Chlamydia Trachomatis (see Chlamydia Trachomatis): may present with combination of acute urinary symptoms, pyuria, and a negative urine culture in young sexually active female
Most common etiology of UTI: accounts for 75-95% of both male and female UTI cases
Clinical Manifestations
Emphysematous Cystitis: most common microbial etiology of emphysematous cystitis
Emphysematous Pyelonephritis
Herpes Simplex Virus (HSV1 or HSV2) (see Herpes Simplex Virus): may present with combination of acute urinary symptoms, pyuria, and a negative urine culture in young sexually active female
Emphysematous Cystitis: may occur with Klebsiella Pneumoniae (see Klebsiella Pneumoniae)
Emphysematous Pyelonephritis: may occur with Klebsiella Pneumoniae (see Klebsiella Pneumoniae)
Neisseria Gonorrhoeae (Gonococci) (see Neisseria Gonorrhoeae): may present with combination of acute urinary symptoms, pyuria, and a negative urine culture in young sexually active female
Mycoplasma Genitalium (see Mycoplasma Genitalium): may present with urethritis or cystitis
Mycoplasma Hominis (see Mycoplasma Hominis): may present with pyelonephritis
Other Fungi: usually involve the kidney as a result of disseminated infection
Ascending Infection: in female, colonization of vaginal introitus with pathogens from fecal flora -> ascension via urethra into bladder (and ultimately to kidneys, via ureters)
Bacteremic Seeding of Kidney: causes some cases of pyelonephritis
Seeding of Kidneys from Bacteria Within Lymphatics: may play a role in some cases of pyelonephritis
Dipstick positivity for leukocyte esterase or nitrite has 75% sensitivity/82% specificity for detection of UTI: test is not helpful to rule out UTI if symptoms are consistent with UTI and dipstick is negative for both (due to low sensitivity)
Nitrite
Assay: dietary nitrate (normally present in the urine) is converted to nitrite by the nitrate reductase enzyme in certain Gram-negative bacteria -> results in pink color change on dipstick
Specific Gram-negative bacteria (E Coli, Citrobacter, Klebsiella, Proteus, Serratia) possess nitrate reductase and are capable of this conversion
Pseudomonas and Gram-positive bacteria (Enterococcus, etc) do not possess the nitrate reductase enzyme
False-Positive: use of phenazopyridine, beet ingestion
Interpretation: positive nitrite indicates presence of the specific Gram-negative bacteria noted above
Leukocyte Esterase
Assay: granulocyte leukocyte esterase catalyzes the hydrolysis of an amino acid ester to liberate 3-hydroxy-5-phenyl pyrrole! which reacts with a diazonium salt -> results in purple color change on dipstick
Sensitivity: 75-96%/Specificity: 94-98% for >10 WBC per hpf
Interpretation: positive nitrite indicates presence of pyuria
Protein: xxx
Ketone: may be mildly positive in cases with associated dehydration and starvation ketoacidosis or with concomitant diabetic ketoacidosis
RBC (on Microscopy): elevated RBC (microscopic or gross hematuria) may be seen
Hematuria is Common in UTI, But Not in Urethritis or Vaginitis
WBC (on Microscopy): >10 WBC/uL (pyuria) indicates UTI (cystitis or pyelonephritis)
Pyuria May Be Absent in Some Cases of Pyelonephritis with Urinary Tract Obstruction
Odorous, Cloudy, or Discolored Urine in the Absence of Other Localizing Symptoms/Sighs (as Noted Above)
Reflex Urine Cultures Based on Urinalysis Results (Such as Pyuria) in the Absence of Other Indications
Note: the Absence of Pyuria Suggests a Diagnosis Other than Catheter-Associated Urinary Tract Infection (CAUTI)
Urine Culture to Routinely Document Response to Therapy (Unless Symptoms Fail to Resolve)
Assay
Clean-Catch (in female: after cleansing of external urethra prior to collection) or via Foley Catheter
Interpretation
*Historically considered positive if there are >100k CFU/mL in culture (this originated from literature in pregnant females with first void morning urine samples)
However, urinary tract infection may occur with colony counts <100k CFU/mL
Male: colony count >10k CFU/mL is considered positive
Lower colony counts of coliforms (E Coli, etc) are likely to represent significant bacteriuria
In some female cases with infection due to Chlamydia Trachomatis/Neisseria Gonorrhoeae/HSV, culture may be negative
Isolation of Other Organisms from Urine Culture
Lactobacillus, Enterococcus, Staphylococcus Epidermidis and group B Streptococcus isolated from a voided urine culture in female may suggest contamination
However, Presence of organism in midstream voided urine at high colony count and with pure growth may suggest that organism is etiologic
May be required to rule out hydronephrosis (due to obstruction), anatomic abnormailities, nephrolithiasis, etc
Clinical Presentations
Asymptomatic Bacteriuria
Definition
Asymptomatic Bacteriuria is Defined as Positive Urine Culture in the Absence of Clinical Symptoms
Male: defined as single clean-catch voided urine with single bacterial species isolated in count >100k CFU/mL in absence of symptoms
Female: XXXXXX
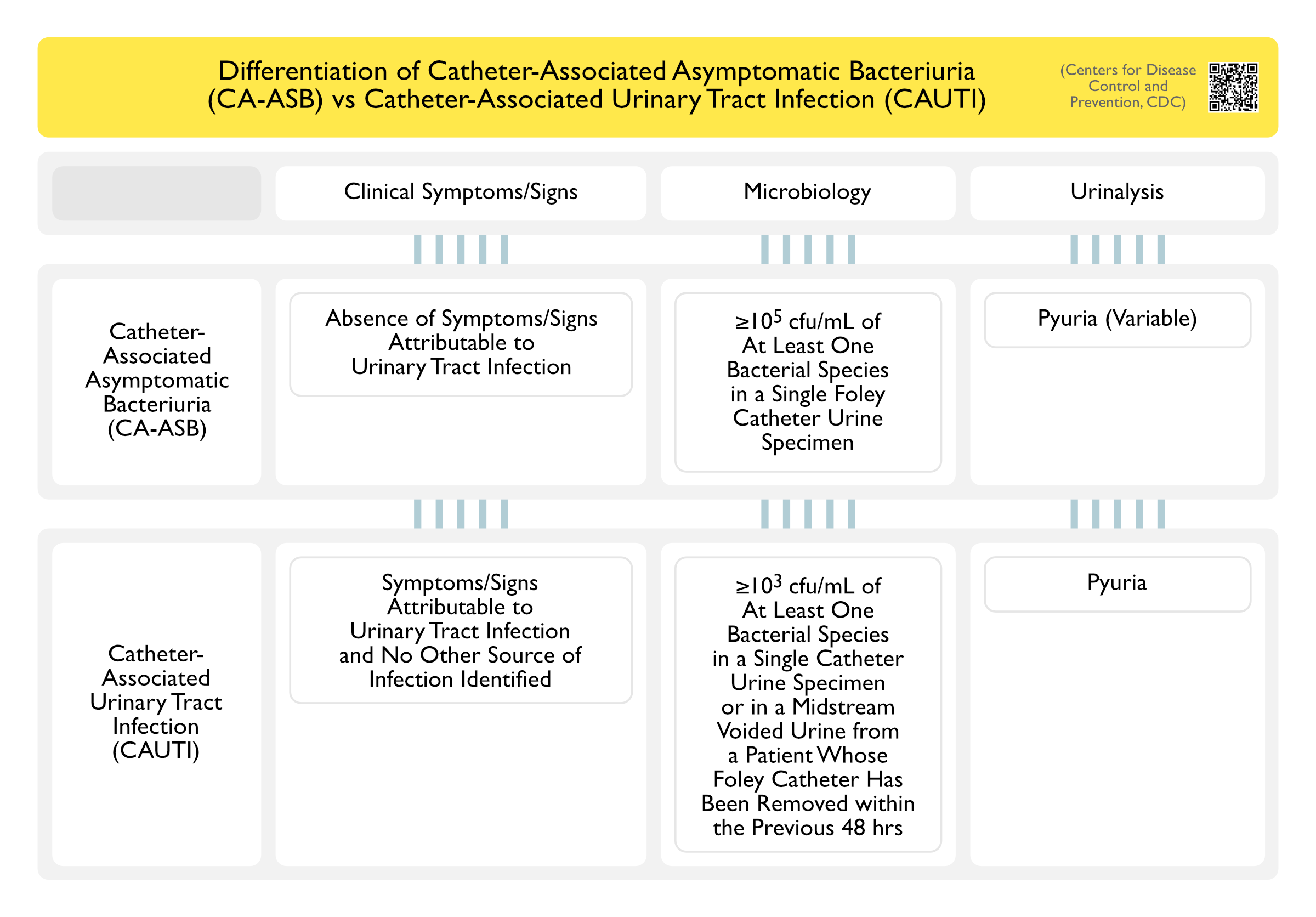
Differentiation of Catheter-Associated Asymptomatic Bacteriuria (CA-ASB) vs Catheter-Associated Urinary Tract Infection (CAUTI) (Centers for Disease Control and Prevention, CDC) [LINK]
Epidemiology
Prevalence of Male Asymptomatic Bacteriuria
Young Male: rare
Elderly Male: prevalence of 6%
Prevalence of Female Asymptomatic Bacteriuria
Young Female: xxx
Elderly Female: prevalence of 18%
Indications to Preoperatively Screen for Asymptomatic Bacteriuria
Other than urologic procedures, the risk of surgical site infection for other surgical procedures (including procedures with high risk of infection, like joint arthroplasty) with pre-operative asymptomatic bacteriuria probably does not warrant screening
Pre-Trans-Urethral Resection of Prostate (TURP): due to risk of bacteremia/sepsis
Pre-Urologic Procedures Where Mucosal Bleeding is Anticipated: due to risk of bacteremia/sepsis
Randomized Trial of Daily Chlorhexidine Bathing to Prevent Healthcare-Associated Infections ( JAMA, 2015) [MEDLINE]
Daily Chlorhexidine Gluconate Bathing Did Not Decrease the Incidence of Healthcare-Associated Infections (Central Line-Associated Bloodstream Infections, Catheter-Related Urinary Tract Infection, Ventilator-Associated Pneumonia, or Clostridium Difficile)
Clinical Guidelines for Short-Course Antibiotics in Common Infections (Annals of Internal Medicine, 2021) [MEDLINE]
In women with uncomplicated bac- terial cystitis, clinicians should prescribe short-course antibi- otics with either nitrofurantoin for 5 days, trimethoprim– sulfamethoxazole (TMP–SMZ) for 3 days, or fosfomycin as a single dose
In men and women with uncomplicated pyelo- nephritis, clinicians should prescribe short-course therapy either with fluoroquinolones (5 to 7 days) or TMP–SMZ (14 days) based on antibiotic susceptibility
Emphysematous Cystitis
Intravenous Antibiotics
Bladder Drainage
Acute Pyelonephritis
Oral (PO) Antibiotics
Amoxicillin-Clavulanic Acid (Augmentin) (ee Amoxicillin-Clavulanic Acid)/Second or Third-Generation Cephalosporins (Cefpodoxime, Cefaclor, Cefdinir) (see Cephalosporins)
Less effective for treatment of pyelonephritis
However, if pathogen is known to be susceptible, need to use at least a 14 day regimen
Fluoroquinolone (see Fluoroquinolones): fluoroquinolones are the only recommended outpatient PO treatment for pyelonephritis
Presence of Bacteremia with Pyelonephritis: does not confer a worse prognosis
References
Emphysematous pyelonephritis: clinicoradiological classification, management, prognosis, and pathogenesis. Arch Intern Med. Mar 27 2000;160(6):797-805 [MEDLINE]
Emphysematous cystitis: An unusual disease of the Genito-Urinary system suspected on imaging. Ann Clin Microbiol Antimicrob. 2004; 3: 20 [MEDLINE]
Chlorhexidine bathing and health care-associated infections: a randomized clinical trial. JAMA. 2015 Jan 27;313(4):369-78. doi: 10.1001/jama.2014.18400 [MEDLINE]
Appropriate Use of Short-Course Antibiotics in Common Infections: Best Practice Advice From the American College of Physicians. Ann Intern Med. 2021 Apr 6. doi: 10.7326/M20-7355 [MEDLINE]