Reversible Platelet P2Y12 Receptor Antagonist (Ticagrelor is a Cyclopentyl-Triazolo-Pyrimidine Which Prevents the Binding of ADP to the P2Y12 Receptor) (see Platelet P2Y12 Receptor Antagonists)
ADP is Released from Platelet Dense Granules and Normally Binds to Both the P2Y1 and P2Y12 Receptors
P2Y1: Gq-coupled receptor which mediates ADP-induced platelet aggregation through the stimulation of phospholipase C and the phosphatidylinositol-signaling pathway
P2Y12 Gi-coupled seven-transmembrane domain receptor which mediates ADP-induced platelet activation by inhibiting the adenylate cyclase-mediated signaling pathway, decreasing intracellular cAMP, inhibition of PI3K, induction of Akt kinase activation
P2Y12 is Also Involved in Platelet Secretion Induced by Various Agonists
Metabolism
XXXXXXXXX
xxxx
Administration
Oral (PO)
Dose: XXXXXXX
Dose Adjustment
Hepatic: XXXX
Renal: XXXXX
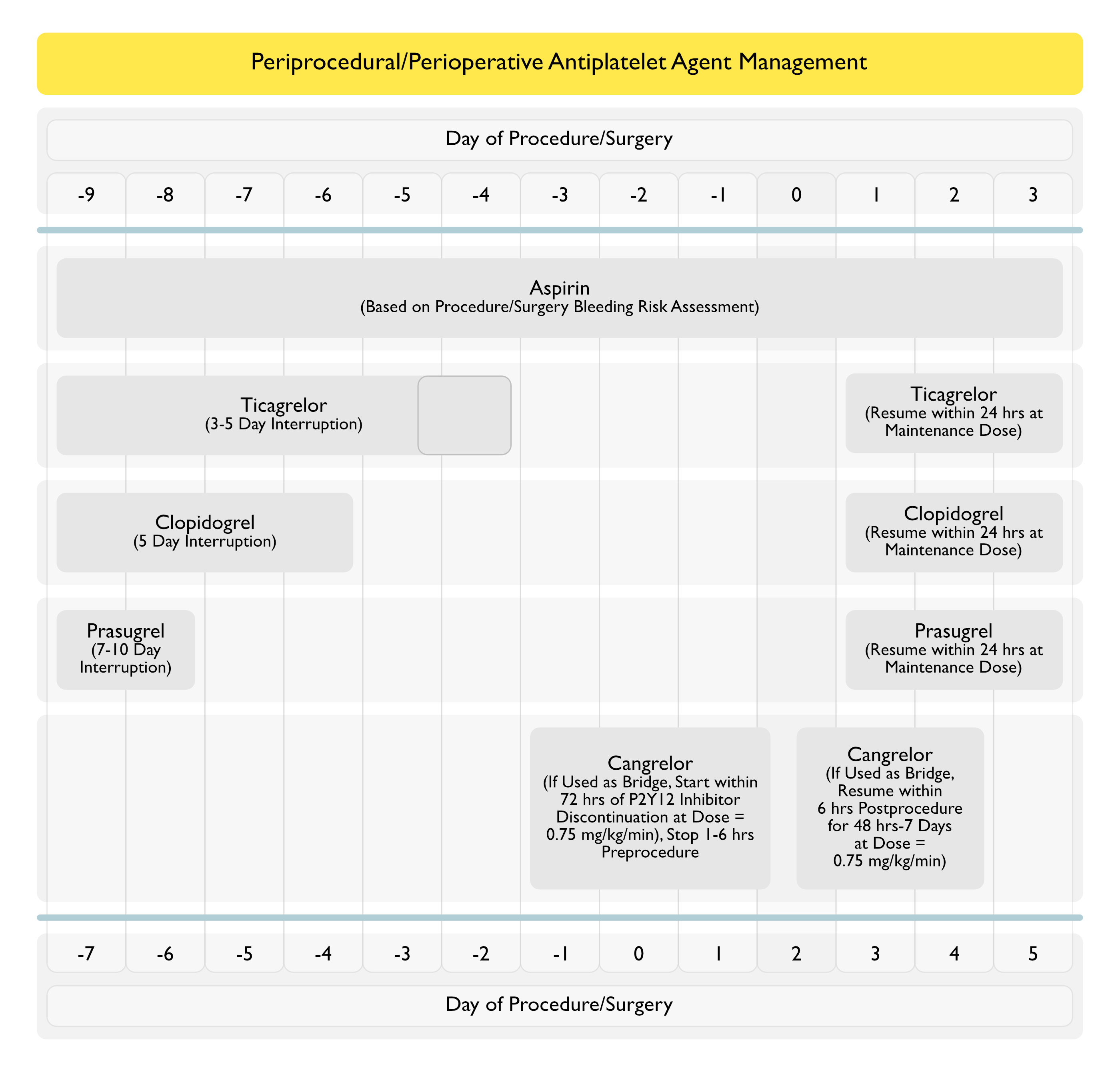
Recommendations for Periprocedural/Perioperative Management of Ticagrelor (American College of Chest Physicians Clinical Practice Guideline for the Perioperative Management of Antithrombotic Therapy) (Chest, 2022) [MEDLINE]
Minor Procedures (Dental, Dermatologic, Ophthalmologic)
In Patients Receiving an Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) Who are Undergoing a Minor Dental Procedure, Continue the Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) (Conditional Recommendation, Very Low Certainty of Evidence)
Patients Who are Receiving Dual Antiplatelet Therapy with Aspirin and a P2Y12 Inhibitor Can Continue Aspirin and Interrupt the P2Y12 Inhibitor
In Patients Receiving an Antiplatelet Drug (Aspirin or P2Y12 inhibitor) Who are Undergoing a Minor Dermatologic Procedure, Continue the Antiplatelet Drug (Aspirin or P2Y12 inhibitor) (Conditional Recommendation, Very Low Certainty of Evidence)
Patients Who are Receiving Dual Antiplatelet Therapy with Aspirin and a P2Y12 Inhibitor Can Continue Aspirin and Interrupt the P2Y12 Inhibitor
In Patients Receiving an Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) Who are Undergoing a Minor Ophthalmologic Procedure, Continue the Antiplatelet Drug (Aspirin or P2Y12 inhibitor) Throughout the Ophthalmologic Procedure (Conditional Recommendation, Low Certainty of Evidence)
Patients Who are Receiving Dual Antiplatelet Therapy with Aspirin and a P2Y12 Inhibitor Can Continue Aspirin and Interrupt the P2Y12 Inhibitor
Elective Non-Cardiac Surgery
In Patients Receiving Ticagrelor Who are Undergoing an Elective Non-Cardiac Surgery, Stop Ticagrelor 3-5 Days (Instead of 7-10 Days) Before Surgery (Conditional Recommendation, Very Low Certainty of Evidence)
Recommendation May Be Modified on a Case-by-Case Basis, Depending on Individual Patient Circumstances (Such as Surgery-Related Bleeding Risk)
Elective Surgery
In Patients Receiving Antiplatelet Drug Therapy Who are Undergoing an Elective Procedure/Surgery, Routine Use of Platelet Function Testing Prior to Procedure/Surgery is Not Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
Platelet Function Testing Could Be Used with a Possible Small Benefit and Little Harm in Certain Scenarios Such as Patients Undergoing Coronary Artery Bypass Graft (CABG) Surgery Who Have Recently Started Taking a P2Y12 Inhibitor
Costs Would Be Moderate for Implementation
In Patients Who Require Antiplatelet Drug Interruption for an Elective Procedure/Surgery, Resume Antiplatelet Drugs in ≤24 hrs (Instead of >24 hrs) After the Procedure/Surgery (Conditional Recommendation, Very Low Certainty of Evidence)
In Patients Receiving ASA and a P2Y12 Inhibitor with Coronary Stents Placed within the Last 6-12 wks Who are Undergoing an Elective Procedure/Surgery, Continuation Both Antiplatelet Agents or Stop One Antiplatelet Agent within 7-10 Days of Procedure/Surgery (Conditional Recommendation, Very Low Certainty of Evidence)
Either Approach is Reasonable Depending on the Bleeding Risk Associated with the Procedure/Surgery if Antiplatelet Therapy is Continued and Risk for Acute Coronary Syndrome/Coronary Stent Thrombosis if Antiplatelet Therapy is Interrupted
The Following Factors Will Weigh in the Decision About Whether to Continue Dual Antiplatelet Therapy or Interrupt One Agent
Timing of Stent Placement (Whether Closer to 6 wks or 12 wks)
Type of Stent (Drug-Eluting or Bare-Metal)
Location of the Stent (Whether at a Dominant Coronary Artery or Not)
Number and length of Stents Implanted
In Patients Receiving Aspirin and a P2Y12 Who Had Coronary Stents Placed within the Last 3-12 mos and are Undergoing an Elective Procedure/Surgery, Stop the P2Y12 Inhibitor Prior to Procedure/Surgery (as Opposed to Continuing the P2Y12 Inhibitor (Conditional Recommendation, Very Low Certainty of Evidence)
Recommendation is Based on Indirect Evidence and Expert-Based Consensus that Stopping P2Y12 Inhibitors in Patients with Stents > 3 mos Postimplantation is Likely Safe
The Following Factors Will Weigh in the Decision About Whether to Interrupt the P2Y12 Inhibitor
Timing of Stent Placement (Whether Closer to 3 mos or 12 mos)
Type of Stent (Drug-Eluting or Bare-Metal)
Location of the Stent (Whether at a Dominant Coronary Artery or Not)
Number and length of Stents Implanted
In Patients with Coronary Stents Who Require Interruption of Antiplatelet Drugs for an Elective Procedure/Surgery, Routine Bridging Therapy with a Glycoprotein IIb-IIIa Inhibitor, Cangrelor, or Low Molecular Weight Heparin is Not Recommended (Conditional Recommendation, Low Certainty of Evidence)
Bridging Approach May Be Considered in Selected High-Risk Patients (Those with Coronary Stent Placed within 3 mos in a Critical Location)
In Patients with Coronary Stents Who Require Continued Dual Antiplatelet Therapy, Delaying an Elective Procedure/Surgery is Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
Duration of Procedure/Surgery Delay is Addressed on a Case-by-Case Basis and Should Consider the Urgency of the Procedure/Surgery, the Time Elapsed Since Coronary Stenting, and the Risk Profile of the Coronary Stenting (Critical Location, Multiple Stents, etc)
In Patients Receiving a P2Y12 Inhibitor Drug (Clopidogrel, Prasugrel, Ticagrelor) and Undergoing Coronary Artery Bypass Graft (CABG) Surgery, Stop the P2Y12 Inhibitor Perioperatively (Conditional Recommendation, Low Certainty of Evidence)
Stop Prasugrel for a Period of 7 Days Preoperatively
Stop Clopidogrel for a Period of 5 Days Preoperatively
Stop Ticagrelor for a Period of 3-5 Days Preoperatively
In Patients Receiving ASA or a P2Y12 Inhibitor Who are Undergoing Coronary Artery Bypass Graft (CABG) Surgery, Resume the Aspirin or the P2Y12 Inhibitor in ≤24 hrs (as Opposed to ≥24 hours) After Surgery (Conditional Recommendation, Low Certainty of Evidence)
Resumption of Antiplatelet Therapy May Be Delayed in Patients Who Develop Post-CABG Thrombocytopenia (Platelet Count < 50k), Typically Occurring with On-Pump Surgery
Cases Have Been Reported (HeartRhythm Case Rep, 2018) [MEDLINE]
Risk Factors
Concurrent Use of Atrioventricular Nodal Blocking Agents
Underlying Conduction Sytem Disease (Sick Sinus Syndrome, Atrioventricular Block, Left Bundle Branch Block, Right Bundle Branch Block, Bradycardia-Related Syncope Not Protected by a Pacemaker)
Physiology
Possible Direct Effect of P2Y12 Inhibition on Cardiac Automaticity or Conduction
Possible Inhibition of Red Blood Cell Adenosine Uptake, Exacerbating Vagal-Mediated Nocturnal Bradycardia and/or Directly Inhbiting Sinoatrial (SA) Node Conduction
Cases Have Been Reported (HeartRhythm Case Rep, 2018) [MEDLINE]
Risk Factors
Concurrent Use of Atrioventricular Nodal Blocking Agents
Underlying Conduction Sytem Disease (Sick Sinus Syndrome, Atrioventricular Block, Left Bundle Branch Block, Right Bundle Branch Block, Bradycardia-Related Syncope Not Protected by a Pacemaker)
Physiology
Possible Direct Effect of P2Y12 Inhibition on Cardiac Automaticity or Conduction
Possible Inhibition of Red Blood Cell Adenosine Uptake, Exacerbating Vagal-Mediated Nocturnal Bradycardia and/or Directly Inhbiting Sinoatrial (SA) Node Conduction
Clinical
General Comments
In Some Cases, Bradycardia Occurred within Hours of Ticagrelor Administration (Int J Cardiol, 2016) [MEDLINE] (Int J Cardiol, 2016) [MEDLINE] (HeartRhythm Case Rep, 2018) [MEDLINE]
Ventricular Pauses Have Been Reported to Occur in 4-6% of Cases
Risk Factors
Concurrent Use of Atrioventricular Nodal Blocking Agents
Underlying Conduction Sytem Disease (Sick Sinus Syndrome, Atrioventricular Block, Left Bundle Branch Block, Right Bundle Branch Block, Bradycardia-Related Syncope Not Protected by a Pacemaker)
Physiology
Possible Direct Effect of P2Y12 Inhibition on Cardiac Automaticity or Conduction
Possible Inhibition of Red Blood Cell Adenosine Uptake, Exacerbating Vagal-Mediated Nocturnal Bradycardia and/or Directly Inhbiting Sinoatrial (SA) Node Conduction
Ticagrelor Use is Associated with Cheyne-Stokes Respiration (NEJM, 2016) [MEDLINE]
Ticagrelor Use is Associated with Central Sleep Apnea (J Am Coll Cardiol, 2018) (J Clin Sleep Med, 2019) [MEDLINE] [MEDLINE] (Sleep, 2024) [MEDLINE]
Ticagrelor Use After Acute Coronary Syndrome (in the Absence of Congestive Heart Failure) is Associated with an Increased Risk of Central Sleep Apnea (Defined as AHI ≥15) (Occurs in 30% in Patients Taking Ticagrelor vs 7.3% in Patients Not Taking Ticagrelor) (Sleep Med, 2021) [MEDLINE]
On Multivariate Analysis, Only Age and Ticagrelor Use were Associated with the Occurrence of Central Sleep Apnea (p = 0.0007 and p = 0.0006)
Medication-Induced Central Sleep Apnea: A Unifying Concept. Sleep. 2024 Feb 9:zsae038. doi: 10.1093/sleep/zsae038 [MEDLINE]
XXXXX
Physiology
Adverse Effect is Not Dose-Related
Due to Inhibition of Sodium-Independent Equilibrative Transporter-1, Resulting in Increased Plasma Adenosine Levels and Affecting Vagal Fibers in the Lung (Circulation, 2018) [MEDLINE] (Sleep Med, 2021) [MEDLINE]
Ticagrelor May Have Central Nervous Sytem P2Y12 Receptor Inhibitory Effects, Resulting in Increased Chemosensitivity to Hypercapnia (Sleep Med, 2021) [MEDLINE]
Clinical
Onset of Central Sleep Apnea is Variable (May Occur from 7 Days Up to 1 Year Following Initiation of Ticagrelor Therapy) (Sleep Med, 2021) [MEDLINE]
Oral Reversible Antiplatelet Agents (Ticagrelor, Elinogrel, Cangrelor) Have Been Demonstrated to Increase the Incidence of Dyspnea in Trials (Cardiology, 2014) [MEDLINE]
However, Irreversible Oral Antiplatelet Agents (Aspirin, Ticlopidoine, Clopidogrel, and Prasugrel) and Intravenous Glycoprotein IIb/IIIa Inhibitors (Abciximab, Eptifibatide, Tirofiban) Do Not Increase the Incidence of Dyspnea
In Contrast to the High Double-Digit Rates of Dyspnea wih Oral Ticagrelor and Elinogrel, Dyspnea Risks with Intravenous Cangrelor were Smaller (<2%) But Still Consistently and Significantly Higher than in the Corresponding Control Arms
Study of Ticagrelor With Aspirin or Alone in High-Risk Patients After Coronary Intervention (TWILIGHT) Trial (JACC Cardiovasc Inter, 2023) [MEDLINE]: n = 179 patients who discontinued ticagrelor (due to dyspnea)
At 3 Months, the Incidence of Dysnea-Related Ticagrelor Discontinuation was 6.4%
At 15 Months, the Incidence of Dysnea-Related Ticagrelor Discontinuation was 9.1%
Risk Factors for Dysnea-Related Ticagrelor Discontinuation
Protective Factors for Dysnea-Related Ticagrelor Discontinuation
Asian Race
Among the 179 Patients Who Discontinued Ticagrelor Because of Dyspnea, Ticagrelor Monotherapy was Not Associated with a Higher Risk of Susequent Ischemic Events (Composite of All-Cause Death, Myocardial Infarction, or Stroke) Compared with Ticagrelor Plus Aspirin (5.0% vs 7.1%; P = 0.566)
Clinical Impact of Dyspnea after Ticagrelor Treatment and the Effect of Switching to Clopidogrel in Patients with Myocardial Infarction. Thromb Haemost. 2024 May 3. doi: 10.1055/a-2299-4537 [MEDLINE]
Background: Dyspnea is frequent during ticagrelor-based dual antiplatelet therapy (DAPT) for acute myocardial infarction (AMI). However, its clinical characteristics or management strategy remains uncertain
Methods
The study assessed 2,617 AMI patients from the Ticagrelor versus Clopidogrel in Stabilized Patients with AMI (TALOS-AMI) trial
Dyspnea during 1-month ticagrelor-based DAPT and following DAPT strategies with continued ticagrelor or de-escalation to clopidogrel from 1 to 12 months were evaluated for drug adherence, subsequent dyspnea, major adverse cardiovascular events (MACE), and bleeding events
Results
Dyspnea was reported by 538 patients (20.6%) during 1 month of ticagrelor-based DAPT
Adherence to allocated DAPT over the study period was lower in the continued ticagrelor arm than the de-escalation to clopidogrel, particularly among the dyspneic population (81.1% vs. 91.5%, p < 0.001)
Among ticagrelor-treated patients with dyspnea, those switched to clopidogrel at 1 month had a lower frequency of dyspnea at 3 months (34.3% vs. 51.7%, p < 0.001) and 6 months (25.5% vs. 38.4%, p = 0.002) than those continued with ticagrelor
In patients with dyspnea in their 1-month ticagrelor-based DAPT, de-escalation was not associated with increased MACE (1.3% vs. 3.9%, hazard ratio [HR]: 0.31, 95% confidence interval [CI]: 0.08-1.11, p = 0.07) or clinically relevant bleeding (3.2% vs. 6.2%, HR: 0.51, 95% CI: 0.22-1.19, p = 0.12) at 1 year
Conclusion
Dyspnea is a common side effect among ticagrelor-based DAPTs in AMI patients
Switching from ticagrelor to clopidogrel after 1 month in AMI patients may provide a reasonable option to alleviate subsequent dyspnea in ticagrelor-relevant dyspneic patients, without increasing the risk of ischemic events
Physiology
Not Dose-Related
Due to Inhibition of Sodium-Independent Equilibrative Transporter-1, Resulting in Increased Plasma Adenosine Levels and Affecting Vagal Fibers in the Lung (Circulation, 2018) [MEDLINE] (Sleep Med, 2021) [MEDLINE]
Ticagrelor May Have Central Nervous Sytem P2Y12 Receptor Inhibitory Effects, Resulting in Increased Chemosensitivity to Hypercapnia (Sleep Med, 2021) [MEDLINE]
Clinical
Onset of Dyspnea May Be Rapid J Cardiovasc Med-Hagerstown, 2018) [MEDLINE]
Onset of Dyspnea Typically Develops within the First 24 hrs of Therapy (But May Occur Later in Some Cases) J Cardiovasc Med-Hagerstown, 2018) [MEDLINE]
Increased Serum Creatinine Occurs in 4-7% of Cases
Clinical
Transient
References
General
XXXXXX
Periprocedural/Perioperative Management of Ticagrelor
Perioperative Management of Antithrombotic Therapy: An American College of Chest Physicians Clinical Practice Guideline. Chest. 2022 Aug 11;S0012-3692(22)01359-9. doi: 10.1016/j.chest.2022.07.025 [MEDLINE]
Adverse Effects
Cardiovascular Adverse Effects
Clinically significant ticagrelor induced conduction abnormalities following percutaneous coronary intervention. Int J Cardiol. 2016 Jul 1:214:21-2. doi: 10.1016/j.ijcard.2016.03.143 [MEDLINE]
The progressed atrioventricular block associated with ticagrelor therapy may not require permanent pacemaker after acute coronary syndrome; it may be reversible. Int J Cardiol. 2016 Jan 15:203:822-4. doi: 10.1016/j.ijcard.2015.11.042 [MEDLINE]
Cyclical sinus bradycardia and atrioventricular block induced by ticagrelor. HeartRhythm Case Rep. 2018 Aug 8;4(11):527-529. doi: 10.1016/j.hrcr.2018.07.017. eCollection 2018 Nov [MEDLINE]
Ticagrelor-induced thrombotic thrombocytopenic purpura: A case report and review of the literature. Medicine (Baltimore). 2018 Jun;97(26):e11206. doi: 10.1097/MD.0000000000011206 [MEDLINE]
Renal Adverse Effects
XXXXX
Pulmonary Adverse Effects
Cheyne-Stokes Respiration, Chemoreflex, and Ticagrelor-Related Dyspnea. N Engl J Med. 2016 Sep 8;375(10):1004-6. doi: 10.1056/NEJMc1601662 [MEDLINE]
Ticagrelor-related late-onset dyspnea as cause of emergency department visit: a 3-year outpatient study. J Cardiovasc Med (Hagerstown). 2018 Jun;19(6):284-289. doi: 10.2459/JCM.0000000000000656 [MEDLINE]
Adenosine and Ticagrelor Plasma Levels in Patients With and Without Ticagrelor-Related Dyspnea. Circulation. 2018 Aug 7;138(6):646-648. doi: 10.1161/CIRCULATIONAHA.118.034489 [MEDLINE]
Ticagrelor and Central Sleep Apnea. J Am Coll Cardiol. 2018 May 22;71(20):2378-2379. doi: 10.1016/j.jacc.2018.03.447 [MEDLINE]
Ticagrelor-Associated Shift From Obstructive to Central Sleep Apnea: A Case Report. J Clin Sleep Med. 2019 Aug 15;15(8):1179-1182. doi: 10.5664/jcsm.7818 [MEDLINE]
Central sleep apnea after acute coronary syndrome and association with ticagrelor use. Sleep Med. 2021 Apr:80:39-45. doi: 10.1016/j.sleep.2021.01.026 [MEDLINE]
Central sleep apnea after acute coronary syndrome and association with ticagrelor use. Sleep Med. 2021 Apr:80:39-45. doi: 10.1016/j.sleep.2021.01.026 [MEDLINE]
Medication-Induced Central Sleep Apnea: A Unifying Concept. Sleep. 2024 Feb 9:zsae038. doi: 10.1093/sleep/zsae038 [MEDLINE]