Persistent Vegetative State: term was first used in 1972
Minimally Conscious State
Considerations
The Criteria for the Determination of Brain death Given in the 1995 AAN Neurology Practice Parameter Have Not Been Invalidated by Published Reports of Neurologic Recovery in Patients Who Fulfill These Criteria (Level U Recommendation)
There is Insufficient Evidence to Determine the Minimally Acceptable Observation Period to Ensure that Neurologic Functions Have Irreversibly Ceased (Level U Recommendation)
Complex Spontaneous Motor Movements and Fase-Positive Triggering of the Ventilator May Occur in Patients Who are Brain Dead (Level C Recommendation)
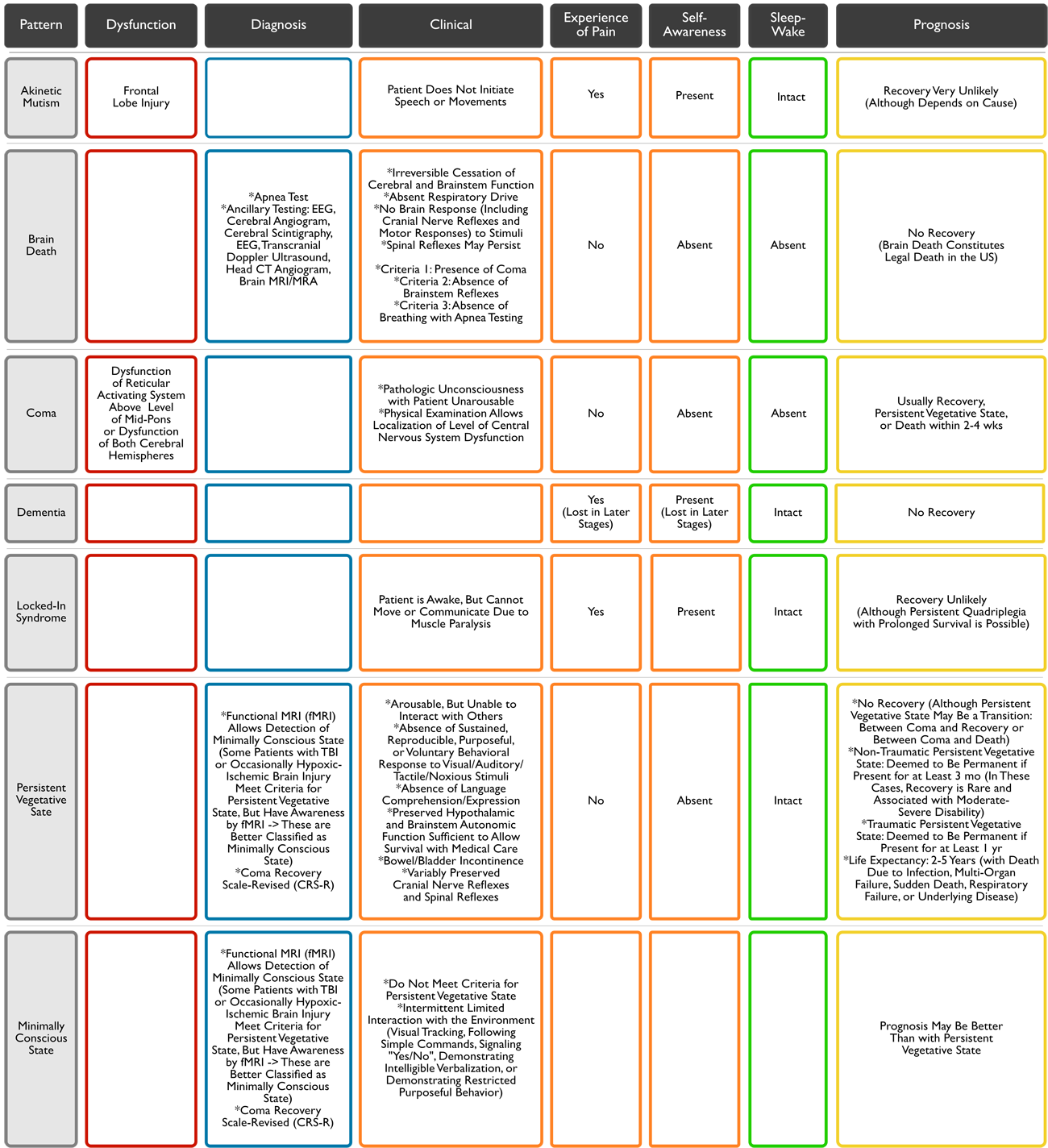
Criteria 1: Presence of Coma
Patients Must Lack All Evidence of Responsiveness
Eye opening or eye movement to Noxious Stimuli is Absent
Noxious Stimuli Should Not Produce a Motor Response Other than Spinally-Mediated Reflexes
The Clinical Differentiation of Spinal Responses from Retained Motor Responses Associated with Brain Activity Requires Expertise
Criteria 2: Absence of Brainstem Reflexes
Absence of Pupillary Response to Bright Light in Both Eyes
Usually the Pupils are Fixed in a Midsize or Dilated Position (4–9 mm)
Constricted Pupils Suggest the Possibility of Drug Intoxication
When Uncertainty Exists, a Magnifying Glass Should be Used
Absence of Ocular Movements with Oculocephalic Reflex Testing and Oculovestibular Reflex Testing
Technique of Oculocephalic Reflex Testing: once the integrity of the cervical spine is ensured, the head is briskly rotated horizontally and vertically
There Should Be no Movement of the Eyes Relative to Head Movement
Technique of Oculovestibular Testing: irrigate each ear with ice water (caloric testing) after the patency of the external auditory canal is confirmed
The Head is Elevated to 30 Degrees
Each External Auditory Canal is Irrigated (1 Ear at a Time) with Approximately 50 mL of Ice Water
Movement of the Eyes Should be Absent During 1 min of Observation
Both Sides are Tested, with an Interval of Several Minutes
Absence of Corneal Reflex
Technique of Corneal Reflex Testing: touching the cornea with a piece of tissue paper, a cotton swab, or squirts of water
No Eyelid Movement Should Be Seen
Absence of Facial Muscle Movement to Noxious Stimuli
Technique: deep pressure on the condyles at the level of the temporomandibular joints and deep pressure at the supraorbital ridge
No Grimacing or Facial Muscle Movement Should Be Seen
Absence of Pharyngeal and Tracheal Reflexes
Technique of Pharyngeal/Gag Reflex Testing: stimulation of the posterior pharynx with a tongue blade or suction device
Technique of Tracheal Reflex Testing: most reliably tested by examining the cough response to tracheal suctioning -> the catheter should be inserted into the trachea and advanced to the level of the carina followed by 1 or 2 suctioning passes
Criteria 3: Absence of Breathing with Apnea Test
Considerations
There is Insufficient Evidence to Determine the Comparative Safety of Techniques Used for Apnea Testing (Level U Recommendation)
Prerequisites
Normothermia: core temperature at least 36.5 C (97 F)
Normotension: SBP >90 mm Hg (with or without pressors)
Eucapnia: normal PCO2 (arterial PCO2 of 35-45 mm Hg) and no prior evidence of CO2 retention
Procedure
Adjust Pressors to Achieve SBP >100 mm Hg
Preoxygenate >10 min with 100% O2 to Achieve pO2 >200 mm Hg
Adjust Ventilator RR to Achieve Eucapnia (pCO2: 35-45)
Reduce PEEP to +5 cm H2O (oxygen desaturation with decreasing PEEP may predict difficulty with performing the apnea test)
If SpO2 Remains >95%, Obtain Baseline ABG
Disconnect Patient from Ventilator -> Place a Cut-Off Nasal Cannula Catheter (at 6 L/min) Through the ETT and Close to the Level of the Carina
Monitor for 10 min -> Look Closely for Respiratory Movements
Respiration is Defined as Abdominal or Chest Excursions and May Include a Brief Gasp
Abort (and Check ABG) if Systolic Blood Pressure Decreases to <90 mm Hg
Abort (and Check ABG) if SpO2 Decreases to <85% for at Least 30 sec
If Apnea Test is Aborted for Hypoxemia, May Retry Procedure with T-Piece, CPAP 10 cm H2O, and 100% Oxygen at 12 L/min
If No Respiratory Movements are Observed, Repeat ABG at 10 min and Reconnect Patient to Ventilator
Interpretation of Apnea Test
Positive Apnea Test (i.e., supports the clinical diagnosis of brain death)
No Respiratory Movements are Observed
Arterial PCO2 >60 mm Hg (or >20 mm Hg Increase in PCO2 Over Baseline Normal Arterial PCO2)
Inconclusive Apnea Test
No Respiratory Movements are Observed
Arterial PCO2 is <60 mm Hg (or <20 mm Hg Increase in PCO2 Over Baseline Normal Arterial PCO2)
If Apnea Test is Inconclusive: if the patient is hemodynamically stable during the testing, it may be repeated for a longer period of time (10-15 min) after the patient is again adequately preoxygenated
Ancillary Testing
Considerations
There is Insufficient Evidence to Determine if Newer Ancillary Tests Accurately Confirm the Cessation of Function of the Entire Brain (Level U Recommendation
Rationale
Ancillary Tests are Used When There is Uncertainty About Reliability of Components of the Neurologic Exam or When the Apnea Test Cannot Be Performed
They are Not Required for the Diagnosis of Brain Death in Adults
They Should Not Replace a Neurologic Exam
Ancillary Tests May Be Used to Shorten the Duration of the Observation Period (in Some Protocols)
Interpretation of Ancillary Tests Requires Expertise: results should be correlated with those from neurologic exam (as false-positives may occur in ancillary testing)
Rather Than Ordering Ancillary Testing, Physicians May Decide to Not Proceed with the Declaration of Brain Death if Clinical Findings are Unreliable