Carbon Dioxide (CO2) Absorption and Excretion During Laparoscopy
CO2 Absorption from Peritoneal Space: CO2 is rapidly absorbed from the peritoneal space during laparoscopy -> this may result in respiratory acidosis, if not properly managed
Direct effects of hypercapnia + acidosis: decreased mycocardial contractility, snesitization of myocardium to arrhythmogenic effects of pressors, systemic vasodilation
Centrally-mediated (autonomic) effects of hypercapnia: sympathetic stimulation with tachycardia and vasoconstriction
Factors Increasing CO2 Absorption During Laparoscopy
High intra-abdominal pressure
Prolonged laparoscopic surgery: allows more time to absorb CO2
Factors Decreasing CO2 Excretion During Laparoscopy
Anesthesiology mismanagement with inadequate minute ventilation maintained on the ventilator
Lung disease: this will increase the required minute ventilation to maintain normal pCO2 during the case
High intra-abdominal pressure: cephalad displacement of the diaphragm decreases lung volumes and produces restriction -> impairs mechanical ventilation
Trendelenburg position: cephalad displacement of the diaphragm decreases lung volumes and produces restriction -> impairs mechanical ventilation
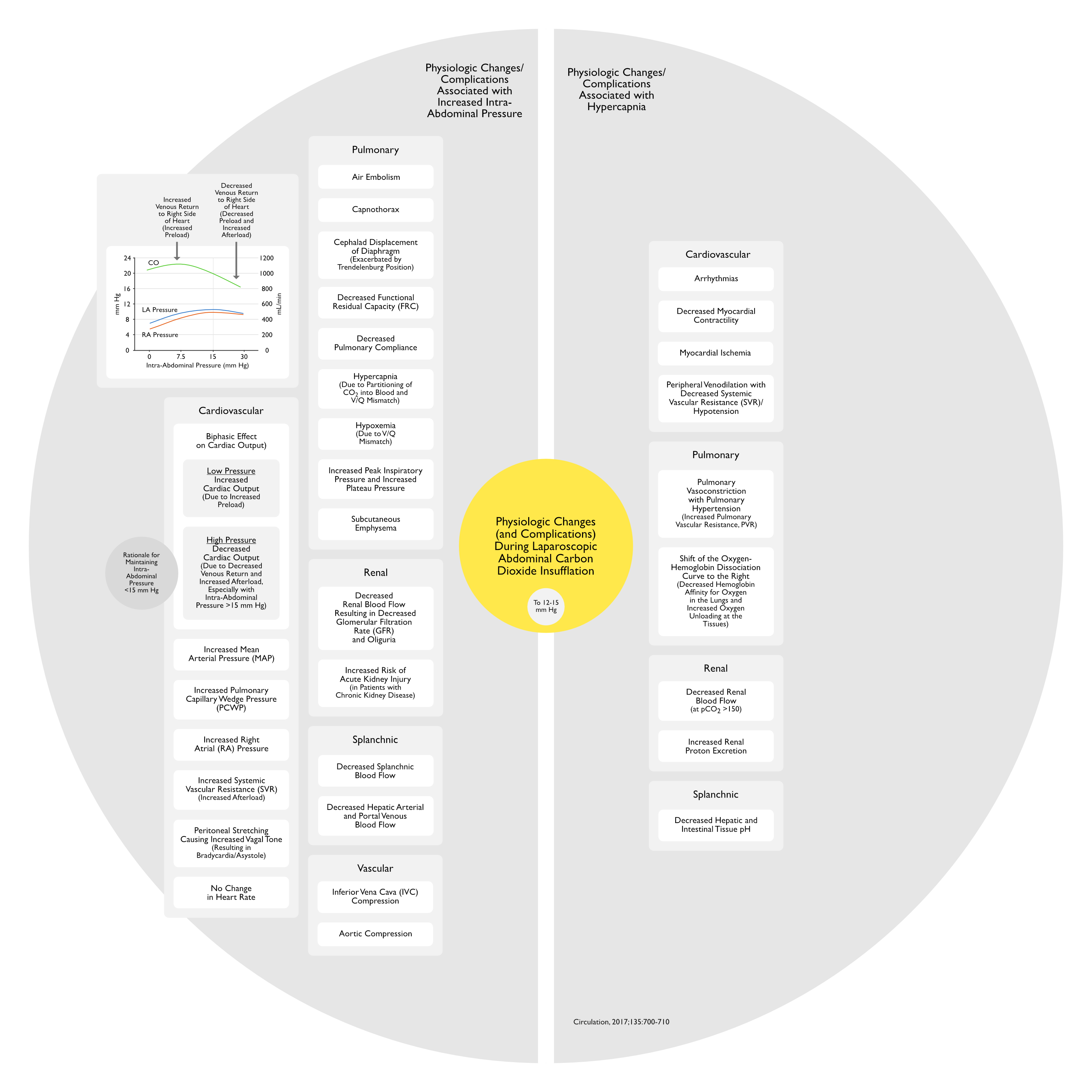
Effects of Increased Intra-Abdominal Pressure During Laparoscopy
Mechanical Impairment of Venous Return: decreased preload
Enhanced CO2 Absorption: as noted above
Impairment of CO2 Excretion via Minute Ventilation: as noted above
Monitoring of intra-abdominal pressure during laparoscopy is crucial, since it may contribute to both increased CO2 absorption and decreased CO2 excretion (via ventilation)
Maintenance of low-moderate intra-abdominal pressures (<12 mm Hg) during laparoscopy can decrease the incidence of adverse effects that result from abdominal CO2 insufflation
Bradycardia/Asystole are Known Complications of Abdominal Insufflation During Laparoscopy (Dig Surg, 2004) [MEDLINE] (JSLS, 2004) [MEDLINE] (Circulation, 2017) [MEDLINE]
Abdominal Insufflation-Associated Hypercapnia (see Hypercapnia)
Impaired Hemoglobin Affinity and Oxygen Transport
Myocardial Depression
Myocardial Ischemia
Abdominal Insufflation-Associated Increase in Intra-Abdominal Pressure (Independent of the Type of Gas Used), Resulting in the Following
Aortic Compression
Due to Aortic Compression and Neuroendocrine Effects, There is Increased Mean Arterial Pressure/Increased Systemic Vascular Resistance/Increased Afterload, Causing a Decrease in Cardiac Output
Decreased Renal Blood Flow
Decreased Splanchnic Blood Flow
Diaphragmatic Displacement Toward Thorax
Resulting in Increased Airway Pressures and Increased Pulmonary Vascular Resistance (PVR)
Inferior Vena Cava Compression
In Animal Models, with Intra-Abdominal Pressure of 5 mm Hg, There is an Early Rise in Right Atrial Pressure and Cardiac Output (Due Predominantly to Compression of the Splanchnic Vasculature, Shifting Blood into the Venous System), Then, as Intra-Abdominal Pressure Increases Further, There is a Decrease in Venous Return to the Right Side of the Heart with Associated Cardiac Output (Due Predominantly to Pooling of Blood in the Lower Extremities)
Stretching of Peritoneum
Results in Vagal Response with Associated Bradycardia or Bradycardia (see Sinus Bradycardia)
<120 L of Carbon Dioxide Can Remain Stored in the Body
Carbon Dioxide is Eliminated by the Lungs and Renal Proton Excretion
In the Presence of Significant Hypercapnia, the Anesthesiologist Should Determine the Optimal Timing of Extubation to Ensure Adequate Removal of Carbon Dioxide
Renal Adverse Effects/Complications
XXXXXXXX
Epidemiology
XXXX
Other Adverse Effects/Complications
xxxx
References
General
XXXX
Adverse Effects/Complications
Circulatory and respiratory complications of carbon dioxide insufflation. Dig Surg. 2004;21(2):95-105. doi: 10.1159/000077038 [MEDLINE]
Recurrent asystolic cardiac arrest and laparoscopic cholecystectomy: a case report and review of the literature. JSLS. 2004 Jan-Mar;8(1):65-8 [MEDLINE]
Cardiovascular and Ventilatory Consequences of Laparoscopic Surgery. Circulation. 2017 Feb 14;135(7):700-710. doi: 10.1161/CIRCULATIONAHA.116.023262 [MEDLINE]