
Anaphylaxis: can we tell who is at risk of a fatal reaction? Curr Opin Allergy Clin Immunol. 2004;4(4):285 [MEDLINE]
Anaphylaxis, killer allergy: long-term management in the community. J Allergy Clin Immunol. 2006;117(2):367 [MEDLINE]
Complement activation-related cardiac anaphylaxis in pigs: role of C5a anaphylatoxin and adenosine in liposome-induced abnormalities in ECG and heart function. Am J Physiol Heart Circ Physiol. 2006;290(3):H1050 [MEDLINE]
Kounis syndrome (allergic angina and allergic myocardial infarction): a natural paradigm? Int J Cardiol. 2006;110(1):7 [MEDLINE]
Further fatalities caused by anaphylactic reactions to food, 2001-2006. J Allergy Clin Immunol. 2007;119(4):1016 [MEDLINE]
Fatal anaphylaxis: postmortem findings and associated comorbid diseases. Ann Allergy Asthma Immunol. 2007;98(3):252 [MEDLINE]
Factors predicting anaphylaxis to peanuts and tree nuts in patients referred to a specialist center. J Allergy Clin Immunol. 2008;121(3):632 [MEDLINE]
Delayed anaphylaxis, angioedema, or urticaria after consumption of red meat in patients with IgE antibodies specific for galactose-alpha-1,3-galactose. J Allergy Clin Immunol. 2009;123(2):426 [MEDLINE]
Antihypertensive medication use is associated with increased organ system involvement and hospitalization in emergency department patients with anaphylaxis. J Allergy Clin Immunol. 2013 Apr;131(4):1103-8 [MEDLINE]
Coronary hypersensitivity disorder: the Kounis syndrome. Clin Ther. 2013;35(5):563 [MEDLINE]
Anaphylaxis and cardiovascular diseases: a dangerous liaison. Curr Opin Allergy Clin Immunol. 2014;14(4):309 [MEDLINE]
Time of Onset and Predictors of Biphasic Anaphylactic Reactions: A Systematic Review and Meta-analysis. J Allergy Clin Immunol Pract. 2015;3(3):408 [MEDLINE]
A rare cause of acute coronary syndrome: Kounis syndrome. Rev Port Cardiol. 2016 Dec;35(12):699.e1-699.e4 [MEDLINE]
Delayed anaphylaxis to alpha-gal, an oligosaccharide in mammalian meat. Allergol Int. 2016 Jan;65(1):16-20 [MEDLINE]
Factors predicting anaphylaxis to peanuts and tree nuts in patients referred to a specialist center. J Allergy Clin Immunol. 2008;121(3):632 [MEDLINE]
Medical and pathologic characteristics of fatal anaphylaxis: a Spanish nationwide 17-year series. Forensic Sci Med Pathol. 2019;15(3):369 [MEDLINE]
Persistent, refractory, and biphasic anaphylaxis: A multidisciplinary Delphi study. J Allergy Clin Immunol. 2020;146(5):1089 [MEDLINE]
Biphasic Reactions in Emergency Department Anaphylaxis Patients: A Prospective Cohort Study. J Allergy Clin Immunol Pract. 2020 Apr;8(4):1230-1238. doi: 10.1016/j.jaip.2019.10.027 [MEDLINE]
World allergy organization anaphylaxis guidance 2020. World Allergy Organ J. 2020;13(10):100472 [MEDLINE]
Risk Factors and Characteristics of Biphasic Anaphylaxis. J Allergy Clin Immunol Pract. 2020;8(10):3388 [MEDLINE]
Persistent, refractory, and biphasic anaphylaxis: A multidisciplinary Delphi study. J Allergy Clin Immunol. 2020;146(5):1089 [MEDLINE]
Anaphylaxis-a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. J Allergy Clin Immunol. 2020;145(4):1082 [MEDLINE]
Management of Refractory Anaphylaxis: An Overview of Current Guidelines. Clin Exp Allergy. 2024;54(7):470 [MEDLINE]