

History of Oxygen Use
- 1770’s
- Joseph Priestly was a Chemist Who Produced Oxygen by Heating Mercuric Oxide (HgO): named it “dephlogisticated air”
- Carl Wilhelm Scheele was a Chemist Who Produced Oxygen by Heating Mercuric Oxide (HgO): named it “fire air”
- 1774
- Oxygen was First Recognized as a Distinct Element
- Antoine Lavoisier (Who Coined the Term Oxygen) Mistakenly Believed that Oxygen was Required to Form All Acids (Greek Words Oxys + Genes = Acid Forming)
- 1885
- First Recorded Medical Use of Oxygen was by Dr George Holtzapple in the Treatment of a Patient with Pneumonia https://www.inogen.com/resources/oxygen-concentrators/history-of-oxygen-concentrators/)
- 1890
- Use of Supplemental Oxygen was First Reported in the Medical Literature (The Continuous Inhalation of Oxygen in Cases of Pneumonia Otherwise Fatal, and in Other Diseases; Boston Med J 1890;123:481-5)
- Around 1900
- First Use of the Nasal Cannula to Deliver Oxygen
- 1950’s
- First Ambulatory Use of Oxygen (Delivered from High-Pressure Cylinders) to Treat Chronic Obstructive Pulmonary Disease (COPD) Patients in the UK
- Current Era
- Supplemental Oxygen is Used in >25% of Patients Who Present to the Emergency Department (Emerg Med J, 2008) [MEDLINE]

Physiology of Oxygen
Oxygen is Required for Adenosine Triphosphate (ATP) Synthesis, But Oxygen Also Has Strong Oxidizing Properties, Which May Contribute to Damage to Many Biologic Molecules (Crit Care Med, 2008) [MEDLINE]
- Formation of Reactive Oxygen Species (ROS) are Believed to Contribute to the Development of Oxygen Toxicity
- During Mitochondrial Respiration, Approximately 1–3 % of Oxygen Consumption Results in the Formation of Reactive Oxygen Species
- Reactive Oxygen Species Have Normal Biologic Roles in Host Defense and Signaling, But They May Also Exert Toxic Biologic Effects
Indications
Acute Coronary Syndrome (ACS) (see Coronary Artery Disease)
Rationale
- There is No Evidence that Withholding Supplemental Oxygen in Normoxic Patients Suspected of Acute Coronary Syndrome Affects the Rate of Death and/or Resolution of Chest Pain
- There is Only a Very Lw Level of Evidence that Withholding Supplemental Oxygen Reduces Infarct Size
- There is No Evidence that Withholding Supplemental Oxygen Therapy Affects the Resolution of EKG Abnormality
Clinical Efficacy
- AVOID Study of Oxygen Therapy in Acute Myocardial Infarction (Circulation, 2015) [MEDLINE]
- Supplemental Oxygen Therapy in Patients with ST-Elevation Myocardial Infarction, But without Hypoxia May Increase Early Myocardial Injury and was Associated with Larger Myocardial Infarct Size Assessed at 6 Months
- DETOX2-SWEDEHEART Trial of Oxygen in Acute Myocardial Infarction (NEJM, 2017) [MEDLINE]: n = 6629
- Routine Use of Supplemental Oxygen in Patients with Suspected Myocardial Infarction Who Did Not Have Hypoxemia was Not Found to Reduce 1 Year All-Cause Mortality
- Retrospective Study of Early Hyperoxia in the Treatment of Patients with Myocardial Injury (PLoS One. 2018 Aug 7;13(8):e0201286. doi: 10.1371/journal.pone.0201286. eCollection 2018 [MEDLINE]
- Hyperoxia during the first 24 hours of presentation is associated with an increased 28-day in-hospital mortality rate and risks of coagulation and hepatic dysfunction in patients with myocardial injury
- Meta-Analysis of Oxygen in the Treatment of Acute Myocardial Infarction (Heart, 2018) [MEDLINE]: n = 7998 (8 trials)
- Although supplemental O2 therapy is commonly used, it was not associated with important clinical benefits
Recommendations (American Heart Association 2015 Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care) (Circulation, 2015)[MEDLINE]
- Usefulness of Supplementary Oxygen Has Not Been Established in Normoxic Patients
- In the Prehospital, Emergency Department, and Hospital Settings, the Withholding of Supplementary Oxygen May Be Considered in Normoxic Patients with Suspected or Confirmed Acute Coronary Syndrome (Class IIb Recommendation, Level of Evidence C-LD)
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- In Patients with Myocardial Infarction/Stroke, Supplemental Oxygen is Not Recommended for Patients with SpO2 >92% Due to No Likely Benefit and Possible Risk of Harm (Strong Recommendation)
- In Patients with Myocardial Infarction/Stroke, Supplemental Oxygen is Not Recommended for Patients with SpO2 90-92% Due to No Likely Benefit and Possible Risk of Harm (Weak Recommendation)
Air Embolism (see Air Embolism)
Clinical Efficacy
- Supplemental Oxygen Increases the Partial Pressure of Oxygen and Decreases the Partial Pressure of Nitrogen in the Blood, Resulting in a Positive Pressure Gradient for the Diffusion of Nitrogen from the Air Bubbles into the Blood, Accelerating Resorption of Air Emboli
- High-Flow Supplemental Oxygen Increases the Partial Pressure of Oxygen in the Blood and Decreases the Partial Pressure of Nitrogen in the Blood (Undersea Hyperb Med, 1998) [MEDLINE]
- This Results in Diffusion of Nitrogen from Inside of the Air Embolism Bubble (Which Has a High Nitrogen Content) into the Blood (Which Will Have a Low Nitrogen Content): decreases the size of the bubble, accelerating bubble resorption
- High-Flow Supplemental Oxygen Increases the Partial Pressure of Oxygen in the Blood and Decreases the Partial Pressure of Nitrogen in the Blood (Undersea Hyperb Med, 1998) [MEDLINE]
- In Contrast, Nitrous Oxide (N20) (Sometimes Given During General Anesthesia) Can Diffuse from the Blood into Air Emboli, Causing the Gas Bubbles to Enlarge and the Patient to Deteriorate (Anesth Analg, 1971) [MEDLINE] (Anesthesiology, 2007) [MEDLINE] (see Nitrous Oxide)
- Therefore, Nitrous Oxide Should Be Discontinued if Air Embolism is Suspected
Carboxyhemoglobinemia (see Carboxyhemoglobinemia)
Rationale
- Mechanism
- Oxygen Inhibits Carbon Monoxide Binding to Hemoglobin and Carbon Monoxide is Subsequently Excreted Through the Lungs
- On Room Air, the Half-Life of Carboxyhemoglobin is 250-320 min
- On 100% Oxygen (Provided Via a High-Flow Non-Rebreather Mask), the Half-Life of Carboxyhemoglobin is 90 min
- Supplemental Oxygen Treats Tissue Hypoxia
- Oxygen Inhibits Carbon Monoxide Binding to Hemoglobin and Carbon Monoxide is Subsequently Excreted Through the Lungs
Clinical Efficacy
- Administration of 100% Oxygen at Atmospheric Pressure Shortens the Half-Life of Carboxyhemoglobin (74 +/- 25 min) as Compared to the Half-Life Influenced by the Paient’s Own pO2 (130 +/- 130 min) (Chest, 2000)[MEDLINE]
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- Higher SpO2 Target (Approaching 100%) is Probably Recommended
Cluster Headache (see Cluster Headache)
Clinical Efficacy
- xxxx
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- Higher SpO2 Target (Approaching 100%) is Probably Recommended
During Rapid Sequence Endotracheal Intubation (RSI) (see Airway Management)
Rationale
- Pre-Oxygenation with Supplemental Oxygen Bag-Mask Ventilation: removes nitrogen from the lungs and creates an alveolar oxygen reservoir (this reservoir remains fixed at the end of pre-oxygenation and does not get replenished once depleted)
- Mechanisms to Increase the Reservoir Size
- Head-Up Patient Positioning: reduces dependent atelectasis
- Increasing Mean Airway Pressure
- Mechanisms to Increase the Reservoir Size
Clinical Efficacy
- Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) Increases Apnea Time During Endotracheal Intubation (Anaesthesia, 2015) [MEDLINE]
- High-Nasal Cannula Oxygenation (During Preoxygenation and Continuing as Post-Oxygenation During Intravenous Induction of Anaesthesia and Neuromuscular Blockade Until Airway was Secured) Increases the Apnea Time During Endotracheal Intubation
- Proposed Mechanism: combines the benefits of classical apneic oxygenation with continuous positive airway pressure and gaseous exchange through flow-dependent deadspace flushing
- French PREOXYFLOW Multicenter Randomized Trial of High-Flow Nasal Cannula in Hypoxemic Patients Undergoing Intubation (Intensive Care Med, 2015) [MEDLINE]: n = 124
- In Terms of the Lowest Level of Oxygen Desaturation, High-Flow Nasal Cannula (Maintained Throughout the Procedure) was Comparable to High-Flow Face Mask Preoxygenation (Removed at End of General Anesthesia Induction)
- No Differences were Observed in Difficult Intubations, Ventilator-Free Days, intubation-Related Events, or Mortality Rate
- Trial of High-Flow Nasal Cannula During Endotracheal Intubation in ICU Patients (Crit Care Med, 2015) [MEDLINE]: n = 101
- High-Flow Nasal Cannula Oxygen Significantly Improved Preoxygenation and Reduced the Prevalence of Severe Hypoxemia, as Compared to Non-Rebreathing Bag Reservoir Facemask Oxygen
- German Randomized Trial of Flow Nasal Cannula Versus Bag-Valve-Mask for Preoxygenation Before Intubation in Subjects With Hypoxemic Respiratory Failure (Respir Care, 2016) [MEDLINE]: n = 40
- No Significant Difference in the Mean Lowest Oxygen Saturation During intubation Between the High-Flow Nasal Cannula Group and the Bag-Valve-Mask-Ventilation Group in Patients with Mild-Moderate Hypoxemic Respiratory Failure
- However, On Continuous Monitoring, There was a Significant Decrease in Oxygen Saturation During the Apnea Phase Before Intubation in the Bag-Valve-Mask-Ventilation Group, which was Not Observed in the High-Flow Nasal Cannula Group
- French OPTINIV Trial of High-Flow Nasal Cannula Combined with Noninvasive Positive-Pressure Ventilation vs Noninvasive Positive-Pressure Ventilation Alone for Preoxygenation Prior to Intubation (Intensive Care Med, 2016) [MEDLINE]: single-center, blinded, randomized trial
- Use of Combined High-Flow Nasal Cannula + Noninvasive Positive-Pressure Ventilation for Preoxygenation Prior to Intubation was More Effective in Decreasing Oxygen Desaturation, as Compared to Noninvasive Positive-Pressure Ventilation Alone
- Trial of Apneic Oxygenation During Rapid Sequence Intubation in the Emergency Department (Acad Emerg Med, 2016) [MEDLINE]
- Apneic Oxygenation During RSI Increased the First Pass Success (without Hypoxemia) Rate: defined as successful intubation with SaO2 remaining ≥90%
- Randomized Trial of Apneic Oxygenation During Intubation in a Medical ICU (Am J Respir Crit Care Med, 2016) [MEDLINE]: n = 150
- Apneic Oxygenation with High-Flow Nasal Cannula (15 L/min) During Intubation Did Not Increase the Lowest SaO2, as Compared to Usual Care
- Systematic Review and Meta-Analysis of Support Techniques to Prevent Oxygen Desaturation in Critically Ill Patients Requiring Endotracheal Intubation ( J Crit Care, 2017) [MEDLINE]
- Apneic Oxygenation was Significantly Associated with Higher Minimum Oxygen Saturation During Intubation, as Compared to No Apneic Oxygenation: but there were no significant differences in severe hypoxemia and intubation related-complications
- *Further Study is Required to Evaluate the Role of Noninvasive Positive-Pressure Ventilation (NIPPV) and High-Flow Nasal Cannula (HFNC) *
High Altitude in Patients with with Cardiopulmonary Disease (see High Altitude)
General Comments
- Requirement for Supplemental Oxygen for Patients with Cardiopulmonary Disease at Altitude Can Be Determined Using Both Hypoxia Altitude Simulation Test (HAST) and 6-Minute Walk Test (6MWT)
Hypoxia Altitude Simulation Test (HAST) (see Hypoxia Altitude Simulation Test)
Hypoxia Altitude Simulation Test (HAST) Interpretation
- pO2 >55 mm Hg During HAST: no supplemental oxygen is required
- pO2 50-55 mm Hg During HAST: considered borderline -> measurement with activity can then be obtained
- pO2 <50 m Hg During HAST: testing with supplemental oxygen (usually 2L/min) is performed
6-Minute Walk Test (6MWT) (see 6-Minute Walk Test)
Clinical Efficacy
- Comparative Study of 6MWT and Hypoxia Altitude Simulation Test (HAST) in Patients with Either Interstitial Lung Disease or COPD (Aviat Space Environ Med, 2007) [MEDLINE]
- Oxygen Desaturation Induced by the 6MWT Correlated with that After HAST (r = 0.52)
- Study of Algorithm Using Resting/6WMT SpO2 and HAST in COPD Patients (Thorax, 2012) [MEDLINE]
- Baseline SpO2 <92%: supplemental oxygen is required for air travel
- Baseline SpO2 92-95%
- 6MWT SpO2 <84%: supplemental oxygen is required for air travel
- 6MWT SpO2 ≥84%:
- HAST SpO2 ≤85%: supplemental oxygen is required for air travel
- HAST SpO2 >85%: no supplemental oxygen is required for air travel
- Baseline SpO2 >95%
- 6MWT SpO2 <84%
- HAST SpO2 ≤85%: supplemental oxygen is required for air travel
- HAST SpO2 >85%: no supplemental oxygen is required for air travel
- 6MWT SpO2 ≥84%: no supplemental oxygen is required for air travel
- 6MWT SpO2 <84%
Hypoxemia/Hypoxemic Respiratory Failure (see Hypoxemia and Respiratory Failure)
Clinical Conditions
- Type I-Hypoxemic Respiratory Failure
- Acute Hypoxemic Respiratory Failure
- Chronic Hypoxemic Respiratory Failure
- Type II-Hypoxemic, Hypercapnic Respiratory Failure
- Acute Hypoxemic, Hypercapnic Respiratory Failure
- Chronic Hypoxemic, Hypercapnic Respiratory Failure
Indications for Long-Term Oxygen Therapy in Chronic Lung Disease (Am J Respir Crit Care Med, 2018) [MEDLINE]
- Resting pO2 ≤55 mm Hg or SpO2 ≤88%
- If the Patient Meets Oxygen Therapy Criteria at Rest, Oxygen Should Also Be Used During Sleep and Exercise (with Appropriate Titration to Meet Needs)
- Resting pO2 ≤59 mm Hg or SpO2 ≤89% with Evidence of Cor Pulmonale
- If the Patient Meets Oxygen Therapy Criteria at Rest, Oxygen Should Also Be Used During Sleep and Exercise (with Appropriate Titration to Meet Needs)
- Evidence of Cor Pulmonale
- P-Pulmonale on EKG
- Hematocrit >55%
- Clinical Signs of Right Heart Failure
- Normal Resting pO2 ≥60 mm Hg or SpO2 ≥90% with Sleep-Associated Desaturation (pO2 ≤55 mm Hg or SpO2 ≤88% or Decrease in pO2 >10 mm Hg or Decrease in SpO2 >5%) and Signs of Nocturnal Hypoxemia (Impaired Cognitive Function, Morning Headache, Restlessness, Insomnia), Due to Either Lung Disease or Sleep Apnea Unresponsive to CPAP Therapy
- In These Cases, Oxygen Therapy Should Be Prescribed for Sleep Only
- Exercise-Associated Desaturation (pO2 ≤55 mm Hg or SpO2 ≤88%)
- In These Cases, Oxygen Therapy Should Be Prescribed for Exercise Only
- Exercise-Associated Dyspnea or Ventilatory Limitation Which May Benefit from Oxygen Therapy (Even in the Absence of Desaturation)
- Data Support this Approach in COPD Patients During Exercise (Chest, 2002) [MEDLINE]
Clinical Efficacy of Oxygen Therapy in Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
- Multicenter Nocturnal Oxygen Therapy Trial (NOTT) in Chronic Obstructive Pulmonary Disease Patients with Hypoxemia (Ann Intern Med, 1980) [MEDLINE]: n = 203 followed for ≥12 mos (mean: 19.3 mos)
- In Hypoxemic Chronic Obstructive Pulmonary Disease, Continuous Oxygen Therapy (Used at Least 18 hrs Per Day) Had Lower Mortality than Nocturnal Oxygen Therapy: nocturnal oxygen therapy group had 1.94x higher mortality than the continuous oxygen therapy group
- Benefit was Most Significant in Patients with Chronic Hypercapnia
- NOTT and MRC Trials Only Included Patients with More Severe Hypoxemia (pO2 ≤60 mm Hg), as Opposed to Other Trials Which Did Not Demonstrate a Benefit of Long-Term Oxygen Therapy, Which Also Included Less Severely Hypoxemic Patients (pO2 <69 mm Hg) (Am J Respir Crit Care Med, 2006) [MEDLINE]: indicates that COPD patients with less severe hypoxemia may not benefit from long-term oxygen therapy
- In Hypoxemic Chronic Obstructive Pulmonary Disease, Continuous Oxygen Therapy (Used at Least 18 hrs Per Day) Had Lower Mortality than Nocturnal Oxygen Therapy: nocturnal oxygen therapy group had 1.94x higher mortality than the continuous oxygen therapy group
- Medical Research Council (MRC) Trial of Oxygen Therapy in Chronic Obstructive Pulmonary Disease Patients with Severe Hypoxemia, Hypercapnia, and a History of Heart Failure (Lancet, 1981) [MEDLINE]: n = 87
- Oxygen Therapy (Used at Least 15 hrs Per Day) Improved the Mortality Rate
- NOTT and MRC Trials Only Included Patients with More Severe Hypoxemia (pO2 ≤60 mm Hg), as Opposed to Other Trials Which Did Not Demonstrate a Benefit of Long-Term Oxygen Therapy, Which Also Included Less Severely Hypoxemic Patients (pO2 <69 mm Hg) (Am J Respir Crit Care Med, 2006) [MEDLINE]: indicates that COPD patients with less severe hypoxemia may not benefit from long-term oxygen therapy
- Polish Trial of Oxygen Therapy in Patients with Chronic Obstructive Pulmonary Disease and Moderate Hypoxemia (Thorax, 1997) [MEDLINE]
- Oxygen Therapy Had No Mortality Benefit in Moderately Hypoxemic Chronic Obstructive Pulmonary Disease (with pO2 56-65 mm Hg)
- French Trial of Nocturnal Oxygen Therapy in Chronic Obstructive Pulmonary Disease with Mild-Moderate Daytime Hypoxemia (Eur Respir J, 1999) [MEDLINE]
- Nocturnal Oxygen Therapy Had No Mortality Benefit in Chronic Obstructive Pulmonary Disease with Daytime pO2 56-69 mm Hg and Nocturnal Desaturation
- Study of Hyperoxia in COPD Patients During Exercise (Eur Respir J, 2001) [MEDLINE]
- Hyperoxia Dose-Dependently Increases Exercise Endurance at Doses Up to 50% FIO2 (6 L/min)
- Review of Studies Which Suggest that Hyperoxia May Benefit COPD Patients During Exercise (Chest, 2002) [MEDLINE]
- Data Suggest that Oxygen Therapy May Benefit COPD Patients During Exercise, Even in the Absence of Desaturation
- Trial of Oxygen Therapy in Chronic Obstructive Pulmonary Disease with Transient Exertional Hypoxemia (Am J Respir Crit Care Med, 2007) [MEDLINE]
- Oxygen Therapy Improved the 5-Minute Distance Walked (But Not Dyspnea) in Chronic Obstructive Pulmonary Disease with Resting pO2 >60 mm Hg
- Trial of Oxygen Therapy in Chronic Obstructive Pulmonary Disease During Exercise (Thorax, 2007) [MEDLINE]
- Oxygen Therapy During Exercise Shortened Recovery Time in Chronic Obstructive Pulmonary Disease
- LOTT Trial of Oxygen Therapy in Moderately Hypoxemic Chronic Obstructive Pulmonary Disease (NEJM, 2016) [MEDLINE]
- Oxygen Therapy Demonstrated No Benefit in Terms of Mortality of Time to First Hospitalization in Moderately Hypoxemic Chronic Obstructive Pulmonary Disease (SpO2 89-93%)
- Randomized, Controlled Trial of Oxygen vs Air-Driven Nebulizers in the Treatment of COPD Exacerbation (BMC Pulm Med, 2018) [MEDLINE]
- Oxygen-Driven nebulisation leads to an increase in PtCO2 in exacerbations of COPD
Clinical Efficacy of Oxygen Therapy in Interstitial Lung Disease (ILD) (see Interstitial Lung Disease)
- Systematic Review of Oxygen Therapy in Patients with Interstitial Lung Disease Who are Normoxemic at Rest, But Desaturate with Exercise (Cochrane Database Syst Rev, 2016) [MEDLINE]
- In Patients with Interstitial Lung Disease Who are Normoxemic at Rest But Desaturate with Exertion, No Evidence Exists to Support the Use of Ambulatory or Short-Burst Oxygen Therapy, in Terms of Impact on Exercise Capacity, Dyspnea, and Quality of Life
- Evidence is Lacking Due to the Limited Number of Included Studies and Data
- In Patients with Interstitial Lung Disease Who are Normoxemic at Rest But Desaturate with Exertion, No Evidence Exists to Support the Use of Ambulatory or Short-Burst Oxygen Therapy, in Terms of Impact on Exercise Capacity, Dyspnea, and Quality of Life
- Randomized Australian/New Zealand Trial of Oxygen Therapy (vs Air) Delivered Via Portable Concentrator to Patients with Fibrotic Interstitial Lung Disease (Chest, 2020) [MEDLINE]: n = 30 (patients with interstitial lung disease and isolated exertional desaturation to <90% on 6-minute walk test)
- No Significant Difference in 6-Minute Walk Test Distance was Demonstrated Between the Air vs Oxygen Groups at Week 12 (Mean Difference of -34 m [95% CI: -105 to 36], P = 0.34)
- As Compared to the Air Group, the Oxygen Group Had a Significantly Higher Leicester Cough Questionnaire Psychological Domain Score, Indicating Better Cough-Related Quality of Life (Mean Difference of 0.9; 95% CI: 0.2 to 1.6], P = 0.01), But a Shorter Duration of Moderate-to-Vigorous Activities (Mean Difference of -135 [95% CI, -267 to -3], P = 0.04) at Week 12
Clinical Efficacy of Oxygen Administration in Acute Respiratory Failure (see Respiratory Failure)
- Randomized Trial of Conservative Oxygen Strategy in Mechanically-Ventilated Patients (Am J Respir Crit Care Med, 2016) [MEDLINE]
- Conservative Oxygen Strategy (SpO 88-92%) Did Not Impact the ICU or 90-Day Mortality Rate or Risk of Organ Dysfunction, as Compared to Liberal Oxygen Strategy (SpO2 ≥96%)
- Italian Oxygen-ICU Trial of Conventional Oxygen Strategy (pO2 Up to 150 mm Hg or SaO2 97-100%) vs Conservative Oxygen Strategy (pO2 70-100 or SaO2 94-98%) in a General ICU Population (Stay of ≥72 hrs) (JAMA, 2016) [MEDLINE]: trial had unplanned, early termination
- Conservative Oxygen Strategy Decreased Mortality Rate, as Compared to the Conventional Oxygen Strategy
- French HYPERS2S Trial of Hyperoxia and Hypertonic Saline in Septic Shock (Lancet Respir Med, 2017) [MEDLINE]
- Trial Stopped Prematurely for Safety Reasons
- Setting FiO2 to 100% to Induce Arterial Hyperoxia Might Increase the Mortality Rate in Septic Shock
- Hypertonic (3%) Saline Resuscitation Did Not Decrease the Mortality Rate in Septic Shock
- Improving Oxygen Therapy in Acute-illness (IOTA) Systematic Review and Meta-Analysis of Conservative vs Liberal Oxygen Strategy in Critically Ill Patients (Lancet, 2018) [MEDLINE]: n = 25 trials (in patients with sepsis, critical illness, stroke, trauma, myocardial infarction, cardiac arrest, and emergency surgery)
- In Acutely Ill Adults, Liberal Oxygen Therapy Strategy (Median SaO2 96%, Range 94-99%) Increases the 30-Day (and Longest Follow-Up) Mortality Rate, as Compared to a Conservative Oxygen Therapy Strategy (Relative Risk at 30 Days was 1.21, 95% CI 1.03-1.43)
- Supplemental Oxygen Might Become Unfavorable with SaO2 >94-96%
- In Acutely Ill Adults, Liberal Oxygen Therapy Strategy (Median SaO2 96%, Range 94-99%) Increases the 30-Day (and Longest Follow-Up) Mortality Rate, as Compared to a Conservative Oxygen Therapy Strategy (Relative Risk at 30 Days was 1.21, 95% CI 1.03-1.43)
- Post Hoc Analysis of HYPERS2S Trial Data (Ann Intensive Care, 2018) [MEDLINE]
- Hyperoxia May Be Associated with a Increased Mortality Rate in Patients with Septic Shock Using the Sepsis-3 Criteria (with Serum Lactate > 2 mmol/L), But Not in Patients with Hypotension Alone
- In Patients with Serum Lactate ≤2 mmol/L, Hyperoxia Had No Effect on the Mortality Rate, Nor on Other Outcomes
- Hyperoxia May Be Associated with a Increased Mortality Rate in Patients with Septic Shock Using the Sepsis-3 Criteria (with Serum Lactate > 2 mmol/L), But Not in Patients with Hypotension Alone
- Observational Study of Hyperoxia in the Emergency Department in Patients with Acute Respiratory Failure (Crit Care, 2018) [MEDLINE]: n = 688
- Emergency Department Exposure to Hyperoxia is Common and Associated with Increased Mortality in Mechanically Ventilated Patients Achieving Normoxia After Admission
- This Suggests that Hyperoxia in the Immediate Post-Intubation Period Could Be Particularly Injurious and Targeting Normoxia from Initiation of Mechanical Ventilation May Improve Outcome
- Australian/New Zealand ICU-ROX Trial of Conservative Oxygen Strategy in Mechanically-Ventilated Patients in the ICU (NEJM, 2020) [MEDLINE]: n = 1000
- RCT of Conservative Oxygen Therapy Using SpO2 <97%
- There was No Difference Between Conservative Oxygen Group (Median Duration: 21.3 Days; Interquartile Range: 0-26.3) and Usual Care Oxygen Group (Median Duration: 22.1 days; Interquartile Range: 0-26.2), in Terms of Number of Ventilator-Free Days
- The Conservative Oxygen Group Spent More Time in the ICU (Median Duration: 29 hrs; Interquartile Range: 5-78) ) with an FiO2 of 21% than the Usual Care Oxygen Group (Median Duration: 1 hr; Interquartile Range: 0-17)
- The Conservative Oxygen Group Spent Less Time with an SpO2 >96% (Median Duration: 27 hrs; Interquartile Range: 11-63.5) than the Usual Care Oxygen Group (Median Duration: 49 hrs; Interquartile Range: 22-112)
- At 180 days, Mortality was 35.7% in the Conservative Oxygen Group and 34.5% in the Usual Care Oxygen Group, for an Unadjusted Odds Ratio of 1.05 (95% CI: 0.81-1.37)
- French Multicenter, Randomized, Liberal or Conservative Oxygen 2 (LOCO2) Trial in ARDS (NEJM, 2020) [MEDLINE]: n= 205
- In ARDS, Early Conservative Oxygen Strategy (Target pO2 55-70 mm Hg or SpO2 88-92%) Did Not Improve 28-Day Survival, as Compared to Liberal Oxygen Strategy (Target pO2 90-105 mm Hg or SpO2 ≥96%) When Used for 7 Days
- Same Mechanical Ventilation Strategy was Used in Both Groups
- Multicenter, Randomized HOT-ICU Trial of Lower or Higher Oxygenation Targets for Acute Hypoxemic Respiratory Failure (NEJM, 2021) [MEDLINE]: n = 2928
- Enrolled Patients Who Had Recently Been Admitted to the ICU (≤12 hrs Before Randomization) and Who were Receiving ≥10 Liters of Oxygen Per Minute in an Open System or Had a Fraction of Inspired Oxygen ≥50% in a Closed System to Receive Oxygen Therapy Targeting a pO2 of Either 60 mm Hg (Lower Oxygenation Group) or 90 mm Hg (Higher Oxygenation Group) for a Maximum of 90 Days
- At 90 Days, There was No Difference in Mortality Rate Between the Low Oxygenation (42.9%) and High Oxygenation (42.4%) Groups
- At 90 Days, There were No Significant Between-Group Difference in the Percentage of Days that Patients were Alive without Life Support or in the Percentage of Days They were Alive After Hospital Discharge
- The Percentage of Patients Who Had New Episodes of Shock, Myocardial Ischemia, Ischemic Stroke, or Intestinal Ischemia were Similar in the Two Groups
- Dutch Randomized, Multicenter O2-ICU Trial of Low (60-90 mm Hg) vs High (105-135 mm Hg) Oxygenation Targets in Critically Ill Patients (with ≥2 SIRS Criteria and Expected ICU Stay >48 hrs) (JAMA, 2021) [MEDLINE]: n = 574
- Comparing Low-Normal to High-Normal pO2 Groups, There was No Significant Difference in the Median Duration of Mechanical Ventilation (3.4 vs 3.1 Days; Median Difference, -0.15 [95% CI, -0.88 to 0.47]; p = 0.59)
- Comparing Low-Normal to High-Normal pO2 Groups, There was No Significant Difference in the In-Hospital Mortality Rate (32% vs 31%; Odds Ratio, 1.04 [95% CI, 0.67 to 1.63]; p = 0.91)
- Comparing Low-Normal to High-Normal pO2 Groups, There was No Significant Difference in the Risk of Acute Kidney Failure (10% vs 11%)
- Comparing Low-Normal to High-Normal pO2 Groups, There was No Significant Difference in the Risk of Acute Myocardial Infarction (2.9% vs 3.6%)
Clinical Efficacy of High-Flow Nasal Cannula for Acute Respiratory Failure (see Respiratory Failure)
- Randomized Trial Comparing Non-Rebreather Mask and High-Flow Nasal Cannula Following Endotracheal Extubation (Respir Care, 2014) [MEDLINE]
- High-Flow Nasal Cannula Improves Dyspnea, Respiratory Rate, and Heart Rate, as Compared to Nasal Cannula
- Patients Preferred High-Flow Nasal Cannula to Non-Rebreather Mask
- Trial of High-Flow Nasal Cannula vs Venturi Mask Following Extubation (Am J Respir Crit Care Med, 2014) [MEDLINE]
- After Extubation, High-Flow Nasal Cannula Resulted in Improved Oxygenation at the Same FIO2, as Compared to Venturi Mask
- High-Flow Nasal Cannula Provided Better Comfort, Fewer Oxygen Desaturations, Fewer Interface Displacements, and a Lower Reintubation Rate
- Korean Tertiary Center Trial of High-Flow Nasal Cannula in Acute Respiratory Failure (Intensive Care Med, 2015) [MEDLINE]
- Failure of High-Flow Nasal Cannula Therapy May Delay Intubation and Worsen Clinical Outcome in Acute Respiratory Failure
- French/Belgian FLORALI Randomized Study Comparing High-Flow Nasal Cannula Oxygen with Standard Oxygen and Non-Invasive Ventilation in Hypoxemic, Non-Hypercapnic Respiratory Failure (NEJM, 2015) [MEDLINE]: n = 313
- Patient Population Consisted of Patients with pO2/FIO2 Ratio <300
- Approximately 66% of Patients Had CAP
- Approximately 10% of Patients Had HAP
- Despite a Trend, There was No Statistically Significant Difference in Intubation Rates (Primary Outcome) Between the HFNC (38%), Standard Oxygen (47%), and NIPPV (50%) Groups (p = 0.18)
- HFNC Group Had a Significantly Higher Number of Ventilator-Free Days at Day 28, as Compared to Standard Oxygen and NIPPV
- HFNC Decreased the Hazard Ratio for 90-Day Mortality, as Compared to Standard Oxygen and NIPPV
- In Post-Hoc Analysis in the Subset of Patients with pO2/FiO2 Ratio ≤200, HFNC Group Had Significantly Decreased the Intubation Rate, as Compared to Standard Oxygen and NIPPV
- HFNC Increased Patient Comfort and Decreased Dyspnea, as Compared to Standard Oxygen and NIPPV
- Criticism of Study: the noninvasive ventilation group was unconventionally ventilated with 9 mL/kg PBW, possibly increasing lung injury in this group
- Patient Population Consisted of Patients with pO2/FIO2 Ratio <300
- Spanish Multicenter, Randomized Trial of High-Flow Nasal Cannula Post-Extubation (JAMA, 2016) [MEDLINE]: n = 527
- Population was Deemed to Be at Low Risk for Reintubation
- Absence of Congestive Heart Failure (CHF), Moderate-Severe Chronic Obstructive Pulmonary Disease (COPD), Airway Patency Problems, and Prolonged Mechanical Ventilation
- Adequate Secretion Management
- Age <65 y/o
- APACHE II <12 on Day of Extubation
- BMI <30
- Comorbidity 0-1
- Simple Weaning
- In Extubated Patients at Low Risk of Reintubation, High-Flow Nasal Cannula Decreased the Risk of Reintubation within 72 hrs, as Compared to Conventional Oxygen Therapy
- Critiques of Trial: problems with blinding in the trial, high proportion of postoperative and neurologic patients (in whom high-flow nasal cannula may have improved secretion clearance)
- Population was Deemed to Be at Low Risk for Reintubation
- Systematic Review and Meta-Analysis of High-Flow Nasal Cannula in Acute Respiratory Failure (Due to Postoperative Respiratory Failure, Post-Extubation Respiratory Failure, and Medical Respiratory Failure) (Crit Care Med, 2017) [MEDLINE]: n= 13 trials
- High-Flow Nasal Cannula Did Not Significantly Decrease the Rate of Intubation (10% vs 16%)
- High-Flow Nasal Cannula Did Not Improve the Mortality Rate (6%), as Compared to Usual Care (8%)
- High-Flow Nasal Cannula is Well-Tolerated
- Further Randomized Trials are Recommended
- Systematic Review and Meta-Analysis Comparing High-Flow Nasal Cannula vs Standard Oxygen vs NIPPV in Acute Respiratory Failure (Chest, 2017) [MEDLINE]
- High-Flow Nasal Cannula and NIPPV Comparably Decreased the Intubation Rate in Acute Respiratory Failure, as Compared to Standard Oxygen Therapy in Acute Respiratory Failure
- Meta-Analysis Examining High-Flow Nasal Cannula in Acute Hypoxemic Respiratory Failure (CMAJ, 2017) [MEDLINE]
- The Intubation Rate with High-Flow Nasal Cannula Oxygen was Lower than the Rate with Conventional Oxygen Therapy and Similar to the Rate with NIPPV in Patients with Acute Hypoxemic Respiratory Failure
- French Randomized HIGH Trial of High-Flow Nasal Cannula vs Standard Oxygen Therapy in Immunocompromised Patients with Acute Hypoxemic Respiratory Failure (JAMA, 2018) [MEDLINE]: n = 776
- Day 28 Mortality Rate was Not Significantly Different Between the Groups (35.6% vs 36.1%; difference, -0.5% [95% CI, -7.3% to +6.3%]; Hazard Ratio, 0.98 [95% CI, 0.77 to 1.24]; P = .94)
- Intubation Rate was Not Significantly Different Between the Groups (38.7% vs 43.8%; difference, -5.1% [95% CI, -12.3% to +2.0%])
- As Compared to Controls, High-Flow Oxygen Therapy Increased the pO2/Fio2 Ratio (150 vs 119; difference, 19.5 [95% CI, 4.4 to 34.6]) and Decreased the Respiratory Rate after 6 hrs (25/min vs 26/min; difference, -1.8/min [95% CI, -3.2 to -0.2])
- No Significant Difference was Observed in ICU Length of Stay (8 vs 6 days; difference, 0.6 [95% CI, -1.0 to +2.2]), ICU-Acquired Infections (10.0% vs 10.6%; Difference, -0.6% [95% CI, -4.6 to +4.1]), Hospital Length of Stay (24 vs 27 Days; Difference, -2 days [95% CI, -7.3 to +3.3]), or Patient Comfort and Dyspnea Scores
- Italian HENIVOT Trial of Helmet Noninvasive Ventilation vs High-Flow Nasal Cannula Oxygen in Moderate-Severe Acute Hypoxemic Respiratory Failure Due to COVID-19 Virus Infection (JAMA, 2021) [MEDLINE]: n = 110
- Rate of Endotracheal Intubation was Significantly Lower in the Helmet Group, as Compared to the High-Flow Nasal Cannula Oxygen Group (30% vs 51%; Difference, -21% [95% CI: -38% to -3%]; P = 0.03)
- Median Number of Days Free of Invasive Mechanical Ventilation within 28 Days was Significantly Higher in the Helmet Group, as Compared to the High-Flow Nasal Cannula Oxygen Group (28 [IQR, 13-28] vs 25 [IQR 4-28]; Mean Difference, 3 days [95% CI: 0-7]; P = 0.04)
- Median Days Free of Respiratory Support within 28 Days After Randomization were 20 (IQR, 0-25) in the Helmet Group and 18 (IQR, 0-22) in the High-Flow Nasal Cannula Oxygen Group (Mean Difference of 2 Days [95% CI: -2 to 6]; P = 0.26 -> Not Statistically Significant)
- In-Hospital Mortality Rate was 24% in the Helmet Group and 25% in the High-Flow Nasal Cannula Oxygen Group (Absolute Difference -1% [95% CI: -17% to 15%]; P > 0.99 -> Not Statistically Significant)
- Review of High-Flow Nasal Cannula vs Conventional Oxygen Therapy vs Noninvasive Positive-Pressure Ventilation in Patients with Acute Respiratory Failure (Ann Intern Med, 2021) [MEDLINE]
- In the Initial Management of Acute Respiratory Failure, as Compared to Conventional Oxygen Therapy
- HFNC Did Not Impact All-Cause Mortality Rate (26.3% vs 27.2%; Absolute Risk Difference was -0.8 Percentage Points [95% CI: -4.9 to 3.8 Percentage Points]) (n= 4 Studies, Low-Certainty Evidence)
- In the Initial Management of Acute Respiratory Failure, as Compared to NIPPV
- HFNC Decreased All-Cause Mortality (12.4% vs 28.2%; Absolute Risk Difference was -15.8 Percentage Points [95% CI: -21.4 to -5.9 Percentage Points]) (n = 1 Studies, Low-Certainty Evidence)
- HFNC Decreased the Intubation Rate (23.0% vs 32.4%; Absolute Risk Difference was -9.4 Percentage Points [95% CI: -15.2 to -1.6 Percentage Points]) (Pooled Results from n = 2 Studies, Low-Certainty Evidence)
- HFNC Decreased the Rate of Hospital-Acquired Pneumonia (3.8% vs 8.2%; Absolute Risk Difference was -4.4 Percentage Points [CI, -7.0 to 3.7 Percentage Points]) (n = 1 Studies, Low-Certainty Evidence)
- Insufficient Data to Address Whether HFNC Decreased the ICU Admission Rate or ICU Length of Stay
- HFNC Did Not Impact Hospital Length of Stay (Mean Difference was 0.45 Days [95% CI: -0.69 to 1.59 Days]; I2 = 0%) (n = 2 Studies, Low-Certainty Evidence)
- HFNC May Improve Patient Comfort, But Did Not Improve Dyspnea (n = 7 Studies, Low-Certainty Evidence)
- In the Management of Post-Extubation Acute Respiratory Failure, as Conventional Oxygen Therapy
- HFNC Did Not Impact the All-Cause Mortality Rate (6.3% vs 6.2%; Absolute Risk Difference was 0.1 Percentage Points [95% CI: 2.5 to 4.5 Percentage Points]) (n = 4 Studies, Low-Certainty Evidence)
- HFNC Slightly Decreased the Reintubation Rate (6.5% vs 10.4%; Absolute Risk Difference was -3.9 Percentage Points [95% CI: -7.8 to 5.3 Percentage Points]) (n = 7 Studies, Low-Certainty Evidence)
- In the Management of Post-Extubation Acute Respiratory Failure, as Compared to NIPPV
- HFNC Slightly Increased the All-Cause Mortality Rate (12.9% vs 11.2%; Absolute Risk Difference was 1.7 Percentage Points [95% CI: -1.3 to 5.7 Percentage Points]) (n = 3 Studies, Low Certainty Evidence)
- HFNC Slightly Increased the Reintubation Rate (17.3% vs 15.3%; Absolute Risk Difference was 2.0 Percentage Points [95% CI: -1.5 to 6.6 Percentage Points]) (n = 3 Studies, Low Certainty Evidence)
- HFNC Did Not Impact Rate of Hospital-Acquired Pneumonia (13.2% vs 14.7%; Absolute Risk Difference was -1.5 Percentage Points [95% CI: -4.4 to 2.3 Percentage Points]) (n = 2 Studies, Low-Certainty Evidence)
- In the Initial Management of Acute Respiratory Failure, as Compared to Conventional Oxygen Therapy
Clinical Efficacy of High-Flow Nasal Cannula Postextubation
- Randomized, Controlled, Open-Label Trial of High-Flow Nasal Cannula in Extubated Patients with pO2/FIO2 <300 (J Crit Care, 2010) [MEDLINE]: n = 105
- After Extubation, High-Flow Nasal Cannla was Associated with Improved Oxygenation for the Same FGIO2, as Compared to Venturi Mask
- Trial of High-Flow Nasal Cannula in Extubated Patients Who Required High-Flow Oxygen (Am J Respir Crit Care Med, 2014) [MEDLINE]
- After Extubation, High-Flow Nasal Cannula were as Effective as High-Flow Face Mask Oxygen
- Tolerance of High-Flow Nasal Cannula was Better than High-Flow Face Mask
- French Multicenter Randomized OPERA Study of Early Postextubation High-Flow Nasal Cannula After Major Abdominal Surgery (Intensive Care Med, 2016) [MEDLINE]: n = 220
- In Patients Undergoing Major Abdominal Surgery, Early Postextubation Preventive High-Flow Nasal Cannula Oxygen Did Not Result in Improved Pulmonary Outcomes, as Compared with Standard Oxygen Therapy
- Spanish Randomized Trial of High-Flow Nasal Cannula Oxygen in Patients at Low Risk for Reintubation (JAMA, 2016) [MEDLINE]: n = 527
- In Extubated Patients at Low Risk for Reintubation, the High-Flow Nasal Cannula Oxygen Decreased the Risk of Reintubation within 72 hrs, as Compared to Conventional Oxygen Therapy
- Review of High-Flow Nasal Cannula vs Conventional Oxygen Therapy vs Noninvasive Positive-Pressure Ventilation in Patients with Acute Respiratory Failure (Ann Intern Med, 2021) [MEDLINE]
- In the Initial Management of Acute Respiratory Failure, as Compared to Conventional Oxygen Therapy
- HFNC Did Not Impact All-Cause Mortality Rate (26.3% vs 27.2%; Absolute Risk Difference was -0.8 Percentage Points [95% CI: -4.9 to 3.8 Percentage Points]) (n= 4 Studies, Low-Certainty Evidence)
- In the Initial Management of Acute Respiratory Failure, as Compared to NIPPV
- HFNC Decreased All-Cause Mortality (12.4% vs 28.2%; Absolute Risk Difference was -15.8 Percentage Points [95% CI: -21.4 to -5.9 Percentage Points]) (n = 1 Studies, Low-Certainty Evidence)
- HFNC Decreased the Intubation Rate (23.0% vs 32.4%; Absolute Risk Difference was -9.4 Percentage Points [95% CI: -15.2 to -1.6 Percentage Points]) (Pooled Results from n = 2 Studies, Low-Certainty Evidence)
- HFNC Decreased the Rate of Hospital-Acquired Pneumonia (3.8% vs 8.2%; Absolute Risk Difference was -4.4 Percentage Points [CI, -7.0 to 3.7 Percentage Points]) (n = 1 Studies, Low-Certainty Evidence)
- Insufficient Data to Address Whether HFNC Decreased the ICU Admission Rate or ICU Length of Stay
- HFNC Did Not Impact Hospital Length of Stay (Mean Difference was 0.45 Days [95% CI: -0.69 to 1.59 Days]; I2 = 0%) (n = 2 Studies, Low-Certainty Evidence)
- HFNC May Improve Patient Comfort, But Did Not Improve Dyspnea (n = 7 Studies, Low-Certainty Evidence)
- In the Management of Post-Extubation Acute Respiratory Failure, as Compared to Conventional Oxygen Therapy
- HFNC Did Not Impact the All-Cause Mortality Rate (6.3% vs 6.2%; Absolute Risk Difference was 0.1 Percentage Points [95% CI: 2.5 to 4.5 Percentage Points]) (n = 4 Studies, Low-Certainty Evidence)
- HFNC Decreased the Reintubation Rate (6.5% vs 10.4%; Absolute Risk Difference was -3.9 Percentage Points [95% CI: -7.8 to 5.3 Percentage Points]) (n = 7 Studies, Low-Certainty Evidence)
- In the Management of Post-Extubation Acute Respiratory Failure, as Compared to NIPPV
- HFNC Slightly Increased the All-Cause Mortality Rate (12.9% vs 11.2%; Absolute Risk Difference was 1.7 Percentage Points [95% CI: -1.3 to 5.7 Percentage Points]) (n = 3 Studies, Low Certainty Evidence)
- HFNC Slightly Increased the Reintubation Rate (17.3% vs 15.3%; Absolute Risk Difference was 2.0 Percentage Points [95% CI: -1.5 to 6.6 Percentage Points]) (n = 3 Studies, Low Certainty Evidence)
- HFNC Did Not Impact Rate of Hospital-Acquired Pneumonia (13.2% vs 14.7%; Absolute Risk Difference was -1.5 Percentage Points [95% CI: -4.4 to 2.3 Percentage Points]) (n = 2 Studies, Low-Certainty Evidence)
- In the Initial Management of Acute Respiratory Failure, as Compared to Conventional Oxygen Therapy
Clinical Efficacy of High-Flow Nasal Cannula in Tracheostomy Patients Who are Weaning (see Tracheostomy)
- Randomized Crossover Trial of High-Flow Oxygen During Tracheostomy Weaning (Intensive Care Med, 2017) [MEDLINE]
- High-Flow Nasal Cannula Oxygen During Tracheostomy Weaning (50 L/min) Had Higher SaO2 for a Given FIO2 (Which Permitted a Lower FIO2), as Compared to 15 L/min Oxygen Via T-Piece
Clinical Efficacy of High-Flow Nasal Cannula During Bronchoscopy
- Small Trial of High-Flow Nasal Cannula During Bronchoscopy in Patients with Acute Respiratory Failure (Respir Investig, 2014) [MEDLINE]: n = 5
- High-Flow Nasal Cannula May Be Used to Support Oxygenation During Bronchoscopy
- German Prospective Randomized Trial of High-Flow Nasal Cannula vs Noninvasive Positive-Pressure Ventilation During Bronchoscopy in Patients with Hypoxemic Respiratory Failure in the ICU (Crit Care, 2014) [MEDLINE]: n = 40
- Noninvasive Positive-Pressure Ventilation was Superior to High-Flow Nasal Cannula with Regard to Oxygenation Before, During, and After Bronchoscopy in Patients with Moderate-Severe Hypoxemia
American College of Physicians Clinical Guideline Recommendations for the Use of High-Flow Nasal Cannula for the Management of Acute Respiratory Failure (Ann Intern Med, 2021) [MEDLINE]
- Initial Management of Acute Hypoxemic Respiratory Failure in Hospitalized Adults
- American College of Physicians Suggests that Clinicians Use High-Flow Nasal Cannula Oxygen, Rather than Noninvasive Positive-Pressure Ventilation (NIPPV) (Conditional Recommendation; Low-Certainty Evidence)
- Management of Postextubation Acute Hypoxemic Respiratory Failure in Hospitalized Adults
- American College of Physicians Suggest that Clinicians Use High-Flow Nasal Cannula Oxygen, Rather than Conventional Oxygen Therapy (conditional recommendation; Low-Certainty)
Ischemic Cerebrovascular Accident (CVA) (see Ischemic Cerebrovascular Accident)
Clinical Efficacy
- SO2S Study of Oxygen in Acute Ischemic Cerebrovascular Accident (JAMA, 2017) [MEDLINE]
- Among Non-Hypoxemic Patients with Acute Stroke, Prophylactic Use of Low-Dose Oxygen Supplementation Did Not Decrease Death or Disability at 3 Months
Recommendations (American Heart Association/American Stroke Association Acute Ischemic Stroke Guidelines, 2013) [MEDLINE]
- Supplemental Oxygen Should Be Provided to Maintain SaO2 >94% (Class I, Level of Evidence C)
- Supplemental Oxygen is Not Recommended in Normoxemic Patients with Acute Ischemic Stroke (Class III, Level of Evidence B)
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- In Patients with Myocardial Infarction/Stroke, Supplemental Oxygen is Not Recommended for Patients with SpO2 >92% Due to No Likely Benefit and Possible Risk of Harm (Strong Recommendation)
- In Patients with Myocardial Infarction/Stroke, Supplemental Oxygen is Not Recommended for Patients with SpO2 90-92% Due to No Likely Benefit and Possible Risk of Harm (Weak Recommendation)
Methemoglobinemia (see Methemoglobinemia)
Rationale
- Supplemental Oxygen is Commonly Used to Treat Tissue Hypoxia
Clinical Efficacy
- xxxx
Palliative Treatment of Dyspnea (see Dyspnea)
Clinical Efficacy
- Review of Oxygen Therapy in the Palliative Treatment of Non-Hypoxemic Dyspneic Patients (Expert Rev Respir Med, 2013) [MEDLINE]
- Oxygen Therapy May Not Be Beneficial in Such Settings (and Compressed Air May Be Just as Beneficial)
Pneumothorax (see Pneumothorax)
Rationale
- xxxx
Clinical Efficacy
- XXXXX
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- Higher SpO2 Target (Approaching 100%) is Probably Recommended
Pulmonary Hypertension (see Pulmonary Hypertension)
Clinical Efficacy
- Observational Data from Pulmonary Hypertension Patients in the REVEAL Trial (J Heart Lung Transplant, 2018) [MEDLINE]
- In Patients with Pulmonary Hypertension and Severely Decreased DLCO, Supplemental Oxygen Decreased the Mortality Rate
- Authors Recommended a Randomized Trial to Address This Further
Sickle Cell Crisis (see Sickle Cell Disease)
Clinical Efficacy
- xxxx
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- Higher SpO2 Target (Approaching 100%) is Probably Recommended
Supportive Therapy During General Anesthesia
Rationale
- Oxygen is Commonly Utilized in this Setting
Pharmacology
Background
- Typical Nasal Flow Rate (At Rest): 12 L/min
- Typical Nasal Flow Rate (During Respiratory Distress): up to 30-120 L/min
Administration
Target Peripheral Oxygen Saturation (SpO2) or Arterial Partial Pressure of Oxygen (pO2)
Disorders in Which Lower SpO2 Target is Recommended (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- Disorders with Chronic Type II-Hypoxemic, Hypercapnic Respiratory Failure
- Chronic Obstructive Pulmonary Disease (COPD) with Chronic Hypoventilation (see Chronic Obstructive Pulmonary Disease)
- Trials of High-Flow Oxygen in Chronic Obstructive Pulmonary Disease (in the Pre-Hospital Setting) Indicate that Excessive Oxygen Should Be Avoided, Due to the Risk of Worsening Hypercapnia (BMJ, 2010) [MEDLINE]
- Disorders with Decreased Central Respiratory Drive (Selected Disorders)
- Brainstem Ischemic Cerebrovascular Accident (CVA)/Hemorrhage (see Ischemic Cerebrovascular Accident or Intracerebral Hemorrhage)
- Sedative Overdose
- Encephalitis (see Encephalitis)
- Neuromuscular Disease with Chronic Hypoventilation (Selected Disorders)
- Amyotrophic Lateral Sclerosis (ALS) with Chronic Hypoventilation (see Amyotrophic Lateral Sclerosis)
- Obesity Hypoventilation Syndrome (OHS) (see Obesity Hypoventilation Syndrome)
- Obstructive Sleep Apnea (OSA) with Chronic Hypoventilation (see Obstructive Sleep Apnea)
- Chronic Obstructive Pulmonary Disease (COPD) with Chronic Hypoventilation (see Chronic Obstructive Pulmonary Disease)
Disorders in Which High SpO2 Target (Approaching SpO2 100%) is Recommended (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- Carboxyhemoglobinemia (see Carboxyhemoglobinemia)
- Cluster Headache (see Cluster Headache)
- Methemoglobinemia (see Methemoglobinemia)
- Pneumothorax (see Pneumothorax)
- Sickle Cell Crisis (see Sickle Cell Disease)
Clinical Efficacy-Long-Term Oxygen Therapy
- The Threshold SpO2 (or pO2) Which Optimally Improves Mortality and Quality of Life is Unknown
- In the NOTT Trial, Investigators Attempted to Maintain the pO2 Between 60-80 mm Hg (Ann Intern Med, 1980) [MEDLINE]: based on this, a pO2 of 60-65 mm Hg (or SpO2 of 90-92%) is typically considered a reasonable target
Clinical Efficacy-Oxygen Therapy in Hospitalized Patient
- French HYPERS2S Trial of Hyperoxia and Hypertonic Saline in Septic Shock (Lancet Respir Med, 2017) [MEDLINE]
- Trial Stopped Prematurely for Safety Reasons
- Setting FiO2 to 100% to Induce Arterial Hyperoxia Might Increase the Mortality Rate in Septic Shock
- Hypertonic (3%) Saline Resuscitation Did Not Decrease the Mortality Rate in Septic Shock
- Italian Oxygen-ICU Trial of Conventional Oxygen Strategy (pO2 Up to 150 mm Hg or SaO2 97-100%) vs Conservative Oxygen Strategy (pO2 70-100 or SaO2 94-98%) in a General ICU Population (Stay of ≥72 hrs) (JAMA, 2016) [MEDLINE]: trial had unplanned, early termination
- Conservative Oxygen Strategy Decreased Mortality Rate, as Compared to the Conventional Oxygen Strategy
- Improving Oxygen Therapy in Acute-illness (IOTA) Systematic Review and Meta-Analysis of Conservative vs Liberal Oxygen Strategy in Critically Ill Patients (Lancet, 2018) [MEDLINE]: n = 25 trials (in patients with sepsis, critical illness, stroke, trauma, myocardial infarction, cardiac arrest, and emergency surgery)
- In Acutely Ill Adults, Liberal Oxygen Therapy Strategy (Median SaO2 96%, Range 94-99%) Increases the 30-Day (and Longest Follow-Up) Mortality Rate, as Compared to a Conservative Oxygen Therapy Strategy (Relative Risk at 30 Days was 1.21, 95% CI 1.03-1.43)
- Supplemental Oxygen Might Become Unfavorable with SaO2 >94-96%
- In Acutely Ill Adults, Liberal Oxygen Therapy Strategy (Median SaO2 96%, Range 94-99%) Increases the 30-Day (and Longest Follow-Up) Mortality Rate, as Compared to a Conservative Oxygen Therapy Strategy (Relative Risk at 30 Days was 1.21, 95% CI 1.03-1.43)
- Post Hoc Analysis of HYPERS2S Trial Data (Ann Intensive Care, 2018) [MEDLINE]
- Hyperoxia May Be Associated with a Increased Mortality Rate in Patients with Septic Shock Using the Sepsis-3 Criteria (with Serum Lactate > 2 mmol/L), But Not in Patients with Hypotension Alone
- In Patients with Serum Lactate ≤2 mmol/L, Hyperoxia Had No Effect on the Mortality Rate, Nor on Other Outcomes
- Hyperoxia May Be Associated with a Increased Mortality Rate in Patients with Septic Shock Using the Sepsis-3 Criteria (with Serum Lactate > 2 mmol/L), But Not in Patients with Hypotension Alone
Recommendations (British Thoracic Society Emergency Oxygen Guidelines, 2017) (Thorax, 2017) [MEDLINE]
- Philosophy of the Guidelines
- Oxygen is a Treatment for Hypoxemia, not Dyspnea
- Oxygen Has Not Been Proven to Have Any Consistent Effect on the Sensation of Dyspnea in Non-Hypoxemic Patients
- Guideline Can Be Summarized as a Requirement for Oxygen to Be Prescribed According to a Target Saturation Range and for Those Who Administer Oxygen Therapy to Monitor the Patient and Keep within the Target Saturation Range
- Guideline Recommends Aiming to Achieve Normal or Near Normal Oxygen Saturation for All Acutely Ill Patients Except for Those at Risk of Hypercapnic Respiratory Failure or Those Receiving Terminal Palliative Care
- Oxygen is a Treatment for Hypoxemia, not Dyspnea
- Patient Assessment
- For Critically Ill Patients, High-Concentration Oxygen Should Be Administered Immediately
- Supplemental Oxygen is Given to Improve Oxygenation, But it Does Not Treat the Underlying Etiology of Hypoxemia Which Must Be Diagnosed and Urgently Treated
- Oxygen Saturation Should Be Checked by Pulse Oximetry in All Dyspneic and Acutely Ill Patients as the “Fifth Vital Sign” (Supplemented by Arterial Blood Gas, When Necessary) and the Inspired Oxygen Concentration Should Be Recorded in the Medical Record
- Pulse Oximetry Must Be Available in All Locations Where Emergency Oxygen is Utilized
- Clinical Assessment is Recommended if the Saturation Falls by ≥3% or Below the Target Range for the Patient
- All Critically Ill Patients Outside of a Critical Care Area (Intensive Care unit, etc) Should Be Assessed and Monitored Using a Recognized Physiological Track and Trigger System such as the National Early Warning Score
- SpO2 Target
- Oxygen Should Be Prescribed to Achieve a Target Saturation of 94–98% for Most Acutely Ill Patients or 88–92% or Patient-Specific Target Range for Those at Risk of Hypercapnic Respiratory Failure
- Best Practice is to Prescribe a Target Range for All Hospitalized Patients at the Time of Hospital Admission So that Appropriate Oxygen Therapy Can Be Started in the Event of Unexpected Clinical Deterioration with Hypoxemia and Also to Ensure that the Oximetry Section of the Early Warning Score Can Be Scored Appropriately
- Target Saturation Should Be Written in the Medical Record
- Oxygen Administration
- Oxygen Should Be Administered by Staff Who are Trained in Oxygen Administration
- These Staff Should Use Appropriate Devices and Flow Rates in Order to Achieve the Target Saturation Range
- Staff Should Be Trained in the Use of a Range of Different Oxygen Delivery Devices to Ensure Oxygen is Delivered Safely
- Monitoring and Maintenance of Target Saturation
- Oxygen Saturation and Delivery System (Including the Flow Rate) Should Be Recorded in the Medical Record
- Oxygen Delivery Devices and Flow Rates Should Be Adjusted to Keep the Oxygen Saturation in the Target Range
- Prompt Clinical Assessment is Required if Oxygen Therapy Needs to Be Initiated or Increased Due to Desaturation
- Oxygen Should Be Prescribed and a Signature Should Be Entered in the Medical Record
- Weaning and Discontinuation of Oxygen Therapy
- Oxygen Should Be Reduced in Stable Patients with Satisfactory Oxygen Saturation
- Oxygen Should Be Discontinued Once the Patient Can Maintain Saturation within or Above the Target Range Breathing Air, But the Prescription for a Target Range Should Be Left in Place in Case of Future Deterioration and to Guide Early Warning Score
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
- General Comments
- While the Guidelines are Specified for Use in Acutely Ill Medical Patients, the Authors Note that the Guidelines Can Be Generalized for Use in Critically Ill Medical and Surgical Patients
- However, the Guidelines are Not Applicable to the Use of Oxygen Therapy in Uncomplicated (Elective) Surgery and in Neonates, as These Groups of Patients are Addressed in Separate Bodies of Literature
- While the Guidelines are Specified for Use in Acutely Ill Medical Patients, the Authors Note that the Guidelines Can Be Generalized for Use in Critically Ill Medical and Surgical Patients
- Supplemental Oxygen Therapy Should Be Titrated to SpO2 ≤96% (Strong Recommendation)
- SpO2 >96% likely is Associated with a Small, But Important, Increased Risk of Death without Plausible Clinical Benefit
- In Patients with Myocardial Infarction/Stroke, Supplemental Oxygen is Not Recommended for Patients with SpO2 >92% Due to No Likely Benefit and Possible Risk of Harm (Strong Recommendation)
- In Patients with Myocardial Infarction/Stroke, Supplemental Oxygen is Not Recommended for Patients with SpO2 90-92% Due to No Likely Benefit and Possible Risk of Harm (Weak Recommendation)
Medicare Reimbursement for Oxygen Therapy
- Requirement for Assessment of Need for Oxygen Therapy
- If Oxygen is Being Prescribed at the Time of Hospital Discharge, SpO2 or Arterial Blood Gas (ABG) Must Be Performed within 2 Days of the Hospital Discharge
- Medicare (and Most Payors) Will Reimburse for the Cost of Oxygen Therapy as Long as a Certificate of Medical Necessity (CMN) Has Been Completed for the Patient
- Medicare Considers Oxygen as “Durable Medical Equipment” (DME), Not a Medication
- With Regard to Reimbursement, Medicare Does Not Differentiate Between Modalities of Oxygen Delivery (All Delivery Systems are Considered Equivalent)
- There is a Small Additional Reimbursement Provided for Patients Who Require a Portable Add-On Device
- Medicare Reimburses for 80% of the Cost of the Oxygen, with the Remaining 20% to Be Covered By the Patient or Supplemental Insurer
General Types of Oxygen Systems
- Oxygen Concentrator: for home use
- Lightweight Compressed Gas Cylinder: portable
- Liquid Oxygen System: portable
- Portable Oxygen Concentrator (POC): portable device (this is the only device which is currently approved for air travel)
- Devices: Eclipse, EverGo, FreeStyle, Inogen, XPO2
- Range of Battery Life 2.5-8 hrs
- Battery Power is Required for Oxygen Production
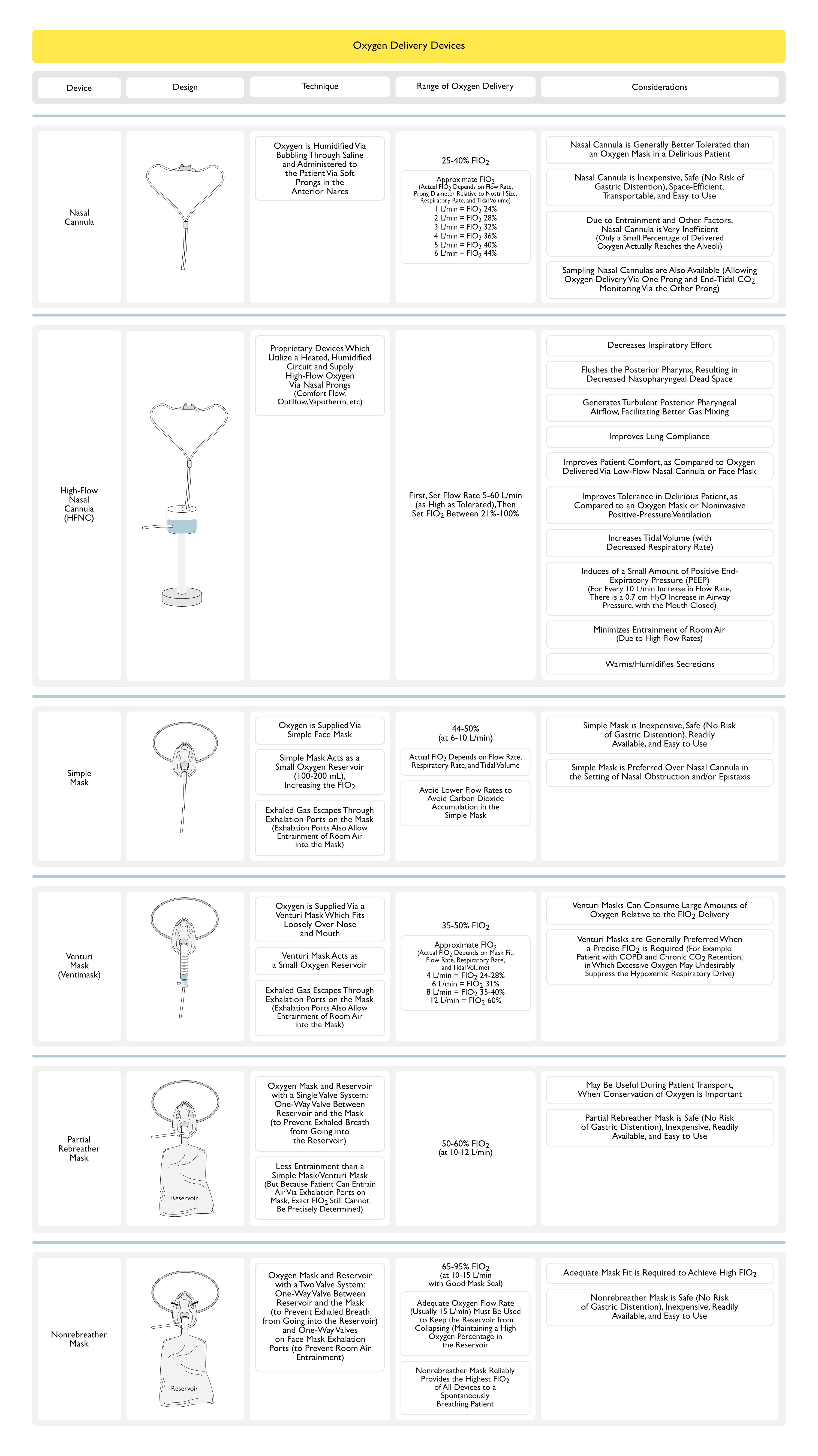
Nasal Cannula (NC)
Technique
- Oxygen is Supplied Via Soft Prongs in Anterior Nares
- Humidification Via Bubbling Through Saline is Standard Utilized, as Flows >2 L/min Can Be Irritating to the Nasal Mucosa
Range of Oxygen Delivery
- Range: 25-40% FIO2 (at flow rate 1-6 L/min)
- As a General Rule, Each Increase in Flow Rate of 1 L/min Accounts for an Approximate 4% Increase in FIO2
- However, the Actual FiO2 Delivered is Affected by Respiratory Rate, Tidal Volume, Oxygen Flow Rate, and the Amount of Mouth Breathing by the Patient (Thorax, 1992) [MEDLINE]
- Higher Respiratory Rate Results in Higher Amount of Air Entrainment and Therefore, Decreased FIO2
- In General, the Most Effective Oxygen Delivery Via Nasal Cannula Occurs During the First 200 msec of the Inspiration
- As a General Rule, Each Increase in Flow Rate of 1 L/min Accounts for an Approximate 4% Increase in FIO2
Considerations
- Nasal Cannula is Generally Better Tolerated than an Oxygen Mask in a Delirious Patient (Due to Claustrophobia, etc)
- Nasal Cannulas are Inexpensive, Space-Efficient, Transportable, and Easy to Use
- However, Due to Entrainment and Other Factors, Nasal Cannulas are Very Inefficient
- Only a Small Percentage of the Oxygen Being Delivered Through the Nasal Cannula Actually Reaches the Alveoli
High-Flow Nasal Cannula (HFNC)
Physiologic Effects and Clinical Benefits
- Decreases Inspiratory Effort
- Inspiratory Flow Rates Linearly Decrease the Inspiratory Effort, Improve Lung Aeration, Improve Dynamic Compliance, and Improve Oxygenation (Intensive Care Med, 2017) [MEDLINE]
- Notably, Most of the Effects on Inspiratory Workload and Carbon Dioxide Clearance were Achieved at the Lowest Flow Rates (Intensive Care Med, 2017) [MEDLINE]
- Inspiratory Flow Rates Linearly Decrease the Inspiratory Effort, Improve Lung Aeration, Improve Dynamic Compliance, and Improve Oxygenation (Intensive Care Med, 2017) [MEDLINE]
- Flushes the Posterior Pharynx, Resulting in Decreased Nasopharyngeal Dead Space (NEJM, 2015) [MEDLINE]
- Improves Efficiency of Ventilation and Oxygen Delivery
- Generates Turbulent Posterior Pharyngeal Airflow, Facilitating Better Gas Mixing
- Improves Lung Compliance
- Italian Prospective, Randomized Crossover Trial of High-Flow Nasal Cannula in Acute Hypoxemic Respiratory Failure (Am J Respir Crit Care Med, 2017) [MEDLINE]
- High-Flow Nasal Cannula Decreased Inspiratory Effort, Improved Lung Volumes, and Improved Lung Compliance
- Italian Prospective, Randomized Crossover Trial of High-Flow Nasal Cannula in Acute Hypoxemic Respiratory Failure (Am J Respir Crit Care Med, 2017) [MEDLINE]
- Improves Patient Comfort, as Compared to Oxygen Delivered Via Low-Flow Nasal Cannula or Face Mask (Respir Care, 2010) [MEDLINE] (J Crit Care, 2010) [MEDLINE] (Respir Care, 2014) [MEDLINE]
- Improves Tolerance in the Delirious Patient, as Compared to an Oxygen Mask or Noninvasive Positive-Pressure Ventilation
- Increases Tidal Volume (with Decreased Respiratory Rate) (Br J Anaesth, 2011) [MEDLINE] (Respir Care, 2013) [MEDLINE]
- Induces of a Small Amount of Positive End-Expiratory Pressure (PEEP)
- Amount of PEEP Achieved is Dose-Dependently Related to the Flow Rate (Respir Care, 2013) [MEDLINE]
- For Every 10 L/min Increase in the Flow Rate, there is a 0.7 cm H2O Increase in Airway Pressure (with the Mouth Closed) and 0.35 cm H20 Increase (with the Mouth Open) (Respir Care, 2011) [MEDLINE]
- With Open Mouth Breathing, Lower Levels of PEEP are Generally Observed
- Physiologic Consequences of the PEEP Effect
- Decreased Auto-PEEP (If Present)
- Decreased Work of Breathing: however, high-flow nasal cannula does not decrease the work of breathing as effectively as noninvasive positive-pressure ventilation (or invasive mechanical ventilation)
- Enhanced Oxygenation in the Setting of Alveolar Filling Processes (Pulmonary Edema, ARDS, etc)
- Amount of PEEP Achieved is Dose-Dependently Related to the Flow Rate (Respir Care, 2013) [MEDLINE]
- Minimizes Entrainment of Room Air (Due to High Flow Rates)
- Increases the Ability to Deliver a Higher FIO2
- Results in a More Accurate FIO2, as Compared to Other Delivery Systems
- This is Clinically Important, Since Patients in Respiratory Distress Can Generate Flow Rates Which Exceed Those Supplied by Many Conventional Oxygen Delivery Systems, Resulting in Entrainment of Room Air (and a Decreased FIO2)
- However, Open-Mouth Breathing Will Allow Entrainment of Room Air and Obviate this Advantage to Some Extent
- Warms/Humidifies Secretions
- Warming and Humidifying Oxygen is More Effective at High Flow Rates (>40 L/min) than at Low Flow Rates: therefore, high-flow nasal cannula systems are better at warming and humidifying than Venturi masks and non-rebreather masks (which use flow rates of 10-15 L/min) or low-flow rate delivery systems (which use flow rates <10 L/min)
- Increased Mucous Membrane Hydration Facilitates Secretion Clearance, Decreases Work of Breathing, and Decreases Mucous Membrane Dessication/Epithelial Injury
Technique
- Proprietary Devices
- Comfort Flo
- Optiflow
- Vapotherm
- Parameters to Set
- Flow Rate: while high-flow nasal cannula may utilize flow rates of 5-60 L/min, the flow rate is usually initially set at 20-35 L/min
- May Increase the Flow Rate in Increments of 5-10 L/min, as Required to Improve Oxygenation: this is usually performed to prioritize a decrease in FIO2 to ≤50%
- FIO2: set between 21%-100% to achieve desired SaO2
- May Increase (After Flow Rate is Maximized), as Required to Improve Oxygenation
- Flow Rate: while high-flow nasal cannula may utilize flow rates of 5-60 L/min, the flow rate is usually initially set at 20-35 L/min
- Heated, Humidified Circuit
- Delivery of Nebulized Medications (Albuterol, etc): usually performed using an oral delivery device (as opposed to via the high-flow nasal cannula device)
- The Efficiency of Delivery of Nebulized Medications Has Not Been Well-Studied with High-Flow Nasal Cannula Systems
- Duration of Use: may be used for prolonged period of time (multiple days)
- Transition Back to a Conventional Delivery Oxygen Delivery System: this can usually be achieved when the flow rate is ≤20 L/min and the FIO2 ≤50%
Indications
- Type I-Hypoxemic Respiratory Failure (see Respiratory Failure)
Contraindications
- Type II-Hypoxemic, Hypercapnic Respiratory Failure (see Respiratory Failure)
- Due to Concerns Related to the Worsening of Hypercapnia
- High-Flow Oxygen Administered to Patients with Chronic Obstructive Pulmonary Disease in the Pre-Hospital Setting Has Been Demonstrated to Worsen Hypercapnia (BMJ, 2010) [MEDLINE]: caution should be exercise when high-flow oxygen is used in this patient population
- Mid-Maxillary Facial Trauma or Upper Airway Surgery
- Due to Concern with Regard to High Pressure Precipitating Air Embolism
- Suspected Pneumothorax (see Pneumothorax)
- Due to Concerns Related to the Development of Barotrauma
Adverse Effects/Complications
- Barotrauma: although the risk of barotrauma with high-flow nasal cannula is lower than that with noninvasive positive-pressure ventilation or intubation with invasive mechanical ventilation
- Pneumomediastinum (se Pneumomediastinum)
- Pneumothorax (see Pneumothorax)
- Subcutaneous Emphysema (see Subcutaneous Emphysema)
- Gastric Distention (with Predisposition to Aspiration)
Venturi Mask (Ventimask)
Technique
- Simple Mask Which Fits Loosely Over the Nose and Mouth
- Plastic Mask Serves as an Oxygen Reservoir
- Exhaled Gas Escapes Through Exhalation Ports on the Mask: however, these exhalation ports also allow entrainment of room air into the mask (decreasing the effective FIO2)
- For This Reason, the Exact FIO2 Cannot Be Precisely Determined in an Individual Patient
- Flow Rate of >5 L/min is Recommended to Prevent Carbon Dioxide Rebreathing (Acta Anaesthesiol Scand, 1991) [MEDLINE]
Range of Oxygen Delivery
- Range: 35-50% FIO2 (at 6-10 L/min)
- The Actual FIO2 Delivered is Affected by the Patient’s Respiratory Rate and the Mask Fit
Considerations
- Percent Oxygen is Affected by Mask Fit and Patient’s Respiratory Rate
Partial Rebreather Mask
Technique
- Consists of a Simple Mask with an Attached Oxygen Reservoir
- Inspiratory Flow Comes Predominantly from the Oxygen Inflow from the Source and the Oxygen Reservoir
- While Entrainment of Room Air Via the Exhalation Ports is Usually Minimal (with Less Entrainment than a Simple Mask/Venturi Mask), the Exact FIO2 Still Cannot Be Precisely Determined in an Individual Patient
- Oxygen Flow Rate Must Be Adjusted to Keep the Reservoir from Collapsing, to Maintain a High Oxygen Percentage in the Reservoir
Range of Oxygen Delivery
- Range: 50-60% FIO2 (at flow rates 10-12 L/mi)
Considerations
- May Be Useful During Patient Transport, When Conservation of Oxygen is Important
Non-Rebreather (NRB) Mask
Technique
- Oxygen Mask and Reservoir System Which Contains Two Valves Which Limit the Mixing of Exhaled Gases and Room Air with the Oxygen Supply
- Only One of the Two Exhalation Ports Has a One-Way Valve
- This Safety Feature Allows the Patient to Still Obtain Room Air Through the Open Port, if the Oxygen Flow to the Mask is Interrupted for Some Reason
- The Second One-Way Valve is Located Between the Reservoir and the Mask and it Functions to Prevent the Flow of Exhaled Gas into the Reservoir
- Only One of the Two Exhalation Ports Has a One-Way Valve
- Oxygen Flow Rate Must Be Adjusted to Keep the Reservoir from Collapsing, to Maintain a High Oxygen Percentage in the Reservoir
Range of Oxygen Delivery
- Range: 65-95% FIO2 (at flow rates 10-15 L/min with a good mask seal)
- Non-Rebreather Mask Reliably Provides the Highest FIO2 of All Devices to a Spontaneously Breathing Patient
Considerations
- Adequate Mask Fit is Required to Achieve High FIO2
Blow By
Indications
- Spontaneously-Breathing Child with Low FIO2 Requirement and Who Cannot Tolerate an Oxygen Mask
- Particularly for Conditions Such as Croup, Bronchiolitis, Bronchospasm, etc
Technique
- Blow By Utilized Oxygen Tubing, Corrugated Plastic Tubing, etc Held a Short Distance from the Child’s Face
Range of Oxygen Delivery
- Range: <30% FIO2
- In General, Blow By is a Less Reliable Means of Oxygen Delivery
Oxygen Hood
Technique
- Oxygen Hood is a Clear Plastic Cylinder Which Encloses the Patient’s Head
- Oxygen Hoods are Used Predominantly in Infants/Children
- Hood Systems Provide Temperature and Humidification Control
- Exhaled Gas Escapes Via the Opening at the Neck
Range of Oxygen Delivery
- Range: 30-90% FIO2
Considerations
- Noisy
Oxygen Tent
Technique
- Oxygen Tent is a Clear Plastic Shell Which Encloses the Head and Upper Body
- Oxygen Tents are Used Predominantly in Infants/Children
- Tent Systems Provide Temperature and Humidification Control
Range of Oxygen Delivery
- Range: 25-50% FIO2
Considerations
- Noisy
- Mist within the Tent (Due to Humidification) May Obscure View of the Patient: which obviously may be problematic with regard to patient monitoring
- Allows Only Limited Access to the Patient
Oxygen-Conservation Devices
Indications
- Oxygen Delivery and Conservation for an Ambulatory Patient
Types of Oxygen-Conservation Systems
- Demand Pulse System
- Principle: using a flow sensor, these devices deliver a metered dose of oxygen during the earliest part of each inspiration (during the first 0.5 sec), when it can maximize gas exchange
- Systems: Chad-Oxymatic, Devilbiss-PD-1000, Helios, Invacare-Venture, Nellcor PB-CR50, Respironics e-POD, EasyPulse, Bonsai, Sage, Evolution, Evolution Motion, Impulse
- Disadvantages
- Audible Pulse Noise
- Potential for Device Failure: rare
- Reservoir Cannulas
- Principle: storage of oxygen in a reservoir during expiration (oxygen is available as a bolus during the next inspiration)
- Efficiency: reservoir nasal cannula is approximately 2-4 fold as efficient as continuous flow delivery via a nasal cannula (for example: oxygen supplied at 0.5 L/min via a reservoir cannula is equivalent to 2 L/min via a continuous flow nasal cannula)
- Systems
- Fluidic Reservoir Cannula: uses a “mustache” reservoir to function as both an oxygen-conserving and high-flow device (at 1-16 L/min)
- Oxymizer: uses a “mustache” oxygen reservoir which is located below the nose
- Oxymizer Pendant: uses an oxygen reservoir which is located on the anterior chest
- Clinical Utility: while reservoir systems can be used to decrease the flow rate in a patient on low-flow oxygen therapy, they are more commonly used to provide a higher oxygen concentrations to a patients who requires a flow rate of ≥4 L/min
- Transtracheal Oxygen Catheter
- Principle: cannula inserted into the trachea via a skin incision in the neck (bypassing the dead space of the upper airway)
- Efficiency: transtracheal catheter is approximately 2-3 fold more efficient than continuous flow delivery via a nasal cannula (this increases to 7-fold increase when using a demand pulse system with the transtracheal catheter)
- Advantages
- Decreased Dead Space: oxygen enters the trachea directly
- Decreased Total Inspired Minute Ventilation: flow from catheter allows less gas inspiration via the mouth, resulting in a decreased work of breathing
- Ensured Delivery of Oxygen
- Increased Carbon Dioxide Elimination Efficiency: therefore, despite decreased total inspiratory minute ventilation, pCO2 remains unchanged
- Oxygen Flow from the Catheter Flushes the Airways Proximal to the Catheter Tip During Expiration, Decreasing the Amount of Carbon Dioxide Which Returns to the Alveoli During the Next Inspiration
- Oxygen Flow from the Catheter Generates Turbulent Flow in the Airway, Facilitating Gas Mixing Distal to the Catheter Tip and Increasing Carbon Dioxide Washout
- Disadvantages
- Invasive (Requires Surgical Placement of a Transtracheal Catheter)
- Clinical Utility: may be used in a patient with refractory hypoxemia (similar to reservoir cannula systems)
Self-Inflating Ventilation Bag (Ambu Bag)
Technique
- Bag Has a Recoil Mechanism, Allowing Self-Inflation
- Does not require an oxygen flow to reinflate
- Ambu Bag Has a One-Way Valve to Prevent Rebreathing: however, with a tight mask seal, some spontaneously breathing patients may be able to generate adequate inspiratory pressure to overcome the one-way valve
- Oxygen Flows to the Patient When the Bag is Squeezed
Range of Oxygen Delivery
- Range: 95-100% FIO2 (with reservoir)
Considerations
- Allows Assisted Ventilation in Combination with Supplemental Oxygen: assisted ventilation is useful for patient who may be hypoxemic in combination with hypercapnic (i.e. in type II hypoxemic, hypercapnic respiratory failure)
- Should Not Use to Provide Blow By
- Requires a Reservoir to Achieve Higher FIO2
Flow-Inflating Ventilation Bag (Anesthesia Bag)
Technique
- Flow-Inflating Bag Provides a Constant Flow of Oxygen (When Connected to an Oxygen Source): bag requires a constant oxygen flow to remain inflated
Range of Oxygen Delivery
- Range: up to 100% FIO2
Considerations
- Allows Assisted Ventilation in Combination with Supplemental Oxygen
- Assisted ventilation is useful for patient who may be hypoxemic in combination with hypercapnic (i.e. in type II hypoxemic, hypercapnic respiratory failure)
- May Use to Provide Blow By
- Requires Expertise to Use Effectively (Pediatr Emerg Care, 1997) [MEDLINE]
Noninvasive Positive-Pressure Ventilation (NIPPV) (see Noninvasive Positive-Pressure Ventilation)
Range of Oxygen Delivery
- Range: 21%-100% FIO2
Considerations
- Appropriate Patient Selection is Critical, with the Following Patient Groups Having the Most Comprehensive Data in the Literature Demonstrating Clinical Benefit with the Use of NIPPV
- Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (see Chronic Obstructive Pulmonary Disease)
- Congestive Heart Failure (CHF) Exacerbation (see Congestive Heart Failure)
Mechanical Ventilation (see Mechanical Ventilation-General)
Range of Oxygen Delivery
- Range: 21%-100% FIO2
Considerations
- Allows Assisted Ventilation in Combination with Supplemental Oxygen: assisted ventilation is useful for patient who may be hypoxemic in combination with hypercapnic (i.e. in type II hypoxemic, hypercapnic respiratory failure)
Adverse Effects/Complications
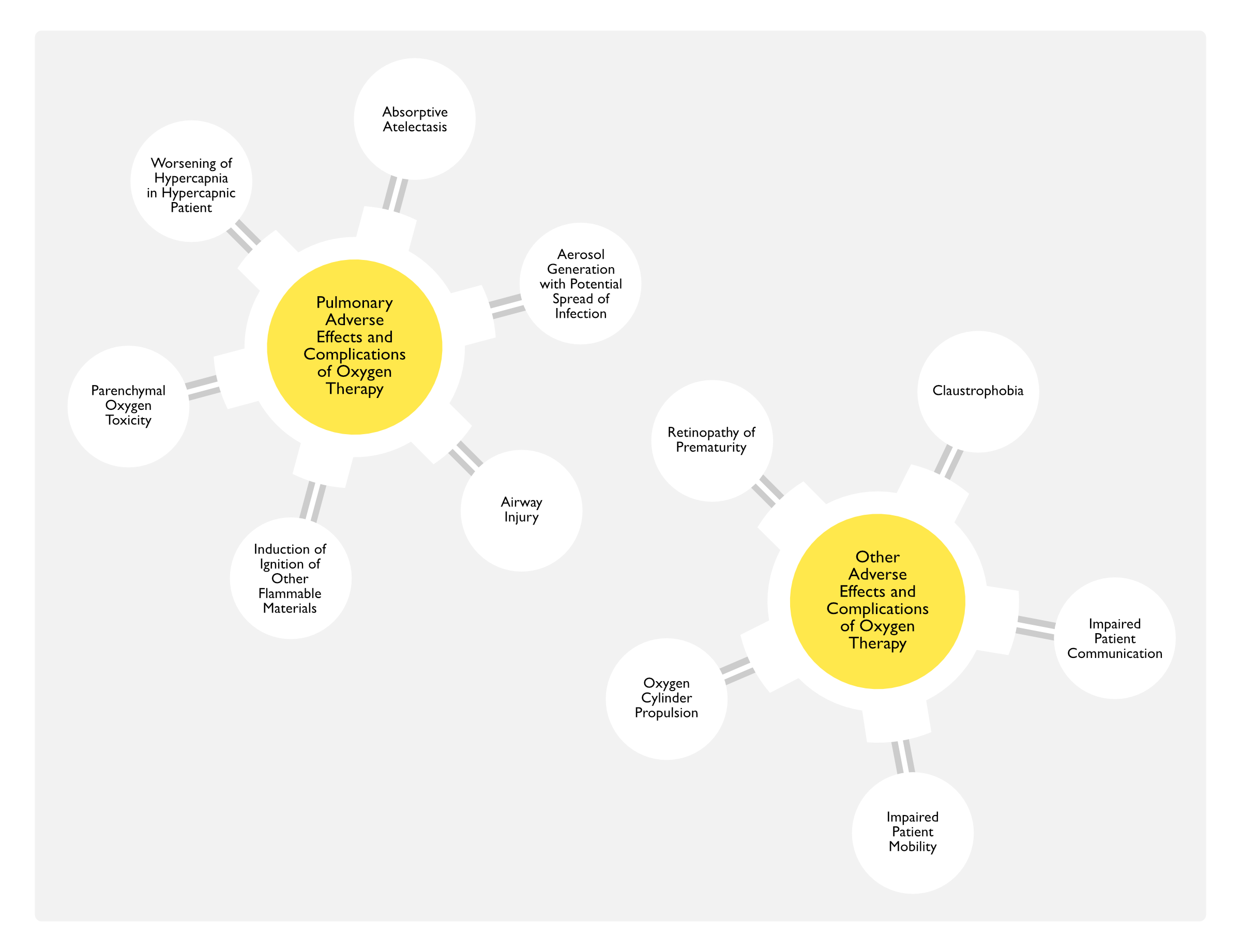
Pulmonary Adverse Effects/Complications
Absorptive Atelectasis (see Atelectasis)
- Physiology
- High FIO2 Causes a Washout of Alveolar Nitrogen and Replacement by Oxygen, Resulting in Absorption of Alveolar Oxygen into the Blood
- End Result is a Small Alveolus Which is Predisposed to Collapse (i.e. Atelectasis)
- Inhalation of 100% Oxygen for Only 5 min During Anesthesia Has Been Demonstrated to Induce Atelectasis (Anesthesiology, 2003) [MEDLINE]
- Risk Factors for Alveolar Collapse (Atelectasis) in this Setting
- High Metabolic Demand with an Increased Rate of Oxygen Uptake
- Low Regional V/Q Ratio: due to low ventilation to the region, oxygen diffuses from the alveolus into the capillary faster than it is replenished by inhaled oxygen
- Surfactant Abnormalities: such abnormalities predispose the alveolus to collapse (and further decrease the regional V/Q ratio)
- Ventilation at Low Tidal Volumes (or with Low PEEP): these factors predispose to alveolar collapse
- High FIO2 Causes a Washout of Alveolar Nitrogen and Replacement by Oxygen, Resulting in Absorption of Alveolar Oxygen into the Blood
- Clinical Consequences of Absorptive Atelectasis
- Decreased Vital Capacity
- Worsened Hypoxemia with Intrapulmonary Shunt
- On 100% FIO2, Shunt is Usually Absent in Younger Patients, But May Occur in Older Patients (Shunt May Be as High as 11% in Older Patients) (J Clin Invest, 1974) [MEDLINE]
- Once Absorptive Atelectasis Occurs, it is Not Readily Reversible by a Decrease in FIO2 (Am J Respir Crit Care Med, 2000) [MEDLINE]: this demonstrates the importance of rapid down-titration of the FIO2 as soon as possible
Aerosol Generation with Potential Spread of Infection (SARS-CoV-2, etc)
- Epidemiology
- Small Study of Aerosol Generation in 10 Normal Subjects with Various Oxygen Delivery Methods (Non-Humidified Nasal Cannula, Face Mask, Heated and Humidified High-Flow Nasal Cannula, and Noninvasive Positive-Pressure Ventilation) (Am J Respir Crit Care Med, 2020) [MEDLINE]
- Measured in a Negative Pressure Room, Oxygen Delivery Via Humidified High-Flow Nasal Cannula and Noninvasive Positive-Pressure Ventilation Did Not Increase Aerosol Generation from the Respiratory Tract in Healthy Humans with No Active Pulmonary Disease
- Small Study of Aerosol Generation in 10 Normal Subjects with Various Oxygen Delivery Methods (Non-Humidified Nasal Cannula, Face Mask, Heated and Humidified High-Flow Nasal Cannula, and Noninvasive Positive-Pressure Ventilation) (Am J Respir Crit Care Med, 2020) [MEDLINE]
Airway Injury
- Physiology
- Concentration of Reactive Oxygen Intermediates In Exhaled Gas Increases After Only 1 hr of Breathing 28% FIO2, Regardless of the Presence of Lung Disease (Thorax, 2004) [MEDLINE]
- Erythema/Edema of Large Airways (Due to Hyperoxia Bronchitis) is Bronchoscopically Observed in Patients Treated with 90% FIO2 for 6 hrs (Ann Intern Med, 1975) [MEDLINE]
- Volunteer Studies Breathing FIO2 100% x 6-48 hrs Variably Induced Tracheobronchitis, Substernal Burning, Chest Tightness, and a Dry Cough
- Pulmonary Function Tests (PFT’s) (see Pulmonary Function Tests)
- Decreased VC
- Decreased DLCO
- Pulmonary Function Tests (PFT’s) (see Pulmonary Function Tests)
- Clinical
- Dry Cough (see Cough)
- Tracheobronchitis (see Acute Bronchitis)
Induction of Ignition of Other Flammable Materials in the Presence of Open Flame, Heat Source, or Electrical Device
- Epidemiology
- Facial Hair and the Use of Hair Products Containing Oils/Alcohols are a Risk Factor for Combustion (Mayo Clin Proc, 2014) [MEDLINE]
- Safety of Electronic Cigarettes with Oxygen Therapy is Unclear
- May Occur During Surgical Airway Procedures Using Sources of Ignition (Laser, etc)
- Physiology
- Oxygen Itself is Not Flammable, But it Induces Other Materials to Catch Fire at Lower Temperatures and to Burn with a Hotter Flame
- Prevention
- Avoidance of Smoking
- Supplemental Oxygen Should Not Be Used within 5 Feet of an Open Flame, Heat Source, or Electrical Device
- Clinical
- Facial/Upper Airway Burns
Parenchymal Oxygen Toxicity
- Epidemiology
- Physiology
- Mechanisms by Which Hyperoxia Contributes to the Development of Lung Injury
- Absorptive Atelectasis: as described above
- Formation of Reactive Oxygen Intermediates (Such as Superoxide Anion, Hydroxyl Radical, and Hydrogen Peroxide) Which Overwhelm the Cell’s Antioxidant Defense Mechanisms
- Concentration of Reactive Oxygen Intermediates In Exhaled Gas Increases After Only 1 hr of Breathing 28% FIO2, Regardless of the Presence of Lung Disease (Thorax, 2004) [MEDLINE]
- Reactive Oxygen Intermediates React with Various Intracellular Macromolecules (Impairing Their Function), Resulting in Cell Death
- Impairment of Bactericidal Function of Immune Cells, Resulting in an Increased Risk of Infection
- Impairment of Mucociliary Clearance, Resulting in an Increased Risk of Infection
- Increased Susceptibility to Mucous Plugging
- Induction of a Deleterious Inflammatory Response, Resulting in Secondary Apoptosis and Tissue Damage
- Volunteer Studies Breathing FIO2 100% x 6-48 hrs Variably Induced Tracheobronchitis, Substernal Burning, Chest Tightness, and a Dry Cough
- Pulmonary Function Tests (PFT’s) (see Pulmonary Function Tests)
- Decreased VC
- Decreased DLCO
- Pulmonary Function Tests (PFT’s) (see Pulmonary Function Tests)
- Tolerance of Hyperoxia Appears to Be Related to an Ability to Generate Antioxidants: this tolerance may be genetically determined
- Phases of Oxygen Toxicity (Phases Overlap)
- Acute/Exudative Phase: usually begins within 48-72 hrs, depending on inspired oxygen fraction (and is believed to be reversible)
- Perivascular, Interstitial, and Alveolar Edema -> atelectasis and alveolar hemorrhage
- Subacute/Proliferative Phase: usually begins after 4th-7th day (and is believed to be irreversible)
- Rebsorption of Exudates
- Hyperplasia of Type II Pneumocytes
- Deposition of Collagen and Elastin in Interstitium and Hyaline Membrane Deposition
- Acute/Exudative Phase: usually begins within 48-72 hrs, depending on inspired oxygen fraction (and is believed to be reversible)
- Mechanisms by Which Hyperoxia Contributes to the Development of Lung Injury
- Clinical
- Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome)
- Treatment
- Preventive Measures: maintain pO2 <80 mmHg and FIO2 <40-50%
Worsening of Hypercapnia in Hypercapnic Patient (see Chronic Obstructive Pulmonary Disease)
- Epidemiology
- High-Flow Oxygen Administered in Chronic Obstructive Pulmonary Disease Patients (in the Pre-Hospital Setting) Has Been Demonstrated to Worsen Hypercapnia (BMJ, 2010) [MEDLINE]
- Supplemental Oxygen Therapy Can Worsen Hypercapnia in Patients with Neuromuscular Disease with Chronic Hypercapnia (Mayo Clin Proc, 1995) [MEDLINE]
- Physiology
- Patients with Chronic Hypercapnia Have a Limited Ability to Increase Their Alveolar Ventilation
- Mechanisms
- Anxiolytic/Anti-Dyspneic Effects of Supplemental Oxygen Promotes Sleep (Particularly in Patients Who are Sleep-Deprived from Respiratory Failure), Resulting in a Sleep-Related Decrease in Respiratory Drive
- Hyperoxia (Acting Via Peripheral Chemoreceptors) Modestly Blunts the Hypoxic Ventilatory Drive ( (Lancet, 1977) [MEDLINE]
- Hyperoxia Causes Oxygen-Induced Bronchodilation of Poorly-Perfused Lung Units, Worsening V/Q Mismatch and Increasing Physiologic Dead Space (i.e. Wasted Ventilation)
- Haldane Effect
- Hyperoxia Increases Oxyhemoglobin
- Oxyhemoglobin Binds Carbon Dioxide Less Avidly than Deoxyhemoglobin, Resulting in Carbon Dioxide Dissociation from Hemoglobin and Increase in Blood Carbon Dioxide Levels
- Hyperoxia-Associated Hypoventilation Decreases Inspiratory Flow Demand (Decreasing Respiratory Rate/Volume), Resulting in Decreased Entrainment of Room Air Around a Face Mask/Nasal Cannula: this effectively increases the FIO2 (even if the flow rate of the supplemental oxygen remains unchanged) further enhancing the effects of supplemental oxygen via the above mechanisms (Lancet, 2001) [MEDLINE]
Other Adverse Effects/Complications
Claustrophobia (see Claustrophobia)
- Epidemiology
- May Especially Occur with the Use of Face Mask Supplemental Oxygen
Impaired Patient Communication
- Epidemiology
- May Especially occur with the use of Face Mask Supplemental Oxygen
Impaired Patient Mobility
- Clinical
- May Result in Trips/Falls
Oxygen Cylinder Falling Over Resulting in Dislodgment of the Regulator and Propulsion
- Epidemiology
- Oxygen Cylinder May Become Propelled Like a Missile (Anesthesiology, 1978) [MEDLINE]
- For This Reason, Oxygen Cylinders Should Be Properly Secured to Avoid Them Falling Over
- Oxygen Cylinder May Become Propelled Like a Missile (Anesthesiology, 1978) [MEDLINE]
Retinopathy of Prematurity (Retrolental Fibroplasia)
- Epidemiology
- Occurs in Infants
References
General
- The oxygen delivery characteristics of the Hudson Oxy-one face mask. Anaesth Intensive Care. 1989;17(2):180 [MEDLINE]
- Rebreathing during oxygen treatment with face mask. The effect of oxygen flow rates on ventilation. Acta Anaesthesiol Scand. 1991;35(4):289 [MEDLINE]
- Comparison of self-inflating bags with anesthesia bags for bag-mask ventilation in the pediatric emergency department. Pediatr Emerg Care. 1997;13(5):312 [MEDLINE]
- ABC of oxygen. Acute oxygen therapy. BMJ. 1998;317(7161):798 [MEDLINE]
- Variability of inspired oxygen concentration with nasal cannulas. Thorax. 1992;47(8):609 [MEDLINE]
- AARC Clinical Practice Guideline: selection of an oxygen delivery device for neonatal and pediatric patients–2002 revision&update. Respir Care. 2002;47(6):707 [MEDLINE]
- Physiologic effects of noninvasive ventilation during acute lung injury. Am J Respir Crit Care Med. 2005 Nov 1;172(9):1112-8 [MEDLINE]
- Nasal high-flow versus Venturi mask oxygen therapy after extubation. Effects on oxygenation, comfort, and clinical outcome. Am J Respir Crit Care Med. 2014;190:282–288 [MEDLINE]
- Effect of Conservative vs Conventional Oxygen Therapy on Mortality Among Patients in an Intensive Care Unit: The Oxygen-ICU Randomized Clinical Trial. JAMA. 2016;316(15):1583 [MEDLINE]
- Ventilation-induced lung injury exists in spontaneously breathing patients with acute respiratory failure: Yes. Intensive Care Med. 2017 Jan 10. doi: 10.1007/s00134-016-4645-4 [MEDLINE]
- British Thoracic Society Emergency Oxygen Guideline Group BTS Emergency Oxygen Guideline Development Group. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax 2017;72(Suppl 1):ii1-90. 10.1136/ thoraxjnl-2016-209729 pmid:28507176 [MEDLINE]
- Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet. 2018 Apr 28;391(10131):1693-1705. doi: 10.1016/S0140-6736(18)30479-3 [MEDLINE]
- Oxygen therapy for acutely ill medical patients: a clinical practice guideline. BMJ. 2018 Oct 24;363:k4169. doi: 10.1136/bmj.k4169 [MEDLINE]
History
- The continuous inhalation of oxygen in cases of pneumonia otherwise fatal, and in other diseases. Boston Med J 1890;123:481-5
- Report of Societies. Oxygen therapy. BMJ 1920;i:150-2
Current Use of Oxygen in Clinical Practice
- Audit of oxygen use in emergency ambulances and in a hospital emergency department. Emerg Med J. 2008 Nov;25(11):773-6. doi: 10.1136/emj.2008.059287 [MEDLINE]
Physiology of Oxygen
- To cope with oxygen: a long and still tumultuous story for life. Crit Care Med. 2008;36:637–8 [MEDLINE]
Indications
Acute Coronary Syndrome (see Coronary Artery Disease)
- A randomized controlled trial of oxygen therapy in acute myocardial infarction Air Verses Oxygen In myocarDial infarction study (AVOID Study). Am Heart J. 2012 Mar;163(3):339-345.e1. doi: 10.1016/j.ahj.2011.11.011 [MEDLINE]
- Air Versus Oxygen in ST-Segment-Elevation Myocardial Infarction. Circulation. 2015 Jun 16;131(24):2143-50. doi: 10.1161/CIRCULATIONAHA.114.014494 [MEDLINE]
- Part 9: Acute Coronary Syndromes: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015 Nov 3;132(18 Suppl 2):S483-500. doi: 10.1161/CIR.0000000000000263 [MEDLINE]
- Oxygen Therapy in Suspected Acute Myocardial Infarction. N Engl J Med. 2017 Sep 28;377(13):1240-1249. doi: 10.1056/NEJMoa1706222 [MEDLINE]
- Impact of early hyperoxia on 28-day in-hospital mortality in patients with myocardial injury. PLoS One. 2018 Aug 7;13(8):e0201286. doi: 10.1371/journal.pone.0201286. eCollection 2018 [MEDLINE]
- Effects of supplemental oxygen therapy in patients with suspected acute myocardial infarction: a meta-analysis of randomised clinical trials. Heart. 2018 Oct;104(20):1691-1698. doi: 10.1136/heartjnl-2018-313089 [MEDLINE]
Air Embolism (see Air Embolism)
- Effect of nitrous oxide on the pulmonary circulation during venous air embolism. Anesth Analg. 1971;50(5):785 [MEDLINE]
- Computer simulation of microscopic cerebral air emboli absorption during cardiac surgery. Undersea Hyperb Med. 1998;25(1):43 [MEDLINE]
- Diagnosis and treatment of vascular air embolism. Anesthesiology. 2007;106(1):164 [MEDLINE]
Carboxyhemoglobinemia (see Carboxyhemoglobinemia)
- Carboxyhemoglobin half-life in carbon monoxide-poisoned patients treated with 100 % oxygen at atmospheric pressure. Chest. 2000;117:801–8 [MEDLINE]
Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
- Long-term results of continuous oxygen therapy at sea level. Chest. 1975;68(4):486 [MEDLINE]
- Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Nocturnal Oxygen Therapy Trial Group. Ann Intern Med. 1980;93(3):391 [MEDLINE]
- Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Report of the Medical Research Council Working Party. Lancet. 1981;1(8222):681 [MEDLINE]
- Psychologic effects of continuous and nocturnal oxygen therapy in hypoxemic chronic obstructive pulmonary disease. Arch Intern Med. 1983;143(10):1941 [MEDLINE]
- Evolution of physiological variables in patients with chronic obstructive pulmonary disease before and during long-term oxygen therapy. Respiration. 1991;58(3-4):126 [MEDLINE]
- Psychological status of COPD patients before and after one year of long-term oxygen therapy. Monaldi Arch Chest Dis. 1996;51(1):7 [MEDLINE]
- Long-term home care programmes may reduce hospital admissions in COPD with chronic hypercapnia. Eur Respir J. 1996;9(8):1605 [MEDLINE]
- Does long-term oxygen therapy affect quality of life in patients with chronic obstructive pulmonary disease and severe hypoxaemia? Eur Respir J. 1996;9(11):2335 [MEDLINE]
- Effect of long-term oxygen therapy on survival in patients with chronic obstructive pulmonary disease with moderate hypoxaemia. Thorax. 1997;52(8):674 [MEDLINE]
- A randomized trial of nocturnal oxygen therapy in chronic obstructive pulmonary disease patients. Eur Respir J. 1999;14(5):1002 [MEDLINE]
- Dose-response effect of oxygen on hyperinflation and exercise endurance in nonhypoxaemic COPD patients. Eur Respir J. 2001;18(1):77 [MEDLINE]
- Enhancement of exercise performance in COPD patients by hyperoxia: a call for research. Chest. 2002;122(5):1830 [MEDLINE]
- Does long-term oxygen therapy reduce hospitalisation in hypoxaemic chronic obstructive pulmonary disease? Eur Respir J. 2002;20(1):38 [MEDLINE]
- Long-term oxygen therapy improves health-related quality of life. Respir Med. 2004;98(4):285 [MEDLINE]
- Long-term oxygen therapy stops the natural decline of endurance in COPD patients with reversible hypercapnia. Respiration. 2004;71(4):342 [MEDLINE]
- Long-term oxygen treatment in chronic obstructive pulmonary disease: recommendations for future research: an NHLBI workshop report. Am J Respir Crit Care Med. 2006;174(4):373 [MEDLINE]
- Short burst oxygen therapy after activities of daily living in the home in chronic obstructive pulmonary disease. Thorax. 2007;62(8):702 [MEDLINE]
- Effect of oxygen on health quality of life in patients with chronic obstructive pulmonary disease with transient exertional hypoxemia. Am J Respir Crit Care Med. 2007;176(4):343 [MEDLINE]
- Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial. BMJ. 2010;341:c5462 [MEDLINE]
- Oxygen therapy for patients with COPD: current evidence and the long-term oxygen treatment trial. Chest. 2010;138(1):179 [MEDLINE]
- LOTT Trial. A Randomized Trial of Long-Term Oxygen for COPD with Moderate Desaturation. N Engl J Med. 2016;375(17):1617 [MEDLINE]
- Home Oxygen in Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2018;197(10):1254 [MEDLINE]
- Oxygen versus air-driven nebulisers for exacerbations of chronic obstructive pulmonary disease: a randomised controlled trial. BMC Pulm Med. 2018 Oct 3;18(1):157. doi: 10.1186/s12890-018-0720-7 [MEDLINE]
During Rapid Sequence Endotracheal Intubation (see Endotracheal Intubation and Airway Management)
- Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia 2015;70:323-9 [MEDLINE]
- Use of high-flow nasal cannula oxygen therapy to prevent desaturation during tracheal intubation of intensive care patients with mild-to-moderate hypoxemia. Crit Care Med. 2015;43:574–583 [MEDLINE]
- First Pass Success Without Hypoxemia Is Increased With the Use of Apneic Oxygenation During Rapid Sequence Intubation in the Emergency Department. Acad Emerg Med. 2016 Jun;23(6):703-10. Epub 2016 May 13 [MEDLINE]
- High-Flow Nasal Cannula Versus Bag-Valve-Mask for Preoxygenation Before Intubation in Subjects With Hypoxemic Respiratory Failure. Respir Care. 2016;61(9):1160 [MEDLINE]
- Respiratory support techniques to avoid desaturation in critically ill patients requiring endotracheal intubation: A systematic review and meta-analysis J Crit Care. 2017 Oct;41:98-106. doi: 10.1016/j.jcrc.2017.05.003 [MEDLINE]
High Altitude (see High Altitude)
- Aerospace Medical Association. Medical guidelines for airline travel, 2nd ed. Aviat Space Environ Med 2003; 74:A1–A19 [MEDLINE]
- Walking capacity and fitness to fly in patients with chronic respiratory disease. Aviat Space Environ Med 2007;78:789–792 [MEDLINE]
- Hypoxia altitude simulation test. Chest. 2008 Apr;133(4):1002-5. doi: 10.1378/chest.07-1354 [MEDLINE]
- The hypoxia altitude simulation test: an increasingly performed test for the evaluation of patients prior to air travel. Chest. 2008 Apr;133(4):839-42. doi: 10.1378/chest.08-0335 [MEDLINE]
- Flying with respiratory disease. Respiration. 2010;80(2):161-70. doi: 10.1159/000313425. Epub 2010 Apr 16 [MEDLINE]
- Air travel and chronic obstructive pulmonary disease: a new algorithm for pre-flight evaluation. Thorax. 2012 Nov;67(11):964-9. doi: 10.1136/thoraxjnl-2012-201855. Epub 2012 Jul 5 [MEDLINE]
Hypoxemia/Hypoxemic Respiratory Failure (see Hypoxemia and Respiratory Failure)
- The standard of care of patients with ARDS: ventilatory settings and rescue therapies for refractory hypoxemia. Intensive Care Med 2016;42:699-711 [MEDLINE]
- Oxygen in the ICU: too much of a good thing? JAMA 2016;316: 1553-4 [MEDLINE]
- Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in50countries.JAMA2016;315:788-800 [MEDLINE]
- Effectiveness and clinical outcomes of a two-step implementation of conservative oxygenation targets in critically ill patients: a before and after trial. Crit Care Med 2016;44:554-63 [MEDLINE]
- Effect of Conservative vs Conventional Oxygen Therapy on Mortality Among Patients in an Intensive Care Unit: The Oxygen-ICU Randomized Clinical Trial. JAMA. 2016;316(15):1583 [MEDLINE]
- Conservative versus Liberal Oxygenation Targets for Mechanically Ventilated Patients. A Pilot Multicenter Randomized Controlled Trial. Am J Respir Crit Care Med. 2016 Jan;193(1):43-51 [MEDLINE]
- Effect of Conservative vs Conventional Oxygen Therapy on Mortality Among Patients in an Intensive Care Unit: The Oxygen-ICU Randomized Clinical Trial. JAMA. 2016 Oct 18;316(15):1583-1589. doi: 10.1001/jama.2016.11993 [MEDLINE]
- British Thoracic Society Emergency Oxygen Guideline Group BTS Emergency Oxygen Guideline Development Group. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax 2017;72(Suppl 1):ii1-90. 10.1136/ thoraxjnl-2016-209729 pmid:28507176 [MEDLINE]
- Hyperoxia and hypertonic saline in patients with septic shock (HYPERS2S): a two-by-two factorial, multicentre, randomised, clinical trial. Lancet Respir Med. 2017 Mar;5(3):180-190. doi: 10.1016/S2213-2600(17)30046-2 [MEDLINE]
- Oxygen therapy for acutely ill medical patients: a clinical practice guideline. BMJ. 2018 Oct 24;363:k4169. doi: 10.1136/bmj.k4169 [MEDLINE]
- Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet. 2018 Apr 28;391(10131):1693-1705. doi: 10.1016/S0140-6736(18)30479-3 [MEDLINE]
- Emergency department hyperoxia is associated with increased mortality in mechanically ventilated patients: a cohort study. Crit Care. 2018 Jan 18;22(1):9. doi: 10.1186/s13054-017-1926-4 [MEDLINE]
- ICU-ROX Trial. Conservative Oxygen Therapy during Mechanical Ventilation in the ICU. N Engl J Med. 2020 Mar 12;382(11):989-998. doi: 10.1056/NEJMoa1903297 [MEDLINE]
- LOCO2 Trial. Liberal or Conservative Oxygen Therapy for Acute Respiratory Distress Syndrome. N Engl J Med. 2020 Mar 12;382(11):999-1008. doi: 10.1056/NEJMoa1916431 [MEDLINE]
- Ambulatory Oxygen in Fibrotic Interstitial Lung Disease: A Pilot, Randomized, Triple-Blinded, Sham-Controlled Trial. Chest 2020 Jul;158(1):234-244. doi: 10.1016/j.chest.2020.01.049 [MEDLINE]
- HOT-ICU Trial. Lower or Higher Oxygenation Targets for Acute Hypoxemic Respiratory Failure. N Engl J Med. 2021 Jan 20. doi: 10.1056/NEJMoa2032510 [MEDLINE]
- Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients With COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial. JAMA. 2021 May 4;325(17):1731-1743. doi: 10.1001/jama.2021.4682 [MEDLINE]
- Effectiveness and Harms of High-Flow Nasal Oxygen for Acute Respiratory Failure: An Evidence Report for a Clinical Guideline From the American College of Physicians. Ann Intern Med. 2021 Jul;174(7):952-966. doi: 10.7326/M20-4675 [MEDLINE]
- Appropriate Use of High-Flow Nasal Oxygen in Hospitalized Patients for Initial or Postextubation Management of Acute Respiratory Failure: A Clinical Guideline From the American College of Physicians. Ann Intern Med. 2021 Jul;174(7):977-984. doi: 10.7326/M20-7533 [MEDLINE]
- O2-ICU Trial. Effect of Low-Normal vs High-Normal Oxygenation Targets on Organ Dysfunction in Critically Ill Patients: A Randomized Clinical Trial. JAMA. 2021 Aug 31. doi: 10.1001/jama.2021.13011 [MEDLINE]
Ischemic Cerebrovascular Accident (CVA) (see Ischemic Cerebrovascular Accident)
- Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013 Mar;44(3):870-947. doi: 10.1161/STR.0b013e318284056a. Epub 2013 Jan 31 [MEDLINE]
- Effect of Routine Low-Dose Oxygen Supplementation on Death and Disability in Adults With Acute Stroke: The Stroke Oxygen Study Randomized Clinical Trial. JAMA. 2017 Sep 26;318(12):1125-1135. doi: 10.1001/jama.2017.11463 [MEDLINE]
Other Lung Diseases
- Long-term oxygen therapy in conditions other than chronic obstructive pulmonary disease. Respir Care. 2000;45(2):172 [MEDLINE]
- Ambulatory and short-burst oxygen for interstitial lung disease. Cochrane Database Syst Rev. 2016;7:CD011716 [MEDLINE]
Palliative Treatment of Dyspnea (see Dyspnea)
- Oxygen for end-of-life lung cancer care: managing dyspnea and hypoxemia. Expert Rev Respir Med. 2013;7(5):479 [MEDLINE]
Pulmonary Hypertension (see Pulmonary Hypertension)
- Use of supplemental oxygen in patients with pulmonary arterial hypertension in REVEAL. J Heart Lung Transplant. 2018 Mar 17. pii: S1053-2498(18)31395-0 [MEDLINE]
Administration
- Effect of Conservative vs Conventional Oxygen Therapy on Mortality Among Patients in an Intensive Care Unit: The Oxygen-ICU Randomized Clinical Trial. JAMA. 2016 Oct 18;316(15):1583-1589. doi: 10.1001/jama.2016.11993 [MEDLINE]
- Hyperoxia and hypertonic saline in patients with septic shock (HYPERS2S): a two-by-two factorial, multicentre, randomised, clinical trial. Lancet Respir Med. 2017 Mar;5(3):180-190. doi: 10.1016/S2213-2600(17)30046-2 [MEDLINE]
- Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet. 2018 Apr 28;391(10131):1693-1705. doi: 10.1016/S0140-6736(18)30479-3 [MEDLINE]
- Hyperoxia toxicity in septic shock patients according to the Sepsis-3 criteria: a post hoc analysis of the HYPER2S trial. Ann Intensive Care. 2018 Sep 17;8(1):90. doi: 10.1186/s13613-018-0435-1 [MEDLINE]
Oxygen Delivery Systems
High-Flow Nasal Cannula
- Research in high flow therapy: mechanisms of action. Respir Med. 2009 Oct;103(10):1400-5 [MEDLINE]
- High-flow oxygen therapy in acute respiratory failure. Respir Care. 2010;55(4):408 [MEDLINE]
- High-flow nasal oxygen vs high-flow face mask: a randomized crossover trial in extubated patients. J Crit Care. 2010 Sep;25(3):463-8 [MEDLINE]
- The effects of flow on airway pressure during nasal high-flow oxygen therapy. Respir Care. 2011;56(8):1151 [MEDLINE]
- Oxygen delivery through high-flow nasal cannulae increase end-expiratory lung volume and reduce respiratory rate in post-cardiac surgical patients. Br J Anaesth. 2011 Dec;107(6):998-1004 [MEDLINE]
- High-flow nasal cannula oxygen therapy during hypoxemic respiratory failure. Respir Care. 2012 Oct;57(10):1696-8 [MEDLINE]
- High flow nasal oxygen in acute respiratory failure. Minerva Anestesiol. 2012 Jul;78(7):836-41 [MEDLINE]
- Beneficial effects of humidified high flow nasal oxygen in critical care patients: a prospective pilot study. Intensive Care Med. 2011;37(11):1780 [MEDLINE]
- Humidified high flow nasal oxygen during respiratory failure in the emergency department: feasibility and efficacy. Respir Care. 2012;57(11):1873 [MEDLINE]
- Impact of high-flow nasal cannula oxygen therapy on intensive care unit patients with acute respiratory failure: a prospective observational study. J Crit Care. 2012;27(3):324.e9 [MEDLINE]
- High-flow oxygen administration by nasal cannula for adult and perinatal patients. Respir Care 2013;58:98-122
- Effect of high-flow nasal cannula and body position on end-expiratory lung volume: a cohort study using electrical impedance tomography. Respir Care. 2013;58(4):589 [MEDLINE]
- Pressures delivered by nasal high flow oxygen during all phases of the respiratory cycle. Respir Care. 2013;58(10):1621 [MEDLINE]
- Use of high flow nasal cannula in critically ill infants, children, and adults: a critical review of the literature. Intensive Care Med. 2013 Feb;39(2):247-57. doi: 10.1007/s00134-012-2743-5 [MEDLINE]
- High-flow oxygen administration by nasal cannula for adult and perinatal patients. Respir Care 2013;58:98-122
- High-flow nasal cannulae in very preterm infants after extubation. N Engl J Med. 2013 Oct 10;369(15):1425-33 [MEDLINE]
- High-flow nasal cannula versus conventional oxygen therapy after endotracheal extubation: a randomized crossover physiologic study. Respir Care. 2014 Apr;59(4):485-90. doi: 10.4187/respcare.02397 [MEDLINE]
- Comparison of three high flow oxygen therapy delivery devices: a clinical physiological cross-over study. Minerva Anestesiol. 2013 Dec;79(12):1344-55 [MEDLINE]
- Implementation of bronchoalveolar lavage using a high-flow nasal cannula in five cases of acute respiratory failure. Respir Investig. 2014 Sep;52(5):310-4 [MEDLINE]
- High-flow nasal cannula oxygen versus non-invasive ventilation in patients with acute hypoxaemic respiratory failure undergoing flexible bronchoscopy–a prospective randomised trial. Crit Care. 2014;18(6):712 [MEDLINE]
- Nasal high-flow versus Venturi mask oxygen therapy after extubation. Effects on oxygenation, comfort, and clinical outcome. Am J Respir Crit Care Med. 2014;190(3):282 [MEDLINE]
- FLORALI Study. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med 2015. DOI: 10.1056/NEJMoa1503326 [MEDLINE]
- High-flow nasal cannula oxygen during endotracheal intubation in hypoxemic patients: a randomized controlled clinical trial. Intensive Care Med. 2015;41(9):1538 [MEDLINE]
- Saving lives with high-flow nasal oxygen. N Engl J Med. 2015 Jun 4;372(23):2225-6. doi: 10.1056/NEJMe1504852. Epub 2015 May 17 [MEDLINE]
- Use of high-flow nasal cannula oxygen therapy to prevent desaturation during tracheal intubation of intensive care patients with mild-to-moderate hypoxemia. Crit Care Med. 2015;43:574–583 [MEDLINE]
- Heated humidified high-flow nasal oxygen in adults: mechanisms of action and clinical implications. Chest. 2015;148(1):253–261 [MEDLINE]
- Use of high-flow nasal cannula oxygen therapy in subjects with ARDS: a 1-year observational study. Respir Care. 2015;60:162–169 [MEDLINE]
- Effect of Postextubation High-Flow Nasal Cannula vs Conventional Oxygen Therapy on Reintubation in Low-Risk Patients: A Randomized Clinical Trial. JAMA. 2016;315(13):1354 [MEDLINE]
- High-flow nasal cannula oxygen therapy in adults. J Intensive Care. 2015 Mar 31;3(1):15. doi: 10.1186/s40560-015-0084-5. eCollection 2015 [MEDLINE]
- Noninvasive respiratory support for acute respiratory failure-high flow nasal cannula oxygen or non-invasive ventilation? J Thorac Dis. 2015 Jul;7(7):1092-7. doi: 10.3978/j.issn.2072-1439.2015.07.18 [MEDLINE]
- Failure of high-flow nasal cannula therapy may delay intubation and increase mortality. Intensive Care Med. 2015;41(4):623 [MEDLINE]
- Effect of Postextubation High-Flow Nasal Cannula vs Conventional Oxygen Therapy on Reintubation in Low-Risk Patients: A Randomized Clinical Trial. JAMA. 2016;315(13):1354 [MEDLINE]
- Apnoeic oxygenation via high-flow nasal cannula oxygen combined with non-invasive ventilation preoxygenation for intubation in hypoxaemic patients in the intensive care unit: the single-centre, blinded, randomised controlled OPTINIV trial. Intensive Care Med. 2016;42(12):1877 [MEDLINE]
- Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill. Am J Respir Crit Care Med. 2016;193(3):273 [MEDLINE]
- Effect of Postextubation High-Flow Nasal Cannula vs Conventional Oxygen Therapy on Reintubation in Low-Risk Patients: A Randomized Clinical Trial. JAMA. 2016;315(13):1354 [MEDLINE]
- Effect of early postextubation high-flow nasal cannula vs conventional oxygen therapy on hypoxaemia in patients after major abdominal surgery: a French multicentre randomised controlled trial (OPERA). Intensive Care Med. 2016;42(12):1888 [MEDLINE]
- Effect of Postextubation High-Flow Nasal Cannula vs Conventional Oxygen Therapy on Reintubation in Low-Risk Patients: A Randomized Clinical Trial. JAMA. 2016;315(13):1354 [MEDLINE]
- Optimum support by high-flow nasal cannula in acute hypoxemic respiratory failure: effects of increasing flow rates. Intensive Care Med. 2017;43(10):1453 [MEDLINE]
- The Effect of High-Flow Nasal Cannula Oxygen Therapy on Mortality and Intubation Rate in Acute Respiratory Failure: A Systematic Review and Meta-Analysis. Crit Care Med. 2017;45(4):e449 [MEDLINE]
- Physiologic Effects of High-Flow Nasal Cannula in Acute Hypoxemic Respiratory Failure. Am J Respir Crit Care Med. 2017;195(9):1207 [MEDLINE]
- High-flow oxygen via tracheostomy improves oxygenation in patients weaning from mechanical ventilation: a randomised crossover study. Intensive Care Med. 2017;43(3):465 [MEDLINE]
- Can High-flow Nasal Cannula Reduce the Rate of Endotracheal Intubation in Adult Patients With Acute Respiratory Failure Compared With Conventional Oxygen Therapy and Noninvasive Positive Pressure Ventilation?: A Systematic Review and Meta-analysis. Chest. 2017;151(4):764 [MEDLINE]
- Effect of high-flow nasal cannula oxygen therapy in adults with acute hypoxemic respiratory failure: a meta-analysis of randomized controlled trials. CMAJ. 2017;189(7):E260 [MEDLINE]
Transtracheal Oxygen
- A program for transtracheal oxygen delivery. Assessment of safety and efficacy. Ann Intern Med. 1987;107(6):802 [MEDLINE]
- Transtracheal oxygen: a step beyond the nasal cannula for long-term oxygen therapy. Nebr Med J. 1992;77(11):29 [MEDLINE]
Adverse Effects/Complications
- The effect of inhalation of high concentrations of oxygen for 24 hours on normal men at sea level and at a simulated altitude of 18,000. JAMA. 1945; 128:710
- The J. Burns Amberson Lecture. The management of acute respiratory failure in chronic bronchitis and emphysema. Am Rev Respir Dis. 1967;96(4):626 [MEDLINE]
- Causes of pulmonary oxygen toxicity. N Engl J Med. 1970;283(27):1518 [MEDLINE]
- Oxygen toxicity in man. A prospective study in patients after open-heart surgery. N Engl J Med. 1970;283(27):1473 [MEDLINE]
- Continuous distributions of ventilation-perfusion ratios in normal subjects breathing air and 100 per cent O2. J Clin Invest. 1974;54(1):54 [MEDLINE]
- Pulmonary effects of oxygen breathing. A 6-hour study in normal men. Ann Intern Med. 1975;82(1):40 [MEDLINE]
- Hypercapnia during oxygen therapy in acute exacerbations of chronic respiratory failure. Hypothesis revisited. Lancet. 1977;2(8036):483 [MEDLINE]
- Potential hazards of compressed gas cylinders: a review. Anesthesiology. 1978 Jan;48(1):72-4 [MEDLINE]
- Controlled oxygen administration in acute respiratory failure in chronic obstructive pulmonary disease: a reappraisal. Am J Med. 1978;65(6):896 [MEDLINE]
- Normobaric oxygen toxicity of the lung. N Engl J Med. 1980;303(2):76 [MEDLINE]
- Pulmonary oxygen toxicity. Early reversible changes in human alveolar structures induced by hyperoxia. N Engl J Med. 1983;309(15):878 [MEDLINE]
- Protective effect of hypoxia on bleomycin lung toxicity in the rat. Am Rev Respir Dis. 1984;130(2):307 [MEDLINE]
- Pulmonary oxygen toxicity. Chest. 1985;88(6):900 [MEDLINE]
- Prediction of pulmonary function abnormalities after adult respiratory distress syndrome (ARDS). Am Rev Respir Dis. 1987;135(3):634 [MEDLINE]
- Oxygen toxicity. New Horiz. 1993;1(4):504 [MEDLINE]
- Severe hypercapnia after low-flow oxygen therapy in patients with neuromuscular disease and diaphragmatic dysfunction. Mayo Clin Proc. 1995;70(4):327 [MEDLINE]
- Hyperoxia and lung disease. Curr Opin Pulm Med. 1998;4(5):300 [MEDLINE]
- Pulmonary gas exchange response to oxygen breathing in acute lung injury. Am J Respir Crit Care Med. 2000;161(1):26 [MEDLINE]
- The role of hypoventilation and ventilation-perfusion redistribution in oxygen-induced hypercapnia during acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1524 [MEDLINE]
- Optimal oxygen concentration during induction of general anesthesia. Anesthesiology. 2003 Jan;98(1):28-33 [MEDLINE]
- Treatment of oxygen-induced hypercapnia. Lancet. 2001;357(9259):884 [MEDLINE]
- Supplementary oxygen in healthy subjects and those with COPD increases oxidative stress and airway inflammation. Thorax. 2004;59(12):1016 [MEDLINE]
- Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932 [MEDLINE]
- Initial oxygen management in patients with an exacerbation of chronic obstructive pulmonary disease. QJM. 2005;98(7):499 [MEDLINE]
- The effects of oxygen therapy in patients presenting to an emergency department with exacerbation of chronic obstructive pulmonary disease. Med J Aust. 2007;186(5):235 [MEDLINE]
- Facial hair: a newly identified, modifiable risk factor in home oxygen therapy-related burns. Mayo Clin Proc. 2014;89(8):1164 [MEDLINE]
- Normobaric hyperoxia alters the microcirculation in healthy volunteers. Microvasc Res. 2015 Mar;98:23-8. doi: 10.1016/j.mvr.2014.11.006 [MEDLINE]
- Hyperoxia in intensive care, emergency, and peri-operative medicine: Dr. Jekyll or Mr. Hyde? A 2015 update. Ann Intensive Care 2015;5:42. 10.1186/s13613-015- 0084-6 pmid:26585328 [MEDLINE]
- Effect of High-Flow Nasal Oxygen vs Standard Oxygen on 28-Day Mortality in Immunocompromised Patients With Acute Respiratory Failure: The HIGH Randomized Clinical Trial. JAMA. 2018 Oct 24. doi: 10.1001/jama.2018.14282 [MEDLINE]
- Aerosol Generation from the Respiratory Tract with Various Modes of Oxygen Delivery. Am J Respir Crit Care Med 2020 Aug 21. doi: 10.1164/rccm.202006-2309OC [MEDLINE]