Alcohol (Ethanol) Abuse (see Ethanol): 5% of cases
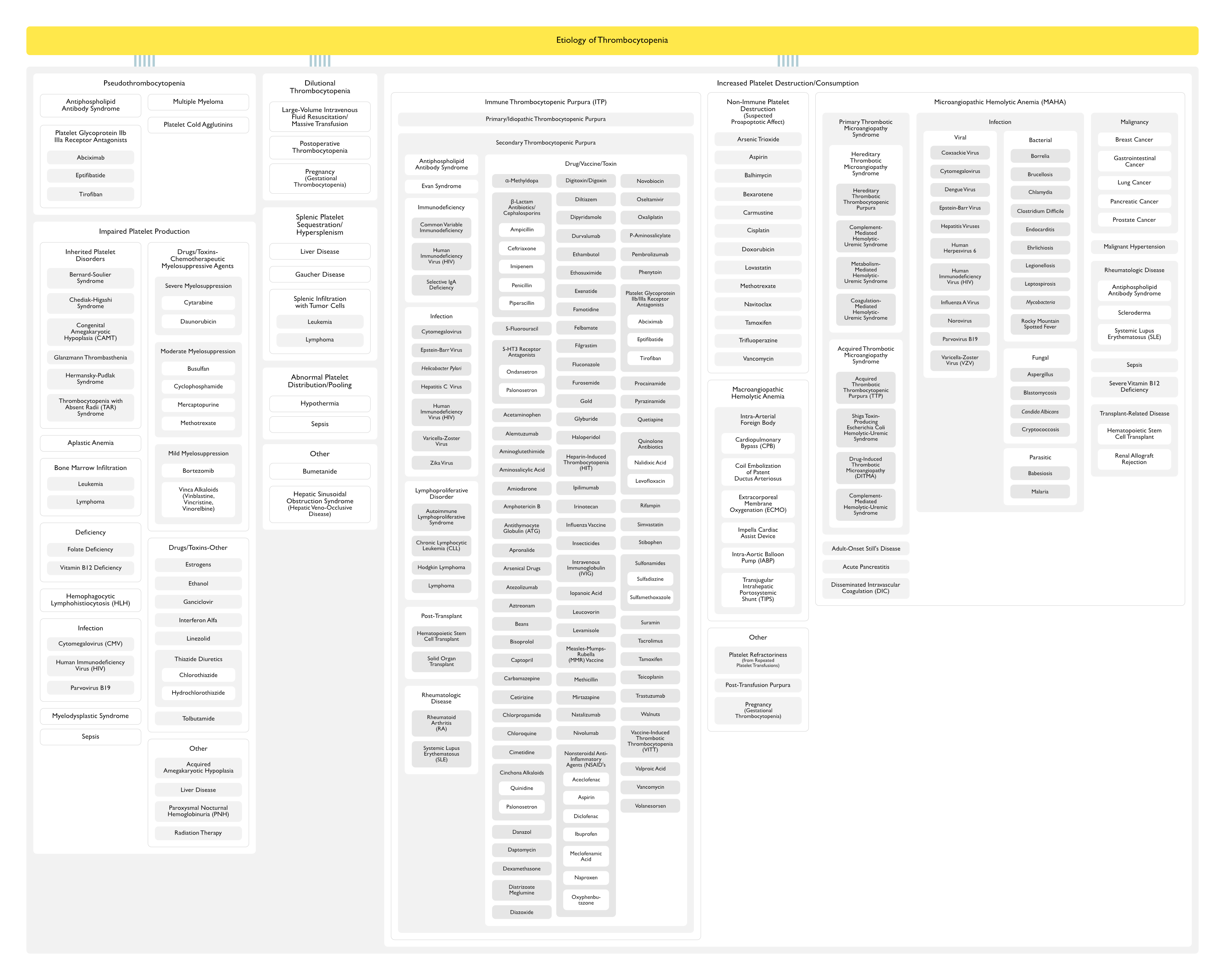
Etiology
Pseudothrombocytopenia
General Comments
In Vitro Artifact Due to Platelet Agglutination Via Antibodies (Usually, IgG, Also IgM and IgA) When the Calcium Content is Decreased by Blood Collection in Purple Top EDTA-Containing Blood Collection Tubes
If Suspected, Platelet Count Should Be Determined Using a Blue Top Sodium Citrate-Containing Tube, a Green Top Heparin-Containing Tube, or Via a Peripheral Smear of Fingerstick Blood
Incidence of Pseudothrombocytopenia with Abciximab was 1.1%, Whereas the Incidence of True Acute Thrombocytopenia was 2.7% with Abciximab (see Abciximab)
Collect Blood in Citrate Tubes
May Allow Accurate Counting in Some, But Not All, Cases of EDTA-Associated Clumping
Inherited platelet disorders can affect platelet number, platelet function, or both
These include syndromic disorders with other manifestations as well as disorders with isolated thrombocytopenia
Although these are lifelong disorders, they often are not diagnosed until adulthood, or they may be misdiagnosed as immune thrombocytopenia (ITP)
This was Illustrated in a Database Review from the McMaster Immune Thrombocytopenic Purpura Registry, Which Found That, of 295 Patients Initially Diagnosed with Primary Immune Thrombocytopenic Purpura, 5 Patients were Reclassified as Having an Inherited Platelet Disorder
Rare Disorder Which Presents with Severe Thrombocytopenia and Absence of Megakaryocytes in the Bone Marrow
Some Patients are Homozygous for Mutations Which Produce an Inactive Thrombopoietin Receptor (c-Mpl) Leading to Minimal Platelet Production Similar to that Observed in c-Mpl Knockout Mice
Some Patients Ultimately Develop Bone Marrow Aplasia, Confirming the Multipotential Effect of Thrombopoietin Activity
Bone Marrow Suppression (Often Accompanied by Other Cytopenias)
Consumptive Coagulopathy Related to Sepsis-Induced Platelet Activation with/without Frank Disseminated Intravascular Coagulation (DIC) (see Disseminated Intravascular Coagulation)
Hemodilution Associated with Intravenous Fluid Resuscitation
Liver Produces Thrombopoietin, and Severe Liver Disease with Impaired Liver Synthetic Function (and Decreased Thrombopoietin Levels) Can Result in Thrombocytopenia
Note that Liver Disease Also Causes Compensatory Splenomegaly with Hypersplenism (Splenic Sequestration of Platelets) (See Below)
Splenic Platelet Sequestration/Hypersplenism (see Splenomegaly)
General Comments
Approximately one-third of the platelet mass is found in the spleen, in equilibrium with the circulating platelet pool (J Clin Invest, 1966) [MEDLINE])
With splenomegaly, a greater fraction of the total platelet mass is sequestered in the spleen (up to 90 percent of the total platelet mass), resulting in a decreased circulating platelet count
Thrombocytopenia from splenic pooling of platelets is typically mild to moderate (in the range of 60-100,000/μL)
Severe thrombocytopenia or bleeding in the setting of splenomegaly should prompt investigation for other causes
In a series of 354 patients with a presumptive diagnosis of nonalcoholic fatty liver disease, thrombocytopenia was seen in 29% (Clin Gastroenterol Hepatol, 2012) [MEDLINE]
Physiology
Portal Hypertension Results in Splenomegaly
In severe liver disease, platelets may also be decreased because of reduced thrombopoietin levels
Massive fluid resuscitation or massive transfusion without proportionate transfusion of platelets can cause thrombocytopenia
In massive transfusion, platelet counts are reduced in proportion to the number of red blood cell (RBC) units transfused in a 24-hour period (Ann Surg, 1979) [MEDLINE] (Am J Clin Pathol, 1991) [MEDLINE]
If thrombocytopenia is mild, the patient can be observed until the platelet count recovers
If significant blood has been lost, platelet transfusions may be needed. Ratios of platelets to other products are discussed separately
Bone Marrow Suppression (Often Accompanied by Other Cytopenias)
Consumptive Coagulopathy Related to Sepsis-Induced Platelet Activation with/without Frank Disseminated Intravascular Coagulation (DIC) (see Disseminated Intravascular Coagulation)
Hemodilution Associated with Intravenous Fluid Resuscitation
Postoperative Thrombocytopenia May Occur if There is Significant Consumption of Platelets During Surgery or in Wound Healing
Dilutional thrombocytopenia may also contribute
This is generally a diagnosis of exclusion made when other causes of thrombocytopenia are absent and the platelet count gradually Normalizes
Pregnancy (Gestational Thrombocytopenia) (see Pregnancy)
Physiology
Gestational Thrombocytopenia results from progressive expansion of the blood volume that typically occurs during pregnancy, leading to Hemodilution*
Cytopenias Result, Although Production of Blood Cells is Normal or Increased
Clinical
Platelet Counts <100k, However, are Observed in <10% of Pregnant Women in the Third Trimester
Decreases in Platelet Count to <70k Should Prompt Consideration of Pregnancy-Related ITP (See Above) as Well as Preeclampsia or a Pregnancy-Related Thrombotic Microangiopathy
Bone Marrow Suppression (Often Accompanied by Other Cytopenias)
Consumptive Coagulopathy Related to Sepsis-Induced Platelet Activation with/without Frank Disseminated Intravascular Coagulation (DIC) (see Disseminated Intravascular Coagulation)
Hemodilution Associated with Intravenous Fluid Resuscitation
In the EPIC Trial, the Incidence of Pseudothrombocytopenia with Abciximab was 1.1%, Whereas the Incidence of True Acute Thrombocytopenia was 2.7% with Abciximab
Physiology
Believed to Be Due to Preformed Antibodies Against Neoepitopes Exposed by Alteration of the GP IIb/IIIa Molecules
Rare Syndrome Which Occurs Approximately 5-30 Days Following Vaccination with a Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2) Adenoviral Vector Vaccine (from AstraZeneca or Janssen)
May Manifest Life-Threatening Arterial and/or Venous Thromboses
Immunologic Destructive Mechanism, Which Occurs Via Abnormal Vessels and/or Fibrin Thrombi
Microangiopathic Hemolytic Anemia (MAHA) is Caused by mechanical Red Blood Cell Fragmentation Which Occurs as Red Blood Cells Traverse Platelet-Rich Thrombi in the Microcirculation
The Result of Red Blood Cell Fragmentation is Schistocytes, Which Typically are Prominent on the Peripheral Blood Smear
Thrombocytopenia is Due to Platelet Consumption in Microthrombi Throughout the Microcirculation
Thrombocytopenia May Be Only Mild-Moderate in Many of the Primary Thrombotic Microangiopathy Syndromes, But in Patients with Thrombotic Thrombocytopenic Purpura (TTP), it is Typically Severe (Platelet Count is Almost Always <30,000/μL
Severe Hypertension (Systolic Blood Pressure >220 mm Hg and/or Diastolic Blood Pressure >100 mm Hg) Can Cause Microangiopathic Hemolytic Anemia (MAHA) and Thrombocytopenia
Physiology
Abnormal Vessel Wall Resulting in Damage to Red Blood Cells
Bone Marrow Suppression (Often Accompanied by Other Cytopenias)
Consumptive Coagulopathy Related to Sepsis-Induced Platelet Activation with/without Frank Disseminated Intravascular Coagulation (DIC) (see Disseminated Intravascular Coagulation)
Hemodilution Associated with Intravenous Fluid Resuscitation
Vitamin B12 Deficiency Can Cause Ineffective Erythropoiesis and Thrombocytopenia, Which May Be Accompanied by Hemolysis and Red Blood Cell Morphology Resembling Microangiopathic Hemolytic Anemia (MAHA) (Pediatr Blood Cancer, 2009) [MEDLINE] (Am J Med, 2015) [MEDLINE] (CMAJ, 2023) [MEDLINE]
Retrospective Series of Patients with Vitamin B12 Deficiency (Br J Haematol, 2020) [MEDLINE]: n = 2,699
Approximately 0.6% of Cases Dad Findings Consistent with a Thrombotic Microangiopathy Including Schistocytes on the Peripheral Blood Smear, Thrombocytopenia, and/or Hemolysis with Increased Lactate Dehydrogenase (LDH)
Compared with a Matched Cohort of Patients with Thrombotic Thrombocytopenic Purpura, Those with Vitamin B12 Deficiency were More Likely to Have Teardrop Cells on the Peripheral Blood Smear, a Very High Lactate Dehydrogenase (LDH) Level, and a Lower PLASMIC Score
Microangiopathic Hemolytic Anemia (MAHA) with Thrombocytopenia May Be Associated with Calcineurin Inhibitor Administration or Cytomegalovirus (CMV) Infection (Due to Immunosuppression)
Abnormal Vessel Wall Resulting in Damage to Red Blood Cells
Clinical
Mild Thrombocytopenia
Prognosis
In Patients Who Have Received a Renal Transplant for a Primary Thrombotic Microangiopathy Syndrome, the Syndrome May Recur in the Transplanted Kidney
Other
Other
Postoperative Thrombocytopenia
Postoperative Thrombocytopenia May Occur if There is Significant Consumption of Platelets During Surgery or in Wound Healing
Dilutional Thrombocytopenia May Also Contribute
Postoperative Thrombocytopenia is Generally a Diagnosis of Exclusion Made When Other Etiologies of Thrombocytopenia are Absent and the Platelet Count Gradually Normalizes
Rare Disorder with Sudden-Onset Thrombocytopenia in Patient Who Recently Received Transfusion of Red Blood Cells, Platelets, or Plasma within 1 wk Prior to Detection of Thrombocytopenia
Antibodies Against the Human Platelet Antigen PlA1 are Detected in Most Patients
Patients with Post-Transfusion Purpura Almost Universally are Either Multiparous Women or Patients Who Have Received Transfusions Previously
Severe Thrombocytopenia and Bleeding is Typical
Initial Treatment Consists of Administration of IVIG (1 g/kg/d for 2 days)l, Which Should Be Administered as Soon as the Diagnosis is Suspected
Platelets are Not Indicated Unless Severe Bleeding is Present, But if They are Administered, HLA-Matched Platelets are Preferred
A Second Course or IVIG, Plasma Exchange, Corticosteroids, or Splenectomy May Be Used in Refractory Cases
PlA1-Negative or Washed Blood Products are Preferred for Subsequent Transfusions
Platelet Refractoriness (Due to Repeated Platelet Transfusions)
Repeat Transfusions Result in Antiplatelet Alloantibodies Resulting in Immune-Mediated Destruction of Future Transfused Platelets
Pregnancy (Gestational Thrombocytopenia) (see Pregnancy)
Physiology
Gestational Thrombocytopenia Results from Progressive Expansion of the Blood Volume that Typically Occurs During Pregnancy, Leading to Hemodilution
Cytopenias Result, Although Production of Blood Cells is Normal or Increased
Clinical
Platelet Counts <100k, However, are Observed in <10% of Pregnant Women in the Third Trimester
Decreases in Platelet Count to <70k Should Prompt Consideration of Pregnancy-Related ITP (See Above) as Well as Preeclampsia or a Pregnancy-Related Thrombotic Microangiopathy
Thrombosis
Large Thromboses Can Consume Platelets, Causing Transient Thrombocytopenia
This Typically occurs very early (within the first day or two) and is relatively mild, although more severe thrombocytopenia can occur
A series of four individuals with thrombocytopenia and an associated literature review documented platelet counts between 33,000 and 88,000/microL in the four with extensive venous thromboembolism (VTE) and platelet counts <150,000/microL in 10 percent of historical patients with a pulmonary embolus (mean platelet count, 293,000/microL (Am J Hematol, 2004) [MEDLINE]
Petechiae Commonly Occur in Association with Thrombocytopenia
Postpartum Hemorrhage
Postpartum Hemorrhage Commonly Occurs in Females with Underlying Bleeding Disorders
In Females with Type 1 Von Willebrand Disease and Symptomatic Hemophilia Carriers in Whom Levels of Von Willebrand Factor and Factor VIII Usually Normalize During Pregnancy, the Onset of Postpartum Hemorrhage May Be Delayed
Women with a History of Postpartum Hemorrhage Have a High risk of Recurrence in Subsequent Pregnancies
Ecchymoses (Bruises) are Nontender Areas of Bleeding into the Skin
Usually Associated with Multiple Colors Due to the Presence of Extravasated Blood (Red, Purple) and Breakdown Products of Heme Pigment (Green, Orange, Yellow)*
Ecchymoses Characteristically are Small, Multiple, and Superficial
However, Ecchymoses May Be Significant, Depending Upon the Degree of Thrombocytopenia
Ecchymoses May Develop without Noticeable Trauma and Do Not Spread into Deeper Tissues
Petechiae Commonly Occur in Association with Thrombocytopenia
Physiology
Petechiae are caused by red blood cell extravasation from capillaries
Clinical
They are asymptomatic, nontender, non-palpable, and do not blanch under pressure
They are most dense in dependent areas where the hydrostatic pressure on the small superficial vessels is greatest (eg, feet and ankles in ambulatory patients; presacral area in bedridden patients)
Petechiae are not found on the sole of the foot, where the vessels are protected by the strong subcutaneous tissue
Petechiae and other lesions should be noted, especially in the dependent parts of the body
Actively bleeding patients with thrombocytopenia should be transfused with platelets immediately to keep platelet counts above 50,000/microL in most bleeding situations including disseminated intravascular coagulation (DIC), and above 100,000k if there is central nervous system bleeding (Br J Haematol, 2009) [MEDLINE]
Platelet Transfusion in Advance of an Invasive Procedures (see Platelet Transfusion)
Platelet Transfusion in Advance of an Invasive Procedures (see Platelet Transfusion)
Typical Recommended Platelet Thresholds
General Comments
Most of the Data Used to Determine Bleeding Risk are Derived from Retrospective Studies of Patients Who are Afebrile and Have Thrombocytopenia But Not Coagulopathy (Transfusion, 2015) [MEDLINE] (Transfusion, 2017) [MEDLINE]
Neurosurgery/Ocular Surgery: <100k
Most Other Major Surgery: <50k
Endoscopic Procedures: <50k for therapeutic procedures; 20k for low risk diagnostic procedures
Bronchoscopy with Bronchoalveolar Lavage (BAL): <20-30k (Transfusion, 2016) [MEDLINE]
Thrombocytopenia Appears to Pose a Greater Hemorrhagic Risk, as Compared to Prolonged Clotting Times (Chest, 1996) [MEDLINE] (Intensive Care Med, 2002) [MEDLINE]
Retrospective studies suggest that no preprocedure reversal is warranted for platelet count >20 x 109/L and INR <3 (Transfusion, 2017) [MEDLINE]
Lumbar Puncture (LP) (see Lumbar Puncture): <10-20k in patients with hematologic malignancies and <40-50k in patients without hematologic malignancies; lower thresholds may be used in patients with immune thrombocytopenia (ITP) (Ann Hematol, 2003) [MEDLINE] (Br J Haematol, 2010) [MEDLINE] (Br J Haematol, 2011) [MEDLINE]
Platelet Transfusion to Prevent Spontaneous Hemorrhage (see Platelet Transfusion)
General Comments
There are No Ideal Tests for Predicting Which Patients Will Experience Spontaneous Hemorrhage in the Setting of Thrombocytopenia (Crit Rev Oncol Hematol, 2003) [MEDLINE]
Studies of patients with thrombocytopenia suggest that patients can bleed even with Platelet Counts >50k (NEJM, 2010) [MEDLINE]
However, bleeding is much more likely at platelet counts less than 5000/microL
Among individuals with platelet counts between 5000/microL and 50,000/microL, clinical findings can be helpful in decision-making regarding platelet transfusion
The platelet count at which a patient bled previously can be a good predictor of future bleeding
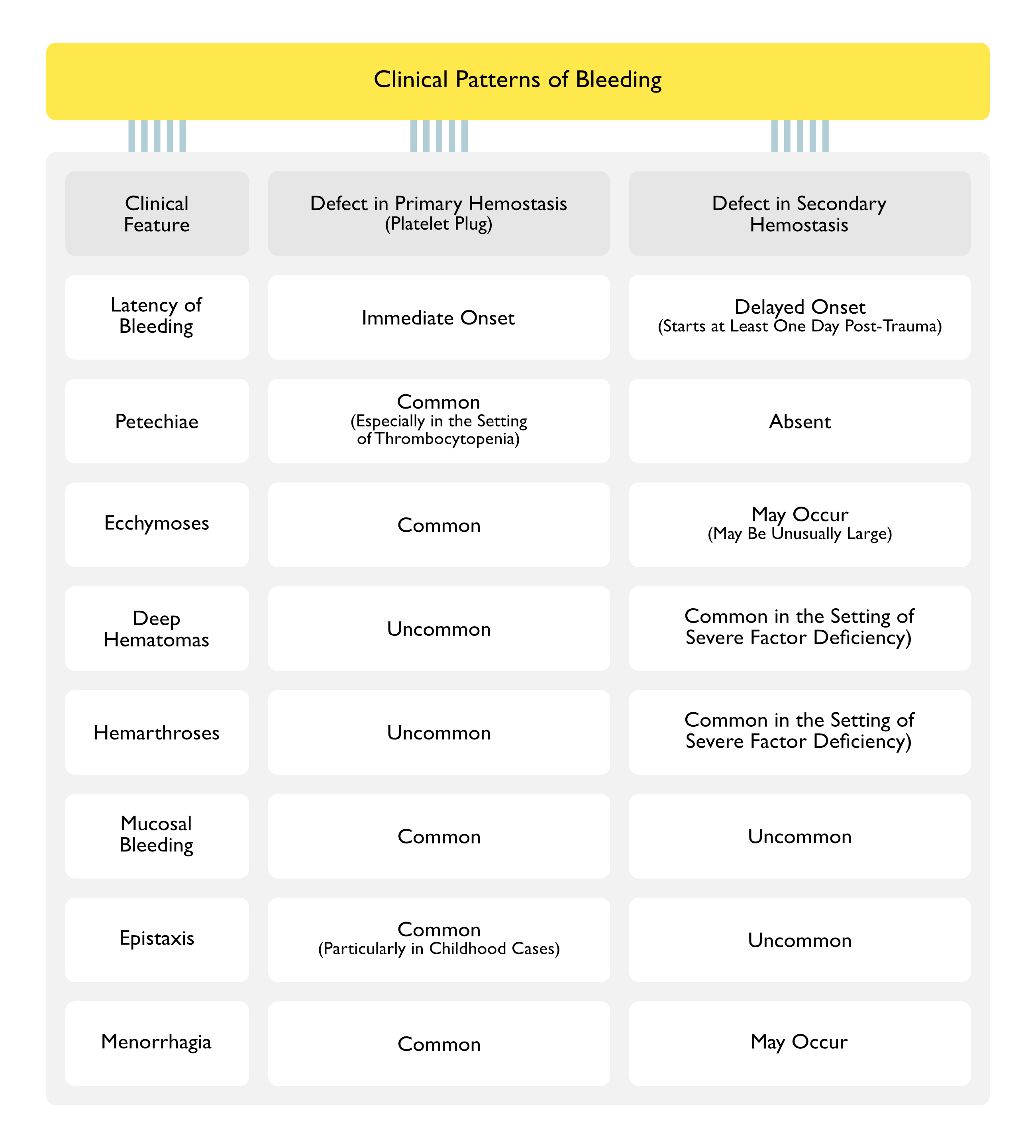
Petechial bleeding and ecchymoses are generally not thought to be predictive of serious bleeding, whereas mucosal bleeding and epistaxis (so-called “wet” bleeding) are thought to be predictive
Coexisting inflammation, infection, and fever also increase bleeding risk
The underlying condition responsible for a patient’s thrombocytopenia also may help in estimating the bleeding risk. As an example, some patients with ITP often tolerate very low platelet counts without bleeding, while patients with some acute leukemias that are associated with coagulopathy (eg, acute promyelocytic leukemia) can have bleeding at higher platelet counts (eg, 30,000 to 50,000/microL)
Compared with adults, children with bone marrow suppression may be more likely to experience bleeding at the same degree of thrombocytopenia
In a secondary subgroup analysis of the PLADO trial, in which patients were randomly assigned to different platelet doses, children had more days of bleeding, more severe bleeding, and required more platelet transfusions than adults with similar platelet counts (Blood, 2012) [MEDLINE]
However, these findings do not suggest a different threshold for platelet transfusion in children, as the increased risk of bleeding was distributed across a wide range of platelet counts
Tests for platelet-dependent hemostasis (ie, bleeding time, thromboelastography (TEG), and other point of care tests) are generally not used to predict bleeding in thrombocytopenic patients
Recommendations for Thrombocytopenic Patients with Bone Marrow Suppression
Prophylactic Platelet Transfusion to Prevent Spontaneous Bleeding are Recommended in Most Afebrile Patients with Platelet Counts <10k Due to Bone Marrow Suppression
Higher Platelet Transfusion Thresholds (i.e. 20-30k) Should Be Used in Patients Who are Febrile or Septic
Standard Practice is to Transfuse at a Threshold Platelet Count of <10-20k for Most Patients with Severe Hypoproliferative Thrombocytopenia Due to Hematologic Malignancy, Cytotoxic Chemotherapy, and Hematopoietic Stem Cell Transplant (HSCT) (Br J Haematol, 2011) [MEDLINE]
Recommendations for Thrombocytopenic Patients with Immune Thrombocytopenic Purpura (ITP) (see xxxx)
Platelet transfusion is Only Recommended for bleeding rather than at a specific platelet count
Circulating platelets in patients with ITP tend to be highly functional, and platelet counts tend to be well above 30,000/microL
Bleeding is rare even in patients with severe thrombocytopenia (platelet count <30,000/microL)
Recommendations for Thrombocytopenic Patients with Thrombotic thrombocytopenic purpura (TTP) and heparin-induced thrombocytopenia (HIT)
Platelet consumption causes thrombocytopenia and an increased risk of bleeding; the underlying platelet activation in these conditions also simultaneously increases the risk of thrombosis
prophylactic platelet transfusions are Not routinely Recommended in patients with TTP or HIT
Platelet transfusions can be helpful or even life-saving in patients with these conditions who are bleeding and/or have anticipated bleeding due to a required invasive procedure (eg, placement of a central venous catheter), and platelet transfusion should not be withheld from a bleeding patient due to concerns that platelet transfusion will exacerbate thrombotic risk
However, platelet transfusions may cause a slightly increased risk of thrombosis in patients with these conditions
Thus, we do not use prophylactic platelet transfusions routinely in patients with TTP or HIT
Support for this approach comes from a large retrospective review of hospitalized patients with TTP and HIT, in which platelet transfusion was associated with a very slight increased risk of arterial thrombosis but not venous thromboembolism (Blood, 2015) [MEDLINE]
In contrast, the review found that patients with immune thrombocytopenia (ITP) had no increased risk of arterial or venous thrombosis with platelet transfusion
Of note, this was a retrospective study in which sicker patients were more likely to have received platelets, and the temporal relationships between platelet transfusions and thromboses were not assessed.
Liver disease and disseminated intravascular coagulation (DIC) are two processes that can cause a complex mixture of abnormalities with procoagulant and anticoagulant effects, along with thrombocytopenia; patients with either of these disorders are at risk for both thrombosis and bleeding
There is no evidence to support the administration of platelets in these patients if they are not bleeding
However, platelet transfusion is justified in patients who have serious bleeding, are at high risk for bleeding (eg, after surgery), or require invasive procedures
Clinical Efficacy
Randomized SToP Trial of Low-Dose Platelet Transfusion Strategy in the Setting of Thrombocytopenia (Blood, 2009) [MEDLINE]
Thrombocytopenic adults requiring prophylactic platelet transfusion were randomly allocated to standard-dose (300-600 x 10(9) platelets/product) or low-dose (150- <300 x 10(9) platelets/product) platelets
Data Safety Monitoring Board stopped the study because the difference in the grade 4 bleeding reached the prespecified threshold of 5%
At this time, 129 patients had been randomized and 119 patients were included in the analysis (58 low dose; 61 standard dose)
Three patients in the low-dose arm (5.2%) had grade 4 bleeds compared with none in the standard-dose arm
WHO bleeding grade 2 or higher was 49.2% (30/61) in the standard-dose arm and 51.7% (30/58) in the low-dose group (relative risk [RR], 1.052; 95% confidence interval [CI], 0.737-1.502)
A higher rate of grade 4 bleeding in patients receiving low-dose prophylactic platelet transfusions resulted in this Trial Being Stopped
Whether this finding was due to chance or represents a real difference requires further investigation.
Prognosis
Thrombocytopenia and Mortality Rate in the Intensive Care Unit (ICU) Setting
Both a Low Nadir Platelet Count and a Large Fall in the Platelet Count Predict a Poor Outcome in Adult Intensive Care Unit Patients (Crit Care Med, 2000) [MEDLINE]
In a logistic regression analysis with ICU mortality as the dependent variable, the occurrence of thrombocytopenia had more explanatory power than admission variables, including APACHE II, SAPS II, and MODS scores (Adjusted Odds Ratio 4.2; 95% CI: 1.8-10.2)
In the Intensive Care Unit, Patients Who Develop Thrombocytopenia are More Likely to Bleed, Receive Transfusions, and Die (Chest, 2013) [MEDLINE]
Moderate and Severe Thrombocytopenia are Associated with Increased Intensive Care Unit and Hospital Mortality Rates
References
Epidemiology
Thrombocytopenia and prognosis in intensive care. Crit Care Med. 2000;28(6):1871 [MEDLINE]
Thrombocytopenia in patients in the medical intensive care unit: bleeding prevalence, transfusion requirements, and outcome. Crit Care Med. 2002;30(8):1765 [MEDLINE]
The frequency and clinical significance of thrombocytopenia complicating critical illness: a systematic review. Chest. 2011 Feb;139(2):271-8 [MEDLINE]
Thrombocytopenia in critically ill patients receiving thromboprophylaxis: frequency, risk factors, and outcomes. Chest. 2013;144(4):1207 [MEDLINE]
Etiology
Pooling of platelets in the spleen: role in the pathogenesis of “hypersplenic” thrombocytopenia. J Clin Invest. 1966;45(5):645 [MEDLINE]
Hemostasis in massively transfused trauma patients. Ann Surg. 1979;190(1):91 [MEDLINE]
Laboratory hemostatic abnormalities in massively transfused patients given red blood cells and crystalloid. Am J Clin Pathol. 1991;96(6):770 [MEDLINE]
Evidence for prevention of death and myocardial infarction with platelet membrane glycoprotein IIb/IIIa receptor blockade by abciximab (c7E3 Fab) among patients with unstable angina undergoing percutaneous coronary revascularization. EPIC Investigators. Evaluation of 7E3 in Preventing Ischemic Complications. J Am Coll Cardiol. 1997 Jul;30(1):149-56. doi: 10.1016/s0735-1097(97)00110-1 [MEDLINE]
Pseudothrombocytopenia after abciximab (Reopro) treatment. Circulation 1999; 100:1460
Thrombocytopenia complicating treatment with intravenous IIb/IIIa receptor inhibitors: a pooled analysis. Am Heart J 2000; 140:206-211
Thrombocytopenia due to acute venous thromboembolism and its role in expanding the differential diagnosis of heparin-induced thrombocytopenia. Am J Hematol. 2004;76(1):69 [MEDLINE]
Vancomycin-induced immune thrombocytopenia. N Engl J Med. 2007 Mar 1;356(9):904-10 [MEDLINE]
Severe vitamin B-12 deficiency in a child mimicking thrombotic thrombocytopenic purpura. Pediatr Blood Cancer. 2009 Mar;52(3):420-2 [MEDLINE]
Systemic malignancies as a cause of unexpected microangiopathic hemolytic anemia and thrombocytopenia. Oncology (Williston Park). 2011;25(10):908 [MEDLINE]
Prevalence and indicators of portal hypertension in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2012 Sep;10(9):1028-33.e2 [MEDLINE]
Cobalamin deficiency causing severe hemolytic anemia: a pernicious presentation. Am J Med. 2015;128(10):e5 [MEDLINE]
Atypical aHUS: State of the art. Mol Immunol. 2015;67(1):31 [MEDLINE]
Clinical features of vitamin B12 deficiency mimicking thrombotic microangiopathy. Br J Haematol. 2020;191(5):938 [MEDLINE]
Histone-Associated Thrombocytopenia in Patients Who Are Critically Ill. JAMA. 2016;315(8):817-819. doi:10.1001/jama.2016.0136 [MEDLINE]
Drug-associated thrombocytopenia. Hematology Am Soc Hematol Educ Program. 2018 Nov 30;2018(1):576-583. doi: 10.1182/asheducation-2018.1.576 [MEDLINE]
A case of acute pancreatitis-induced microangiopathic hemolytic anemia with thrombocytopenia. J Thromb Thrombolysis. 2020 Jan;49(1):159-163. doi: 10.1007/s11239-019-01946-2 [MEDLINE]
Severe vitamin B12 deficiency causing pseudo-thrombotic microangiopathy. CMAJ. 2023;195(38):E1300 [MEDLINE]
Physiology
Pooling of platelets in the spleen: role in the pathogenesis of “hypersplenic” thrombocytopenia. J Clin Invest. 1966;45(5):645 [MEDLINE]
Thrombokinetics in man. J Clin Invest. 1969;48(6):963 [MEDLINE]
An improved method for the quantification of the in vivo kinetics of a representative population of 111In-labelled human platelets. Eur J Nucl Med. 1985;10(11-12):522 [MEDLINE]
Programmed anuclear cell death delimits platelet life span. Cell. 2007;128(6):1173 [MEDLINE]
Platelet senescence is regulated by an internal timer, not damage inflicted by hits. Blood. 2010;116(10):1776 [MEDLINE]
Sialylation on O-glycans protects platelets from clearance by liver Kupffer cells. Proc Natl Acad Sci U S A. 2017;114(31):8360 [MEDLINE]
Clinical
Central venous catheter placement in patients with disorders of hemostasis. Chest. 1996;110(1):185 [MEDLINE]
Central venous catheter use. Part 1: mechanical complications. Intensive Care Med. 2002;28(1):1 [MEDLINE]
Central venous catheter placement in coagulopathic patients: risk factors and incidence of bleeding complications. Transfusion. 2017;57(10):2512 [MEDLINE]
Treatment
Thrombocytopenia and hemorrhagic risk in cancer patients. Crit Rev Oncol Hematol. 2003 Oct;48(Suppl):S13-6 [MEDLINE]
Safety of lumbar puncture for adults with acute leukemia and restrictive prophylactic platelet transfusion. Ann Hematol. 2003;82(9):570 [MEDLINE]
The risk of spinal haematoma following neuraxial anaesthesia or lumbar puncture in thrombocytopenic individuals. Br J Haematol. 2010;148(1):15 [MEDLINE]
Dose of prophylactic platelet transfusions and the prevention of hemorrhage. N Engl J Med 2010; 362:600-613 [MEDLINE]
A randomized controlled trial comparing standard- and low-dose strategies for transfusion of platelets (SToP) to patients with thrombocytopenia. Blood 2009; 113:1564-1573 [MEDLINE]
Evidence-based platelet transfusion guidelines. Hematology Am Soc Hematol Educ Program 2007:172- 178 [MEDLINE]
Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br J Haematol. 2009;145(1):24 [MEDLINE]
Dose of prophylactic platelet transfusions and prevention of hemorrhage. N Engl J Med. 2010;362(7):600 [MEDLINE]
Personal practice: how we manage the risk of bleeding and thrombosis in children and young adults with acute lymphoblastic leukaemia. Br J Haematol. 2011 Mar;152(5):505-11 [MEDLINE]
Platelet transfusions for patients with haematological malignancies: who needs them? Br J Haematol. 2011;154(4):425 [MEDLINE]
Optimal preprocedural platelet transfusion threshold for central venous catheter insertions in patients with thrombocytopenia. Transfusion. 2011 Nov;51(11):2269-76 [MEDLINE]
Bleeding risks are higher in children versus adults given prophylactic platelet transfusions for treatment-induced hypoproliferative thrombocytopenia. Blood. 2012;120(4):748 [MEDLINE]
Platelet transfusion: a systematic review of the clinical evidence. Transfusion. 2015 May;55(5):1116-27 [MEDLINE]
Platelet transfusions in platelet consumptive disorders are associated with arterial thrombosis and in-hospital mortality. Blood. 2015;125(9):1470 [MEDLINE]
Bronchoscopy can be done safely in patients with thrombocytopenia. Transfusion. 2016 Feb;56(2):344-8 [MEDLINE]
Preprocedural platelet transfusion for patients with thrombocytopenia undergoing interventional radiology procedures is not associated with reduced bleeding complications. Transfusion. 2017;57(4):890 [MEDLINE]