Allows Invasive Measurement of Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP)
Arterial Line Placement with Invasive Blood Pressure Measurement is Generally Recommended in the Setting of Shock (Especially When Vasopressors are Required)
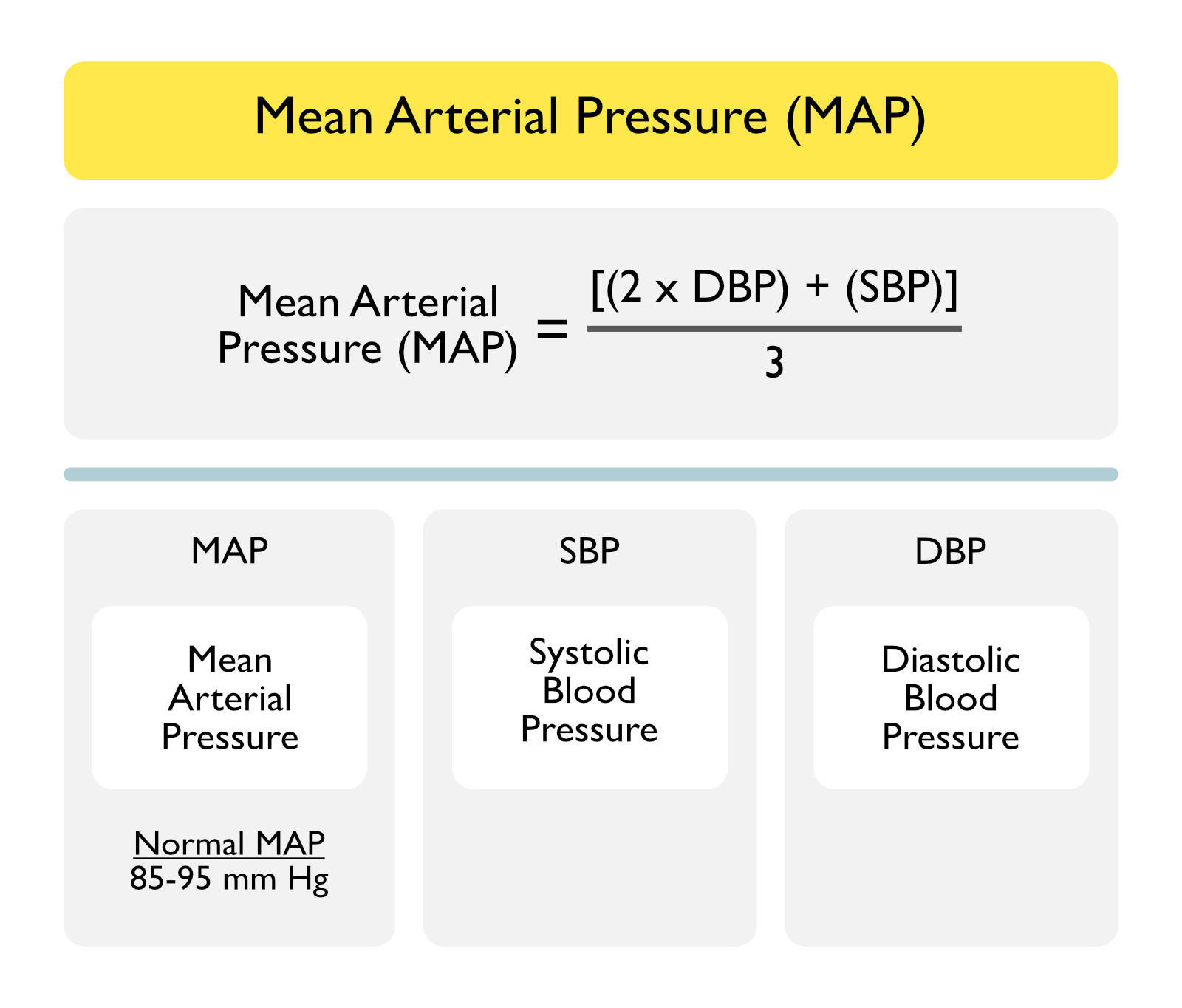
Equation for the Mean Arterial Pressure (MAP)
MAP = [(2 x DBP) + (SBP)]/3
Twice as Much of the Cardiac Cycle is Spent in Diastole, Relative to Systole
Terms
MAP: mean arterial blood pressure (in mm Hg)
SBP: systolic blood pressure (in mm Hg)
DBP: diastolic blood pressure (in mm Hg)
Normal MAP: 85-95 mm Hg
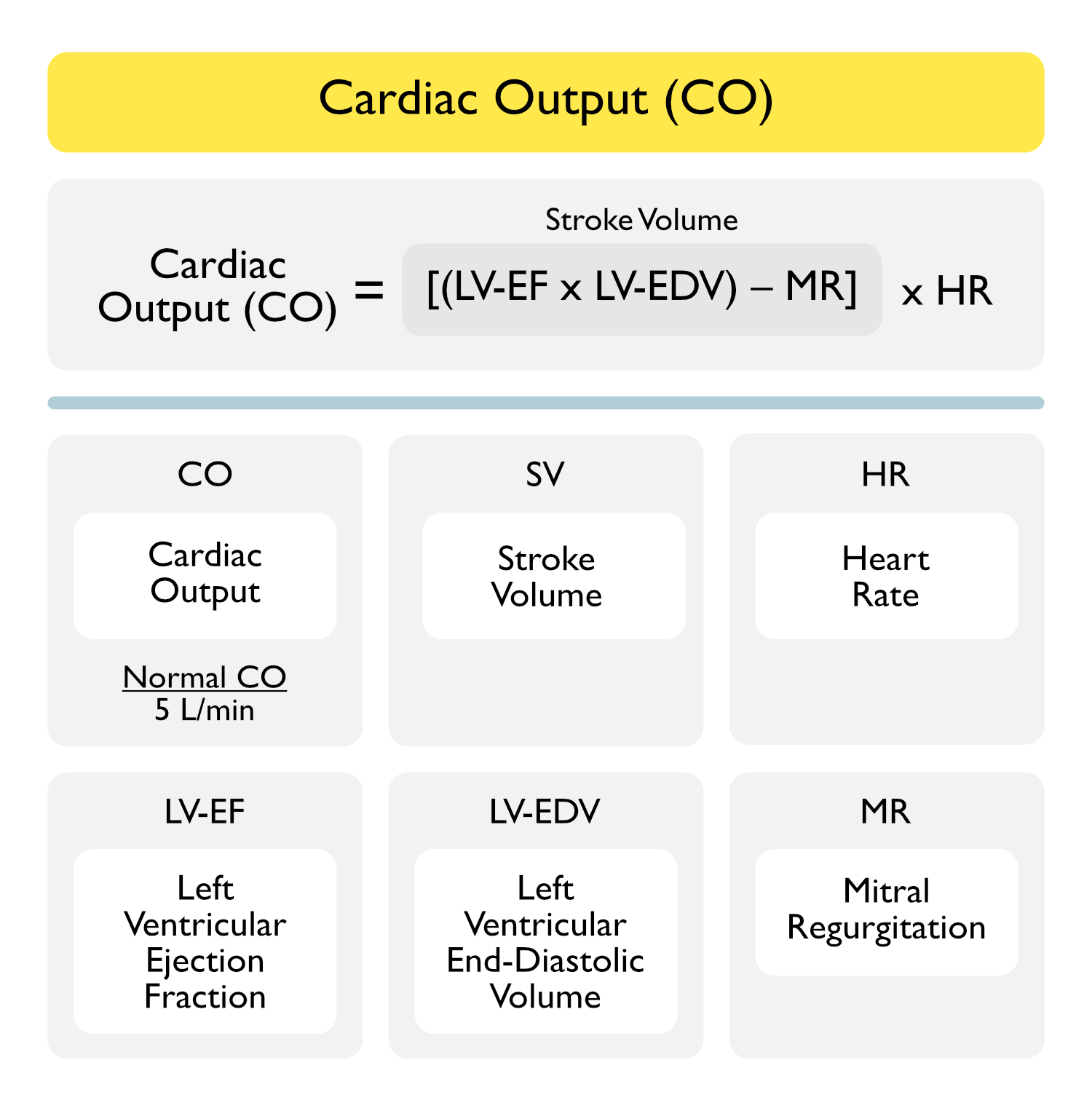
Cardiac Output (CO)
Cardiac Output Measurement Technique
Thermodilution Cardiac Output (Utilizing a Swan-Ganz Catheter) (see Swan-Ganz Catheter)
Thermodilution Method Allows Measurement of Cardiac Output Using the Injection of Cold Saline through a Port on the Swan-Ganz Catheter, Using a Temperature-Sensitive Thermistor on the Catheter to Measure the Rate of Clearance of the Cold Saline
Utilizing Principles Developed by Fick in the Late 19th Century, the Rate of Clearance of Cold Saline is Proportional to the Blood Flow Rate (i.e. Cardiac Output)
The Area Under the Thermodilution Curve is Inversely Related to the Cardiac Output (i.e. High Cardiac Output Results in Rapid Clearance of the Cold Saline, Resulting in a Small Area Under the Curve)
Variability in Serial Thermodilution Cardiac Output Measurements
Variability in Cardiac Output Values Obtained by Thermodilution is Approximately 10%
Therefore, Changes in Cardiac Output Should Generally Be on the Order of 15% to Be Regared as Valid
Etiology of Falsely Decreased Cardiac Output
Tricuspid Regurgitation (TR) (see Tricuspid Regurgitation: local “recirculation” of injectate mimics slow injectate clearance
Pulmonic Regurgitation (see Pulmonic Regurgitation): local “recirculation” of injectate mimics slow injectate clearance
Erroneously High Cold Saline Injectate Volume
Etiology of Falsely Increased Cardiac Output
Intracardiac Shunt (in Either Direction) (see Intracardiac and Extracardiac Shunt): alters curve and makes cardiac output calculation less accurate
Low Cardiac Output State: injectate can disperse into the surrounding tissue, mimicking rapid injectate clearance
Erroneously Low Cold Saline Injectate Volume
Early Recirculation on Thermodilution Curve
Suggests Presence of Left-to-Right Intracardiac Shunt
Continuous Cardiac Output Measurement
Swan-Ganz Catheters with the Capability to Measure Cardiac Output “continuously” (Actually Averages the Cardiac Output Over a Few Minute Window) are Commercially Available
Fick Cardiac Output
Fick Cardiac Output = Oxygen Consumption/(10 x Arterial-Venous Oxygen Difference)
Determination of Oxygen Consumption
Oxygen Consumption (Estimated) Can Be Obtained from a Nomogram Which Utilizes Age, Sex, Height, and Weight
Oxygen Consumption Can Also Be Determined Using Breath Analysis
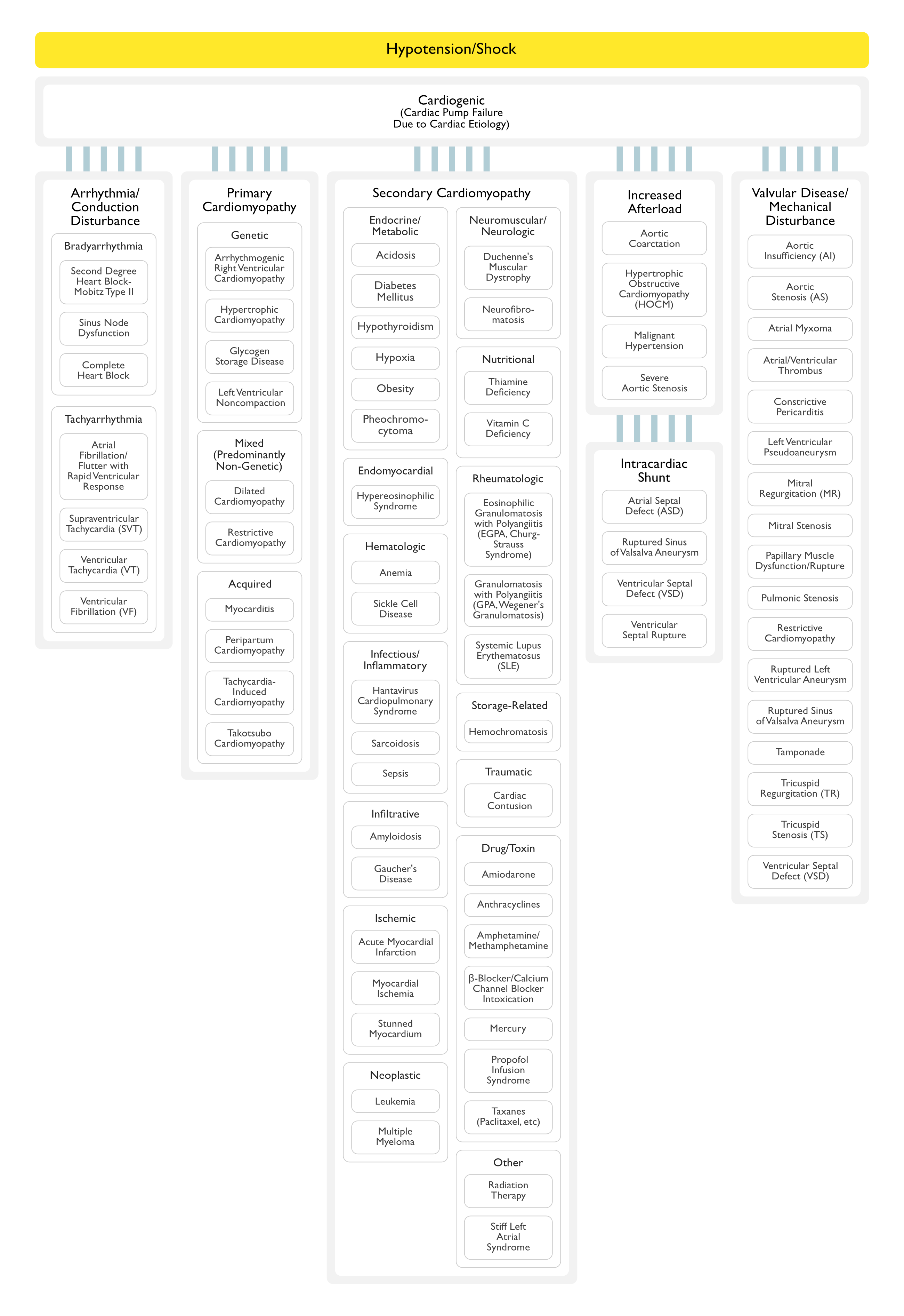
Mixed (Predominantly Non-Genetic; Familial Disease with a Genetic Origin has been Reported in a Minority of Cases)
Dilated Cardiomyopathy: this is a heterogeneous group of disorders characaterized by ventricular dilation and decreased myocardial contractility in the absence of abnormal loading (valvular heart disease, hypertension)
Restrictive Cardiomyopathy (Non-Dilated and Non-Hypertrophied)
Acquired
Cardiomyopathy in Infants of Insulin-Dependent Diabetic Mothers
Myocarditis (Inflammatory Cardiomyopathy) (see Myocarditis)
Pharmacology: negative inotropy can occur in patients with preexisting left ventricular dysfunction with EF <35% (amiodarone also casuses peripheral vasodilation, which may offset some of the negative inotropy)
Narrowing of Descending Aorta (Typically at the Insertion of the Ductus Arteriosus Distal to the Left Subclavian Artery), Resulting in Left Ventricular Pressure Overload
Ruptured Sinus of Valsalva Aneurysm May Produce Aortic Insufficiency, Tricuspid Regurgitation, Left-to-Right or Right-to-Left Shunt, and/or Sudden Cardiac Death
Aortic Insufficiency May Be Acute in the Setting of Ascending Aortic Dissection
Physiology
Portion of Left Ventricular Stroke Volume Regurgitates Back from the Aorta into the Left Ventricle, Resulting in Increased Left Ventricular End-Diastolic Volume and Increased Left Ventricular Wall Stress
Cardiac Rupture is Contained by Adherent Pericardium or Scar Tissue (Pseudoaneurysm Contains No Endocardium or Myocardium), Resulting in Decreased Stroke Volume
In Cases Where Left Ventricular Pseudoaneurysm Rupture Occurs, Tamponade May Occur
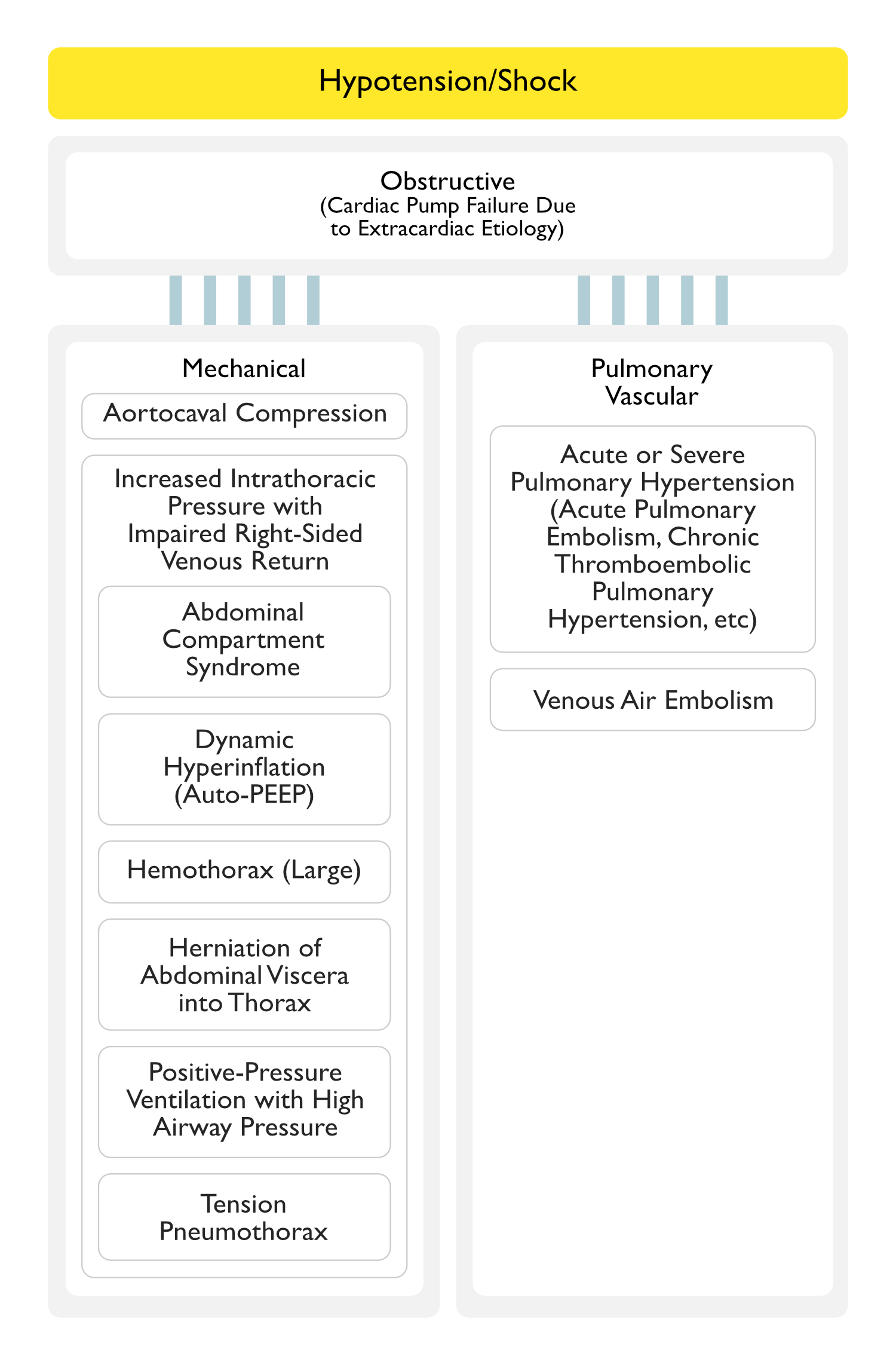
Increased Intrathoracic Pressure, Resulting in Impaired Right-Sided Venous Return
Herniation of Abdominal Viscera Into Thorax
Physiology
Due to Movement of Abdominal Visceral Contents into the Thoracic Cavity, there is Increased Intrathoracic Pressure, Resulting in Impaired Right-Sided Venous Return
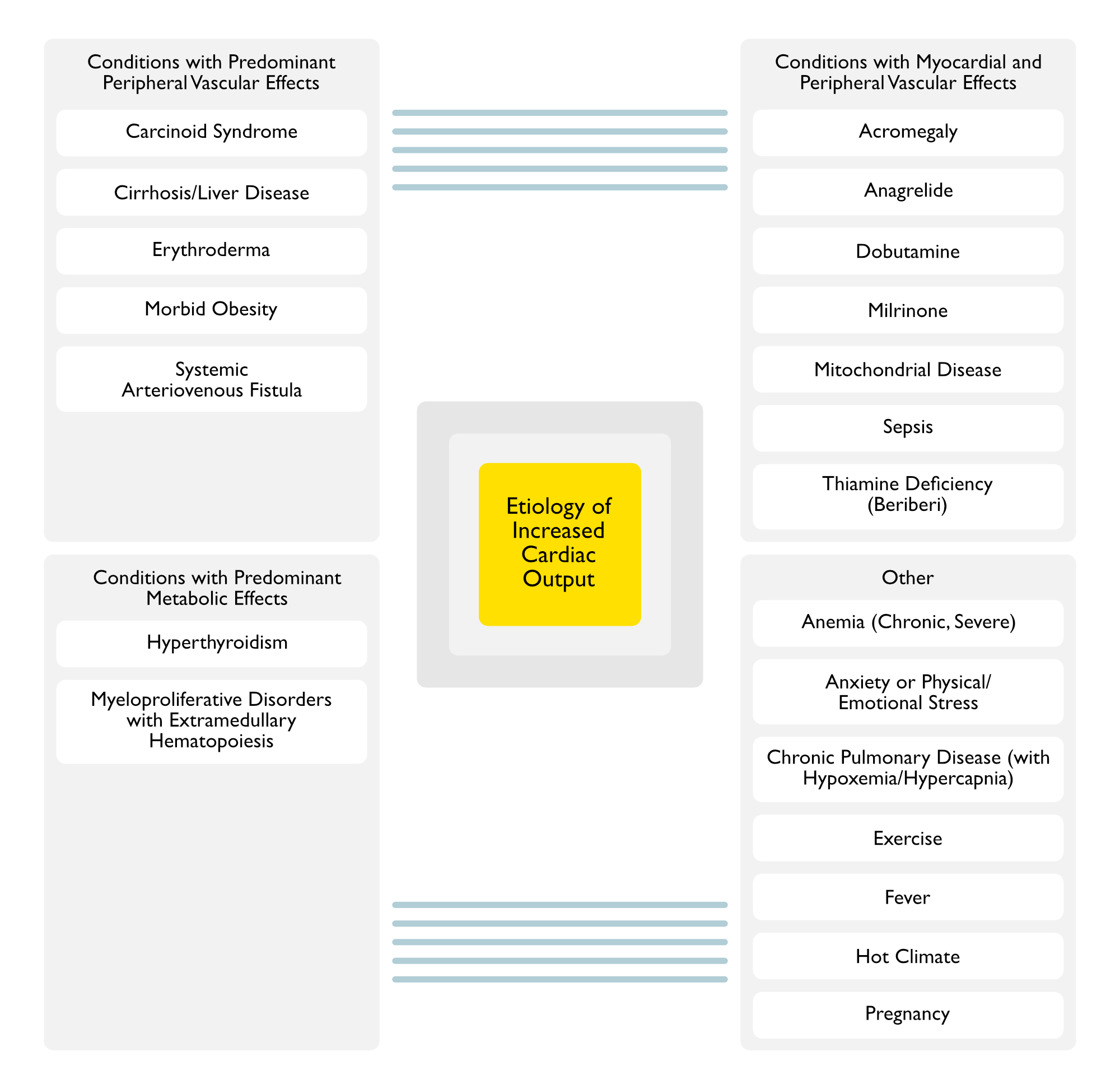
Etiology of Increased Cardiac Output (J Am Coll Cardiol, 2016) [MEDLINE])
General Comments
Many of the Following Conditions are Classified as Etiologies of “High Output Heart Failure”
However, this Term is a Misnomer, Since the Heart is Generally Normal (Capable of Generating a High Cardiac Output) and the Underlying Pathophysiology is Decreased Systemic Vascular Resistance, Resulting in Activation of Neurohormones Which Increase Renal Salt and Water Retention (and May Result in Hypotension)
Treatment with Vasodilators (Typically Used in Congestive Heart Failure) May Exacerbate the Heart Failure in These Conditions
Conditions with Predominant Peripheral Vascular Effects
Peripheral Vasodilation with Decreased Systemic Vascular Resistance
Clinical
High Cardiac Output/Low Systemic Vascular Resistance State Has Been Reported in Some Cases (Ann Intern Med, 1994) [MEDLINE] (Neth J Med, 2002) [MEDLINE]
However, Heart Failure with Right Heart Valvular Fibrosis is a More Common Cardiac Presentation
Progressive Systemic Vasodilation (Especially Splanchnic) with Development of Intrahepatic/Mesenteric Arteriovenous Shunts
Intrapulmonary Arteriovenous Shunts (i.e. Hepatopulmonary Syndrome) May Also Occur (Echocardiography, 2006) [MEDLINE] (see Hepatopulmonary Syndrome)
Clinical
Characteristically Produces a High Cardiac Output/Low Systemic Vascular Resistance State
High Output Heart Failure May Occur
Of All of the High Output Heart Failure Conditions, Cirrhosis Generally Produces the Lowest Arterial-Venous Oxygen Difference and the Lowest Systemic Vascular Resistance
Multiple Myeloma (see Multiple Myeloma): due to multiple minute arteriovenous fistulas in bony lesions
Paget Disease of the Bone (Osteitis Deformans) (see Paget Disease of Bone): due to multiple minute arteriovenous fistulas in bony lesions
Polyostotic Fibrous Dysplasia (McCune-Albright Syndrome): due to multiple minute arteriovenous fistulas in bony lesions
Trauma
Aortocaval Fistula
Bullet/Knife Wound (Particularly in the Thigh)
Physiology
High Pressure Arterial Blood is Shunted into a Low Pressure Vein, Shunting Past the Tissue Capillary Bed (and Decreasing the Systemic Vascular Resistance)
Subsequently, there is a Compensatory Increase in Stroke Volume, Cardiac Output, and Total Plasma Volume to Maintain Capillary Perfusion
High Cardiac Output/Low Systemic Vascular Resistance State May Occur (with High Output Heart Failure) (NEJM, 2001) [MEDLINE]
Sympatholytic Agents (β-Blockers) Can Partially Decrease Heart Rate and Cardiac Output, as Well as Partially Improve Pulse Pressure
Hyperthyroidism-Associated Hyperdynamic Right Ventricular Function (Which is Reversible with Treatment) Has Also Been Reported (Heart Lung Circ, 2017) [MEDLINE]
Hyperthyroidism-Associated Decreased Cardiac Output May Alternately Occur (Due to Tachycardia-Mediated Cardiomyopathy or Associated Cardiac Disease) (Heart, 2007) [MEDLINE]
Hyperthyroidism-Associated Reversible Right Ventricular Failure with Pulmonary Hypertension Has Also Been Reported (Am J Med Sci, 2018) [MEDLINE]
Myeloproliferative Disorders with Extramedullary Hematopoiesis
Due to Inflammatory Response (Involving TNF-α, IL-1β, IL-6, etc)
Clinical
Characteristically Produces a High Cardiac Output/Low Systemic Vascular Resistance State (Although Sepsis-Induced Myocardial Dysfunction May Alternately Occur)
High Output Heart Failure May Occur
Thiamine (Vitamin B1) Deficiency (Beriberi) (see Thiamine)
Physiology
Vasodilation May Occur Due to Direct Depression of Vasomotor Function (Am J Med, 1966) [MEDLINE]
Thiamine Deficiency Impairs Lactate and Pyruvate Utilization by the Myocardium (These Substrates are Important for Oxidation and Energy Production in the Myocardium)
Placental Blood Flow (Which May Function an Arteriovenous Shunt)
Systemic Vascular Resistance (SVR)
Calculation of Systemic Vascular Resistance (SVR) Using Pressures Measured from Swan-Ganz Catheter (see Swan-Ganz Catheter)
Calculation Technique
Systemic Vascular Resistance (SVR) is Calculated from the Mean Arterial Pressure (MAP), Central Venous Pressure (CVP), and Cardiac Output (CO)
Unlike, Systemic Vascular Resistance, All Three of These Latter Parameters are Measured
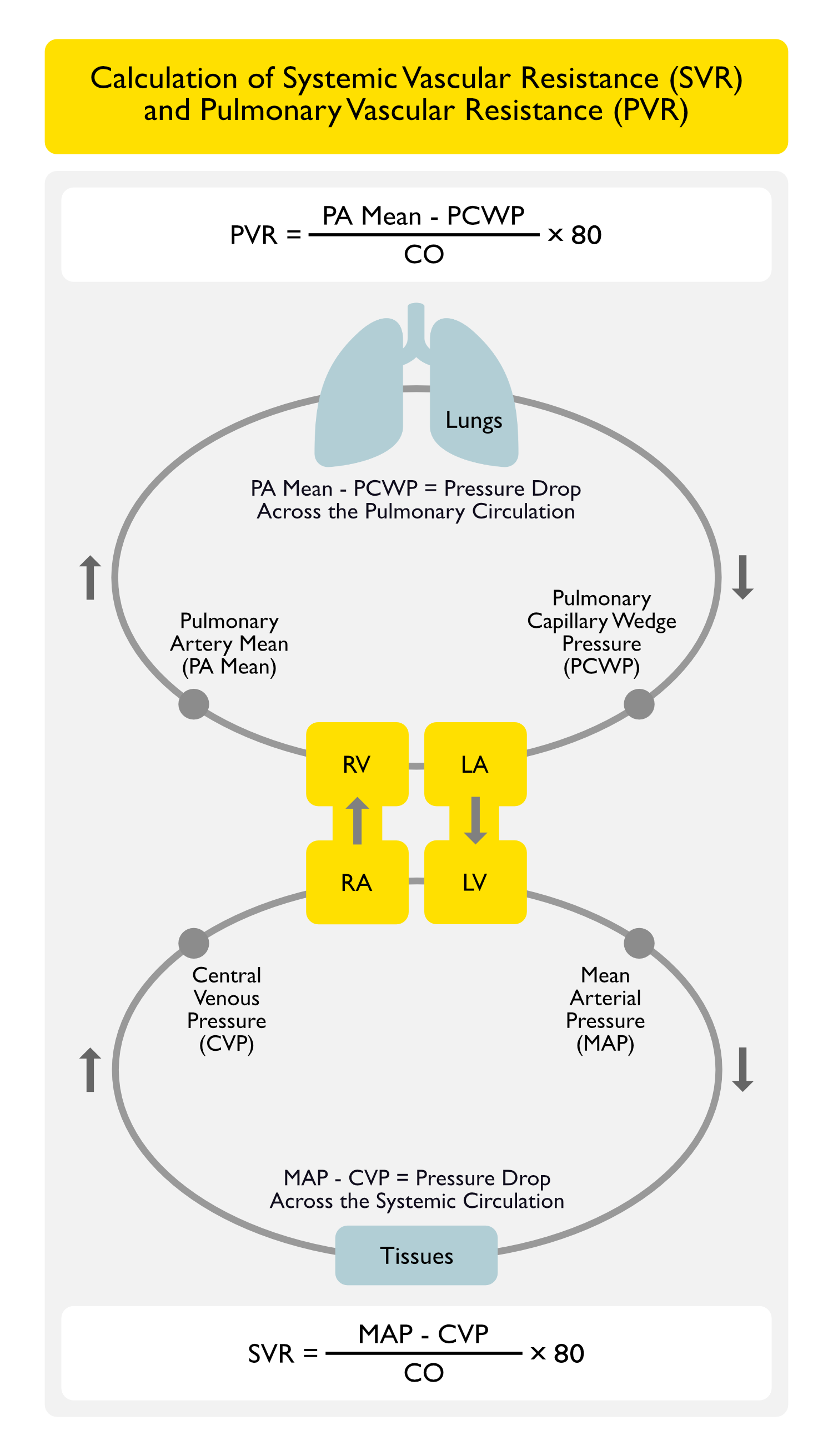
Equation: SVR = [(MAP-CVP)/CO] x 80
Normal SVR Values (using dynes-sec/cm5): 770-1500 dynes-sec/cm5
Note: SVR normal values can alternatively be expressed as 9–20 Woods units (9-20 mm Hg-min/L) -> to convert from Woods units to dynes-sec/cm5, multiply by 80
Etiology of Decreased Systemic Vascular Resistance (Distributive Shock)
Air Bubbles Occlude the Arterial Microcirculation, Resulting in Ischemia-Induced Endothelial Damage and Release of Inflammatory Mediators, Culminating in End-Organ Injury
Venous Air Embolism
Air Bubbles in the Pulmonary Microcirculation Result in Local Endothelial Damage, Culminating in Bronchospasm/Acute Lung Injury
Cases of Hypocalcemia-Associated Hypotension Have Been Extensively Reported (Am J Kidney Dis, 1994) [MEDLINE] (Am J Kidney Dis, 2015) [MEDLINE] (Hemodial Int, 2016) [MEDLINE]
Hypocalcemia-Associated Hypotension is Most Commonly Seen When it is Rapidly Induced by Ethylenediaminetetraacetic Acid (EDTA), Transfusion of Citrated Blood, Products, or with the Use of Low Calcium Dialysate in Patients Undergoing Dialysis
Inhibition of Phosphodiesterase 5/PDE5 (the Enzyme Which Degrades cGMP), Resulting in Enhanced NO-Mediated Smooth Muscle Relaxation and Therefore, Peripheral Vasodilation
Femoral Arteriovenous Fistula: most common type of acquired arteriovenous fistula (due to the frequency of using the femoral site for percutaneous arterial or venous access)
Calculation of Pulmonary Vascular Resistance (PVR) Using Pressures Measured from Swan-Ganz Catheter (see Swan-Ganz Catheter)
Calculation Technique
Pulmonary Vascular Resistance (PVR) is Calculated from the Mean Arterial Pressure (MAP), Central Venous Pressure (CVP), and Cardiac Output (CO)
Unlike, Pulmonary Vascular Resistance, All Three of These Latter Parameters are Measured
Equation: PVR = [(PA Mean – PCWP)/CO] x 80
Normal PVR Values (using dynes-sec/cm5): 20-120 dynes-sec/cm5
Note: PVR normal values can alternatively be expressed as 0.25–1.6 Woods units (or 0.25–1.6 mm Hg-min/L) -> to convert from Woods units to dynes-sec/cm5, multiply by 80
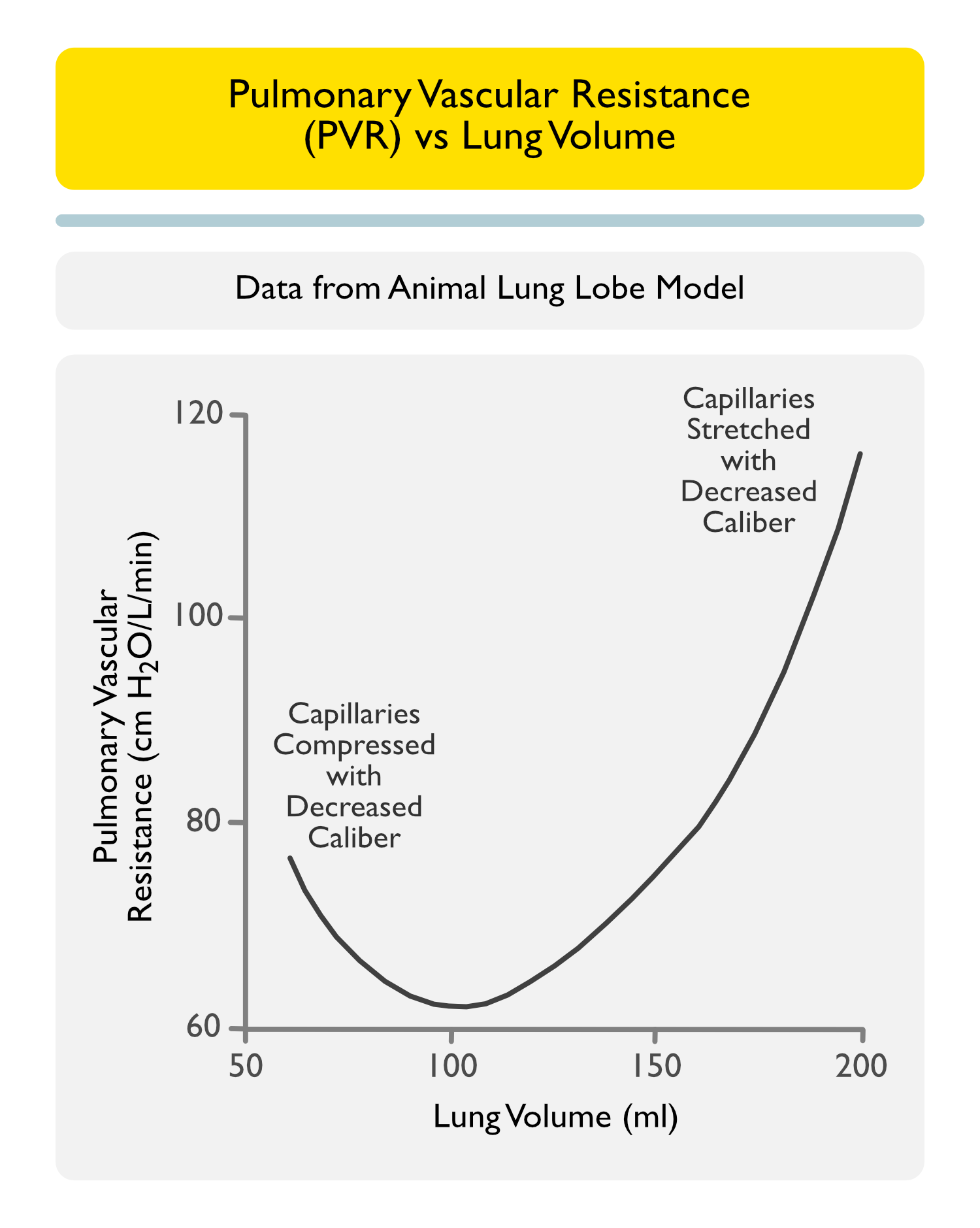
Etiology of Increased Pulmonary Vascular Resistance (PVR)
Very Low Lung Volume/Atelectasis (see Atelectasis)
Mechanism
Capillaries are Compressed, Increasing Pulmonary Vascular Resistance (PVR)
Hypercapnic Pulmonary Vasoconstriction May Be Responsive to Nitric Oxide
When Associated with High PEEP in the Setting of ARDS, Hypercapnic Pulmonary Vasoconstriction May Result in RV Dysfunction (Intensive Care Med, 2009) [MEDLINE]
Distal Port is Traditionally Located in Either the Superior Vena Cava (or the Right Atrium)
Clinical Efficacy Data
Clinical Efficacy-Measurement of Central Venous Pressure (CVP) Via a Peripherally Inserted Central Catheter (PICC) (see Peripherally Inserted Central Catheter)
General Comments
Peripherally Inserted Central Catheter (PICC) Has a Longer Length and a Narrower Lumen than a Central Venous Catheter (CVC)
Peripherally Inserted Central Catheter (PICC) has a Higher Intrinsic Resistance than a Central Venous Catheter (CVC)
Central Venous Pressure (CVP) Monitoring is an Indicated Use by Several Commercially Available Peripherally Inserted Central Catheters (PICC’s)
AngioDynamics
Arrow
Bard
Medcomp
Early Study Comparing Central Venous Pressure (CVP) Obtained from Central Venous Catheters (CVC’s) and Peripherally Inserted Central Catheters (PICC’s) (2000) [MEDLINE]: study used 77 data pairs from 12 patients with measurements recorded at end-expiration in 19-gauge double-lumen peripherally inserted central catheters (PICC’s) (zeroed at the right atrium)
Peripherally Inserted Central Catheters (PICC’s) Used in This Study Did Not Have High Infusion Rate Capability
To Overcome the Higher Intrinsic Resistance of the Peripherally Inserted Central Catheter (PICC), a Continuous Infusion Device was Used with Heparinized Saline at 3 mL/hr (as is Commonly Used for Arterial Lines)
Central Venous Pressure (CVP) Recorded from a Peripherally Inserted Central Catheter (PICC) is About 1 mm Hg Higher than that Obtained from Central Venous Pressure (CVP) Recorded from a Central Venous Catheter (CVC) (This Difference is Believed to Be Clinically Insignificant)
Peripherally Inserted Central Catheters (PICC’s) Can Be Used to Measure Central Venous Pressure (CVP), Provided that Continuous Infusion Device is Used with Heparinized Saline
Operative Study During AAA Repair Comparing Central Venous Pressure (CVP) Obtained from Central Venous Catheters (CVC’s) and Peripherally Inserted Central Catheters (PICC’s) (2006) [MEDLINE]
Peripherally Inserted Central Catheters (PICC’s) are an Effective Method for Central Venous Pressure (CVP) Monitoring in Situations of Dynamic Systemic Compliance and Preload, Such as During Elective AAA Repair
In Vitro Study Comparing CVP Obtained from Central Venous Catheters (CVC’s) and Peripherally Inserted Central Catheters (PICC’s) (2010) [MEDLINE]: in vitro study of AngioDynamics Morpheus Peripherally Inserted Central Catheter (PICC)
Unlike Other Peripherally Inserted Central Catheters (PICC) Models, the Morpheus Peripherally Inserted Central Catheter (PICC) Shaft Has a Stiff Proximal End with a Softer Distal End
The Stiff Proximal End Decreases Intraluminal Resistance, Prevents Compression by Soft Tissues Prior to Vessel Entry, and Prevents Compression of the Catheter in Region of the Subclavian Vein (Which is a Known Compression Site for Vascular Catheters)
AngioDynamics Morpheus Peripherally Inserted Central Catheter (PICC) was Equivalent to Central Venous Catheter (CVC) When Measuring Central Venous Pressure (CVP)
Korean Study Utilizing Peripherally Inserted Central Catheter (PICC) and Central Venous Pressure (CVP) Measurements During Liver Transplantation (2011) [MEDLINE]: study using double-lumen Arrow Peripherally Inserted Central Catheter (PICC)
Peripherally Inserted Central Catheter (PICC was a Viable alternative to Central Venous Catheter (CVC) for Central Venous Pressure (CVP) Measurement During Liver Transplantation
In Vitro and In Vivo Study Comparing Central Venous Pressure (CVP) Obtained from Central Venous Catheter (CVC) and Peripherally Inserted Central Catheter (PICC) (2012) [MEDLINE]: study used triple and double-lumen Bard PowerPICC’s (with high infusion rate capability) vs central venous catheter (CVC) in in vitro (540 pressure measurements) and in vivo (70 pressure measurements) protocols
Peripherally Inserted Central Catheter (PICC) was Equivalent to Central Venous Catheter (CVC) When Measuring Central Venous Pressure (CVP) in Intensive Care Unit (ICU) Patients
Clinical Efficacy-Utility of Central Venous Pressure (CVP) to Assess Volume Status and Volume Responsiveness
Systematic Review of Clinical Utility of Central Venous Pressure (CVP) (Chest, 2008) [MEDLINE]
Systematic Review of 24 Studies (Which Studied Either the Relationship Between Central Venous Pressure (CVP) and Blood Volume or Reported the Associated Between Central Venous Pressure (CVP)/Delta Central Venous Pressure (CVP) and the Change in Stroke Volume/Cardiac Index Following a Fluid Challenge)
There was a Very Poor Relationship Between Central Venous Pressure (CVP) and Blood Volume, as Well as the Inability of Central Venous Pressure (CVP)/Delta Central Venous Pressure (CVP) to Predict the Hemodynamic Response to a Fluid Challenge
Despite Widely-Used Clinical Guidelines Recommending the Use of Central Venous Pressure (CVP), the Central Venous Pressure (CVP) Should Not Be Used to Make Clinical Decisions Regarding Fluid Management
Meta-Analysis of Central Venous Pressure to Predict Fluid Responsiveness (Crit Care Med, 2013) [MEDLINE]: n= 43 studies (healthy adult controls n = 1, intensive care unit patients n = 22, and operating room patients n = 20)
Overall 57% ± 13% of the Patients were Fluid Responders
Summary Area Under the Curve was 0.56 (95% CI: 0.54-0.58) with No Heterogenicity Between the Studies
Summary Area Under the Curve was 0.56 (95% CI: 0.52-0.60) for Those Studies Done in the Intensive Care Unit and 0.56 (95% CI: 0.54-0.58) for Those Studies Done in the Operating Room
Summary Correlation Coefficient Between the Baseline Central Venous Pressure and Change in Stroke Volume Index/Cardiac Index was 0.18 (95% CI: 0.1-0.25), Being 0.28 (95% CI: 0.16-0.40) in the Intensive Care Unit Patients and 0.11 (95% CI: 0.02-0.21) in the Operating Room Patients
There are No Data to Support the Widespread Practice of Using Central Venous Pressure to Guide Fluid Therapy
Systematic Review Examining CVP in Predicting Fluid Responsiveness in Critically Ill Patients (Intensive Care Med, 2016) [MEDLINE]: n = 1148 (51 studies)
Central Venous Pressure (CVP) was Subgrouped into Low (<8 mmHg), Intermediate (8-12 mmHg), High (>12 mmHg) Baseline Central Venous Pressure (CVP)
Although Authors Identified Some Positive and Negative Predictive Values for Fluid Responsiveness for Specific Low and High Values of Central Venous Pressure (CVP), Respectively, None of the Predictive Values were >66% for Any Central Venous Pressure (CVP) from 0 to 20 mm Hg
Central Venous Pressure (CVP) in the Normal Range Does Not Predict Fluid Responsiveness
Recommendations (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE] (Intensive Care Med, 2014) [MEDLINE]
Use of Central Venous Pressure (CVP) Alone to Guide Resuscitation is Not Recommended in Sepsis
Pulmonary Capillary Wedge Pressure (PCWP)
Measurement Technique
PCWP is Measured from the Swan-Ganz Catheter with the Balloon Inflated and “Wedged” in a Pulmonary Artery Branch (see Swan-Ganz Catheter)
By Convention, PCWP is Measured at End-Expiration, Where the Extravascular (i.e. Pleural Pressure) is Zero
Assuming Passive Inspiration/Expiration (Indicated by a Zero Slope of the PCWP Waveform) in a Spontaneously-Breathing Patient, End-Expiration Occurs at the “Peak” of the PCWP Waveform
Assuming Passive Inspiration/Expiration (Indicated by a Zero Slope of the PCWP Waveform) in a Mechanically-Ventilated Patient, End-Expiration Occurs in the “Valley” of the PCWP Waveform (“Vent = Valley”)
In a Patient Who is Actively Expiring, PCWP Waveform Will Have a Positive (Upward) Slope: in this case, it is impossible to determine an accurate PCWP without an esophageal balloon to measure the actual pleural pressure (since pleural pressure is not zero at end-expiration)
Using the Airway Pressure Tracing to Correctly Identify End-Expiration, at Which the Pulmonary Capillary Wedge Pressure Should Be Measured
Study Attempting to Improve Inter-Observer Agreement of PCPW Readings Using Airway Pressure in ARDS (Crit Care Med, 2005) [MEDLINE]
When Using a Standard Protocol Using Airway Pressure to Identify End-Expiration in the Tracing, PCWP Reading Agreement (within 2 mm Hg) Improved from 71% without Use of the Airway Pressure to 83% with Use of the Airway Pressure
Inter-Observer Agreement was Higher for Strips Demonstrating >8 mm Hg in Phasic Respiratory Variation
Correction of Pulmonary Capillary Wedge Pressure Correction for Applied PEEP
Change Units of PEEP to mm Hg by Dividing the Amount by 1.3
Correct by Subtracting 33-50% of PEEP from the PCWP
Left Atrial End-Diastolic Pressure (LA-EDP)
Measurement Technique: measured with (left-sided) cardiac catheterization
Normal: 5-12 mm Hg
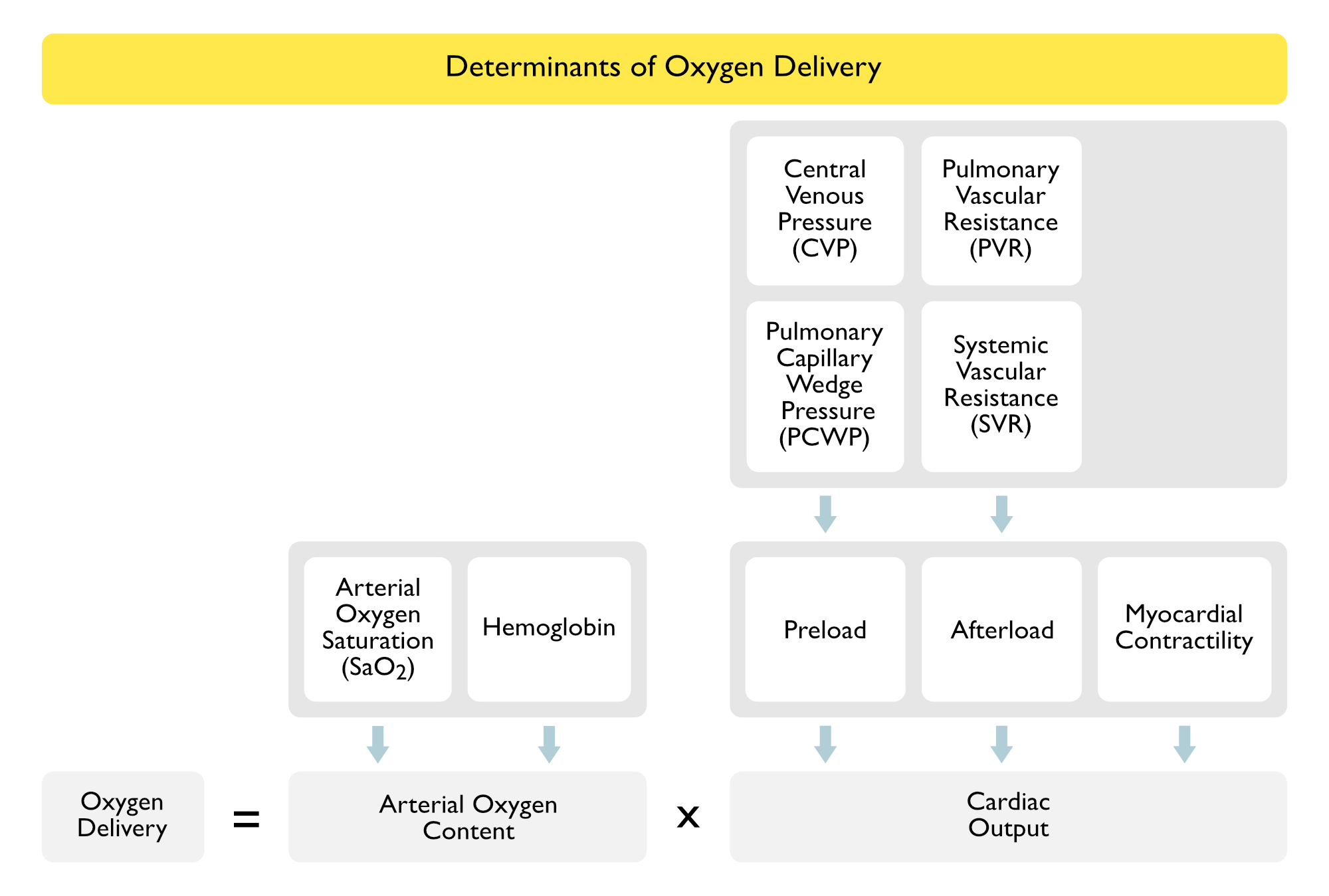
Oxygen Delivery and Consumption
Central Venous O2 Saturation (ScvO2)
General Comments
Source of ScvO2: SaO2 sampled from SVC, with CVC tip above the RA
Normal ScvO2: 65-80% (usually around 70%)
ScvO2 is Usually Slightly Higher Than the SvO2: as ScvO2 is sampled at a point where venous blood from the coronary sinus has not mixed in yet (however, ScvO2 and SvO2 trend together)
Etiology of Increased ScvO2 (Decreased Oxygen Demand or Increased Oxygen Supply)
Cyanide Intoxication (see Cyanide): due to decreased tissue extraction
High pO2
Hypothermia (see Hypothermia): due to decreased tissue metabolic rate
Institute for Healthcare Improvement (IHI) Sepsis Goal-Directed Therapy Targets for ScvO2
Target: ScvO2 >70%
Target: CVP >8 (target: CVP>12 in mechanically ventilated patients and those with increased abdominal pressure)
Target: Hct >30
Mixed Venous O2 Saturation (SvO2)
General Comments
Source of SvO2: SaO2 sampled from Swan-distal port
Normal SvO2: 68-77%
ScvO2 is Usually Slightly Higher Than the SvO2: as ScvO2 is sampled at a point where venous blood from the coronary sinus has not mixed in yet (however, ScvO2 and SvO2 trend together)
Etiology of Increased SvO2 (Decreased Oxygen Demand or Increased Oxygen Supply)
Cyanide Intoxication (see Cyanide): due to decreased tissue extraction
High pO2
Hypothermia (see Hypothermia): due to decreased tissue metabolic rate
Institute for Healthcare Improvement (IHI) Sepsis Goal-Directed Therapy Targets for SvO2
Target: SvO2 >65%
Target: CVP >8 (target: CVP>12 in mechanically ventilated patients and those with increased abdominal pressure)
Target: Hct >30
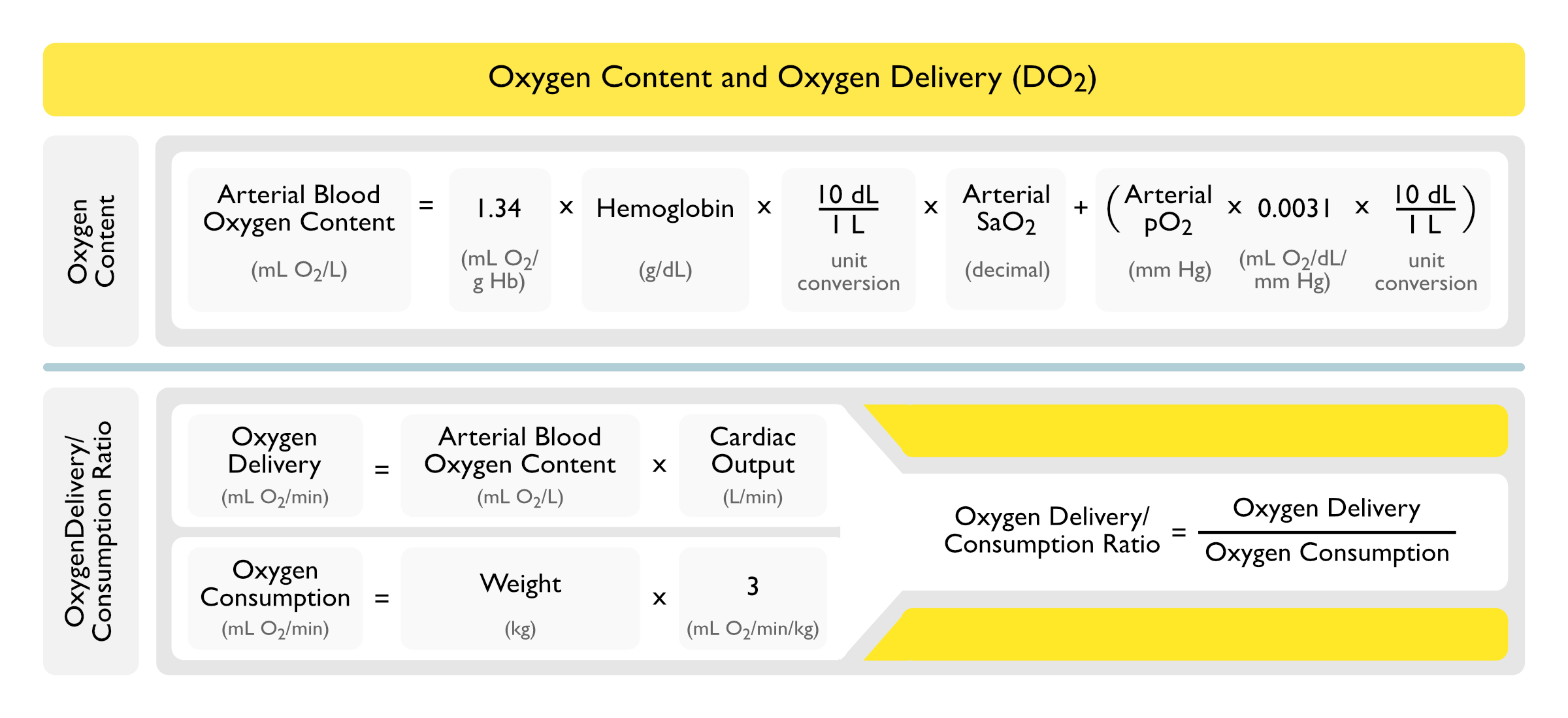
Arterial Oxygen Content
Most of the Oxygen Which Diffuses from the Alveolus into the Blood is Bound by Hemoglobin
The Amount of Oxygen Dissolved in Plasma is Generally Small Relative to the Amount of Oxygen Bound to Hemoglobin, But Becomes Significant at Very High pO2 (as in a Hyperbaric Chamber) or in Severe Anemia
The Constant 0.0031 in the Arterial Oxygen Content Represents the Amount of Oxygen Dissolved in the Plasma
Because this Amount is Relatively Small, the pO2 Term is Commonly Omitted from the Arterial Oxygen Content Equation (as We Do Below)
Under Normal Conditions, Complete Oxygenation of the Blood Occurs in 0.25 sec (This is Approximately One Third of the Total Time that the Blood is in Contact with the Alveolar-Capillary Membrane)
This Rapid Diffusion Normally Allows the System to Sufficiently Compensate for Any Impairment in Oxygen Diffusion
In Dyshemoglobinemias (Such as Sickle Cell Disease, etc), the Arterial Oxygen Content is Calculated with the Same Equation as Below, Although the Saturations (and Therefore, the Oxygen Content) Will Be Different for a Specific pO2 (Pediatr Pulmonol, 1999) [MEDLINE]
Arterial Oxygen Content Equation
Arterial Oxygen Content = [Hb x 13.4 x SaO2 + (0.0031 x pO2)]
Hemoglobin (Hb): in g/dL
Constant 13.4: accounts for the fact that 1.34 ml of O2 is carried per g of Hb (13.4 is used in the equation to correct the units from dL to L)
Arterial Oxygen Saturation (SaO2): as a decimal
pO2: in mm Hg
Normal Arterial Oxygen Content: approximately 200 mL O2/L (or 20 mL O2/dL)
This Equation Will Yield the Arterial Oxygen Content in mL O2/L, Which Allows the Arterial Oxygen Content Value to Be Plugged into the Oxygen Delivery Equation Below without Unit Conversion
Simplified Arterial O2 Content (Omitting the pO2 Term) Arterial O2 Content = [Hb x 13.4 x (SaO2)]
Oxygen Delivery Equation
Definition: rate at which oxygen is transported from the lungs to the tissues
Using a Train Analogy
Hb = number of boxcars
SaO2= how full the boxcars are
CO = how fast the train is going
O2 Delivery = CO x Arterial O2 Content x 10 = CO x [Hb x 1.34 x SaO2] x 10
CO: in L/min
Hb: in g/dL
SaO2: as decimal
Factor of 10 in the Equation Converts Everything to mL
Normal (Using Cardiac Output): 1000 mL/min
Normal (Using Cardiac Index): 500 mL/min/m2
Oxygen Consumption Equation
Oxygen Consumption = CO x [Hb x 1.34 x (SaO2-SvO2)]
Hb: in g/dL
SaO2: as decimal
SvO2: as decimal
Normal (Using Cardiac Output): 250 mL/min
Normal (Using Cardiac Index): 110-130 mL/min/m2
Fick Equation
Fick Cardiac Output = Oxygen Consumption/(10 x Arteriovenous O2 Difference)
Fick Cardiac Output = Oxygen Consumption/(10 x Arterial Oxygen Content – Venous Oxygen Content)
Fick Cardiac Output = 250/[(Hb x 13.4 x SaO2) – (Hb x 13.4 x SvO2)]
Oxygen Consumption: this equation assumes the oxygen consumption is approximately 250 mL/min (or determined by respirometry or a nomogram)
Arteriovenous O2 Difference: in mL O2/dL
Hemoglobin (Hb): in g/dL
Arterial Oxygen Saturation (SaO2): as a decimal
Venous Oxygen Saturation (SaO2): as a decimal
Oxygen Extraction Ratio
Oxygen Extraction Ratio = [O2 Consumption/O2 Delivery] x 100
Normal: 23-32% (interpretation: only 20-30% of oxygen delivered is taken up by tissues)
Etiology of Increased Oxygen Extraction Ratio
Low Cardiac Output State
Cardiogenic Shock
Hypovolemic Shock
Etiology of Decreased Oxygen Extraction Ratio
Sepsis (see Sepsis): due to peripheral shunting and decreased tissue extraction
Hepatopulmonary Syndrome (see Hepatopulmonary Syndrome): due to high CO + low SVR state seen in cirrhosis
Hemodynamic Patterns
High Cardiac Output + Low Systemic Vascular Resistance Pattern (with Normal Pulmonary Capillary Wedge Pressure and Central Venous Pressure)
Conditions with Predominant Peripheral Vascular Effects
Left Heart Failure Pattern = High Central Venous Pressure + High Pulmonary Capillary Wedge Pressure + Low Cardiac Output + Normal Pulmonary Vascular Resistance
Plasma volume expansion in surgical patients with high central venous pressure: the relationship of blood volume to hematocrit, CVP, pulmonary wedge pressure and cardiorespiratory changes. Surg 1975;78:304-315 [MEDLINE]
Critical level of oxygen delivery in anesthetized man. Crit Care Med 1983; 11:640 [MEDLINE]
The effects of dopamine on cardiopulmonary function and left ventricular volumes in patients with acute respiratory failure. Am Rev Respir Dis 1984;130:396-399 [MEDLINE]
Critical level of oxygen delivery after cardiopulmonary bypass. Crit Care Med 1987; 15:194 [MEDLINE]
Measurement of hemoglobin saturation by oxygen in children and adolescents with sickle cell disease. Pediatr Pulmonol. 1999;28(6):423 [MEDLINE]
Human pulmonary vascular response to 4 h of hypercapnia and hypocapnia measured using Doppler echocardiography. J Appl Physiol 2003, 94:1543-1551 [MEDLINE]
Impact of acute hypercapnia and augmented positive end-expiratory pressure on right ventricle function in severe acute respiratory distress syndrome. Intensive Care Med 2009, 35:1850-1858 [MEDLINE]
Pulmonary vascular and right ventricular dysfunction in adult critical care: current and emerging options for management: a systematic literature review. Crit Care. 2010;14(5):R169 [MEDLINE]
Hemodynamic Monitoring for the Evaluation and Treatment of Shock: What Is the Current State of the Art? Semin Respir Crit Care Med. 2015 Dec;36(6):890-8. doi: 10.1055/s-0035-1564874. Epub 2015 Nov 23 [MEDLINE]
Mean Arterial Pressure
Blood pressure measurement in shock. Mechanism of inaccuracy in ausculatory and palpatory methods. JAMA 1967: 199(13):118–122 [MEDLINE]
Arterial catheters as a source of bloodstream infection: a systematic review and meta-analysis. Crit Care Med. 2014 Jun;42(6):1334-9. doi: 10.1097/CCM.0000000000000166 [MEDLINE]
Cardiac Output
Hemodynamic studies in beriberi heart disease. Am J Med. 1966;41(2):197 [MEDLINE]
Echocardiographic LV function in thyrotoxicosis. Am Heart J. 1979;97(4):460 [MEDLINE]
The challenge of cardiomyopathy. J Am Coll Cardiol. 1989;13(6):1219 [MEDLINE]
Metastatic carcinoid disease presenting solely as high-output heart failure. Ann Intern Med. 1994;120(1):45 [MEDLINE]
Thyrotoxicosis-induced congestive heart failure in an urban hospital. Am J Med Sci. 1994;308(6):344 [MEDLINE]
Pathophysiology and treatment of haemodynamic instability in acute pulmonary embolism: the pivotal role of pulmonary vasoconstriction. Cardiovasc Res 2000 Oct;48(1):23-33 [MEDLINE]
Thyroid hormone and the cardiovascular system. N Engl J Med. 2001;344(7):501 [MEDLINE]
Cardiovascular abnormalities in patients with a carcinoid syndrome. Neth J Med. 2002 Mar;60(1):10-6 [MEDLINE]
Hyperthyroidism: a “curable” cause of congestive heart failure–three case reports and a review of the literature. Congest Heart Fail. 2003;9(1):40 [MEDLINE]
Echocardiographic detection of intrapulmonary shunting in a patient with hepatopulmonary syndrome: case report and review of the literature. Echocardiography. 2006;23(1):56 [MEDLINE]
Incidence, clinical characteristics and outcome of congestive heart failure as the initial presentation in patients with primary hyperthyroidism. Heart. 2007;93(4):483 [MEDLINE]
Mechanisms in endocrinology: Heart failure and thyroid dysfunction. Eur J Endocrinol. 2012 Nov;167(5):609-18 [MEDLINE]
Diet-induced obesity promotes altered remodeling and exacerbated cardiac hypertrophy following pressure overload. Physiol Rep. 2015;3(8) [MEDLINE]
High-Output Heart Failure: A 15-Year Experience. J Am Coll Cardiol. 2016;68(5):473 [MEDLINE]
Hyperdynamic Right Heart Function in Graves’ Hyperthyroidism Measured by Echocardiography Normalises on Restoration of Euthyroidism. Heart Lung Circ. 2017;26(6):580 [MEDLINE]
Leptin-Aldosterone-Neprilysin Axis: Identification of Its Distinctive Role in the Pathogenesis of the Three Phenotypes of Heart Failure in People With Obesity. Circulation. 2018;137(15):1614 [MEDLINE]
Acute Right Ventricular Heart Failure: An Uncommon Case of Thyrotoxicosis. Am J Med Sci. 2018;356(3):309 [MEDLINE]
Pulmonary Capillary Wedge Pressure
Effect of airway pressure display on interobserver agreement in the assessment of vascular pressures in patients with acute lung injury and acute respiratory distress syndrome. Crit Care Med. 2005 Jan;33(1):98-103; discussion 243-4 [MEDLINE]
Central Venous Pressure (CVP)
Central venous pressure measurements: peripherally inserted catheters versus centrally inserted catheters. Crit Care Med. 2000 Dec;28(12):3833-6 [MEDLINE]
Intraoperative peripherally inserted central venous catheter central venous pressure monitoring in abdominal aortic aneurysm reconstruction. Ann Vasc Surg. 2006 Sep;20(5):577-81. Epub 2006 Jul 27 [MEDLINE]
Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest. 2008 Jul;134(1):172-8. doi: 10.1378/chest.07-2331 [MEDLINE]
An in vitro study comparing a peripherally inserted central catheter to a conventional central venous catheter: no difference in static and dynamic pressure transmission. BMC Anesthesiol. 2010 Oct 12;10:18. doi: 10.1186/1471-2253-10-18 [MEDLINE]
Comparison of the central venous pressure from internal jugular vein and the pressure measured from the peripherally inserted antecubital central catheter (PICCP) in liver transplantation recipients. Korean J Anesthesiol. Oct 2011; 61(4): 281–287. Published online Oct 22, 2011. doi: 10.4097/kjae.2011.61.4.281 [MEDLINE]
Peripherally inserted central catheters are equivalent to centrally inserted catheters in intensive care unit patients for central venous pressure monitoring. J Clin Monit Comput. 2012 Apr;26(2):85-90. doi: 10.1007/s10877-012-9337-1 [MEDLINE]
Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med 2014; 40(12):1795–1815 [MEDLINE]
Systematic review including re‐analyses of 1148 individual data sets of central venous pressure as a predictor of fluid responsiveness. Intensive Care Med 2016, 42(3):324–332 [MEDLINE]
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017 Jan 18. doi: 10.1007/s00134-017-4683-6 [MEDLINE]
Ultrasound
The respiratory variation in inferior vena cava diameter as a guide to fluid therapy. Intensive Care Med. 2004 Sep;30(9):1834-7. Epub 2004 Mar 25 [MEDLINE]
Bedside ultrasonography for the intensivist. Crit Care Clin. 2015 Jan;31(1):43-66. doi: 10.1016/j.ccc.2014.08.003. Epub 2014 Oct 3 [MEDLINE]